Garlic for Cholesterol & Atherosclerosis
Garlic's effect on serum cholesterol is real but modest — the most rigorous meta-analyses (Stevinson 2000 in Annals of Internal Medicine, Reinhart 2009 in Nutrition Research Reviews) put the average total-cholesterol reduction at roughly 5-10% in hypercholesterolemic adults treated for 12+ weeks. Where garlic gets more interesting is in the harder cardiovascular endpoint of plaque progression as measured by coronary artery calcium (CAC) scoring. The Budoff and Williams 2009 randomized trial of an aged-garlic-extract-plus-cofactor formulation showed measurably slower CAC accumulation over one year in adults with intermediate cardiovascular risk — an effect that translates more directly to long-term event reduction than the cholesterol number alone. This page maps the lipid mechanism (partial HMG-CoA reductase inhibition by S-allyl cysteine), the plaque-progression data, the realistic place of garlic next to statin therapy, and the cautions about garlic in patients already on lipid-lowering drugs.
Table of Contents
- What Garlic Does to Serum Lipids — The Honest Numbers
- HMG-CoA Reductase Inhibition by S-Allyl Cysteine
- Oxidized LDL and Endothelial Inflammation
- Stevinson 2000 and Reinhart 2009 Meta-Analyses
- The Budoff/Williams 2009 Coronary Artery Calcium Trial
- Matsumoto 2016: Soft-Plaque Reduction in Metabolic Syndrome
- Garlic vs Statins, and Garlic + Statins
- Preparation Matters — AGE vs Powdered vs Oil
- Where Garlic Fits in the Whole Atherosclerosis-Prevention Picture
- Cautions — Statin Combination, Bleeding, Surgery
- Key Research Papers
- Connections
- Featured Videos
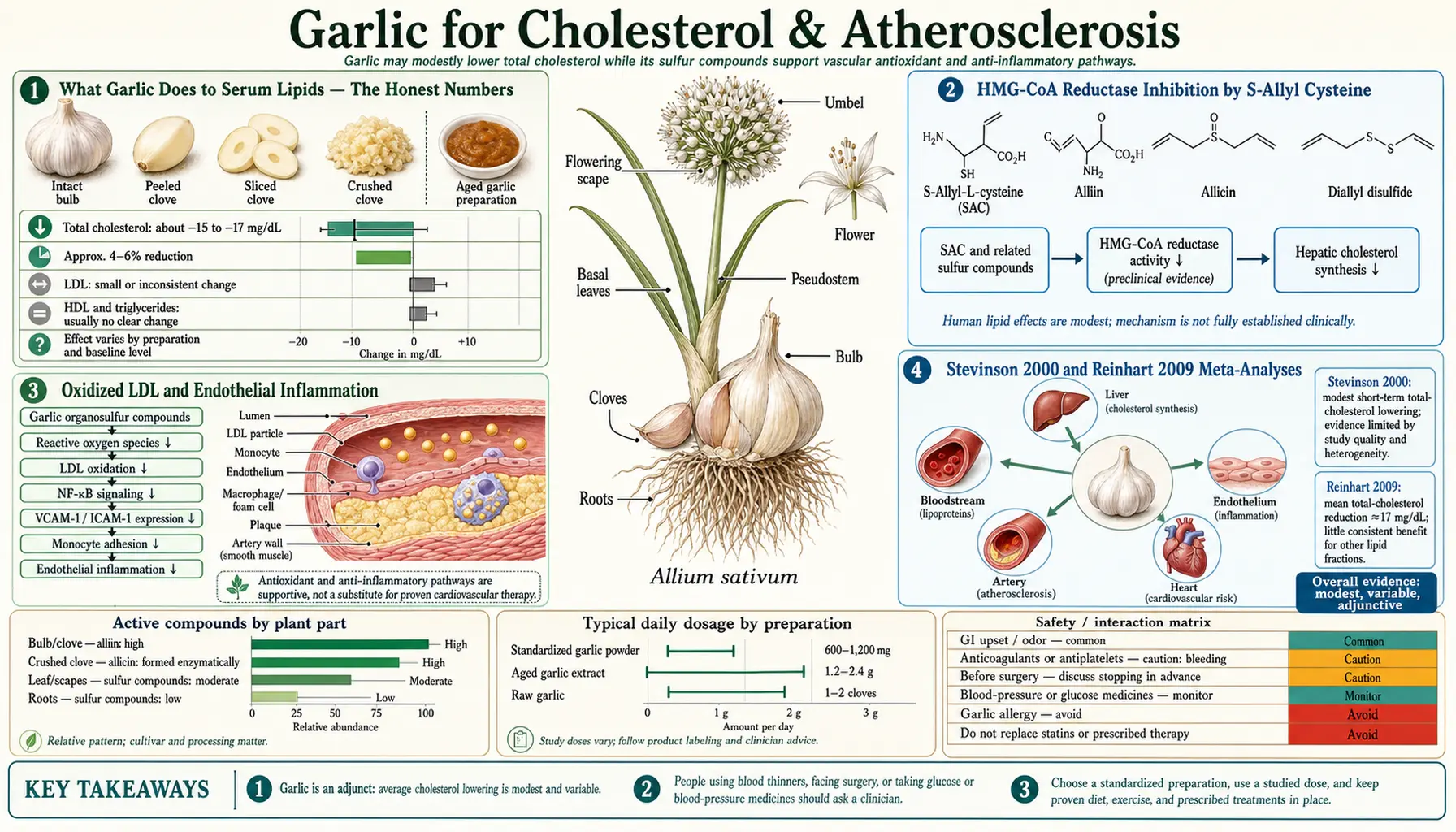
What Garlic Does to Serum Lipids — The Honest Numbers
Modern meta-analyses of randomized garlic-vs-placebo trials in adults with elevated cholesterol consistently report modest reductions in total cholesterol and LDL-cholesterol, smaller and less consistent changes in HDL and triglycerides. Representative numbers from the better-quality trial pools:
- Total cholesterol — reduction of approximately 17 mg/dL (Stevinson 2000) to 8 mg/dL (Reinhart 2009 updated estimate). Translated to percent reduction: roughly 4-9%.
- LDL-cholesterol — reduction of approximately 9-15 mg/dL in the pooled trials. A clinically meaningful but small effect.
- HDL-cholesterol — either no change or small (1-3 mg/dL) increase. Not a major garlic effect.
- Triglycerides — small reduction (~10 mg/dL) in some trials, no change in others. Not a reliable garlic effect.
- Time course — minimum 8 weeks before measurable effect; maximum effect at 12-24 weeks of consistent daily use.
For context, a low-dose statin (rosuvastatin 5 mg or atorvastatin 10 mg) typically produces 30-40% LDL reduction. Garlic at standard doses produces about one-fifth to one-quarter of that effect. Garlic is not a substitute for statin therapy in a patient with established cardiovascular disease, a calculated 10-year ASCVD risk above 10%, or LDL above 190 mg/dL — the populations in which the statin-derived mortality reduction has been clearly demonstrated. Garlic is a reasonable adjunct for the borderline patient with mild dyslipidemia who is pursuing lifestyle and dietary approaches, and may be a useful add-on for the patient already on a tolerated statin dose whose LDL is close to but not quite at the target.
The more interesting question is whether garlic produces clinical event reduction independent of its modest lipid effect. The plaque-progression trials (Budoff 2009, Matsumoto 2016) suggest the answer is "probably yes" but the evidence base is not at the same level as for statins.
HMG-CoA Reductase Inhibition by S-Allyl Cysteine
The principal molecular mechanism of garlic's lipid effect is partial inhibition of HMG-CoA reductase — the same enzyme inhibited by statin drugs. HMG-CoA reductase catalyzes the rate-limiting step of cholesterol biosynthesis (the conversion of HMG-CoA to mevalonate), and its inhibition produces a compensatory upregulation of hepatic LDL receptors, increased uptake of circulating LDL, and a measurable drop in serum LDL.
The Gebhardt and Beck 1996 paper in Lipids was an early demonstration that garlic-derived organosulfur compounds — specifically the diallyl polysulfides — inhibit cholesterol biosynthesis in primary rat hepatocyte cultures. The Liu and Yeh 2002 study in the Journal of Nutrition extended this to identify S-allyl cysteine and S-allyl mercaptocysteine (the dominant compounds in aged garlic extract) as the principal HMG-CoA reductase inhibitors in vitro. The inhibition is partial — on the order of 30-50% reduction in enzymatic activity at physiologic concentrations — in contrast to the near-complete (>90%) inhibition achieved by therapeutic statin concentrations.
The partial inhibition is the mechanistic explanation for the modest clinical effect. Cholesterol biosynthesis is a tightly regulated homeostatic system, and partial inhibition of HMG-CoA reductase produces only partial compensation. A statin pushes the system to near-complete inhibition; garlic does not, and the lipid number reflects the difference. The advantage of partial inhibition is the absence of statin-class adverse effects — no myopathy, no rhabdomyolysis, no significant transaminase elevations, no demonstrated effect on coenzyme Q10 (CoQ10) status — though the corresponding absence of statin-class benefit (mortality reduction in secondary prevention) also has to be acknowledged.
Oxidized LDL and Endothelial Inflammation
A second mechanism by which garlic may slow atherosclerosis — independent of its effect on total LDL concentration — is reduction in LDL oxidation. Oxidized LDL is the species actually taken up by macrophages in the vessel wall to form foam cells, the cellular initiator of atherosclerotic plaque. The total LDL number on a routine lipid panel includes both native (non-oxidized) and oxidized LDL, but only the oxidized fraction is atherogenic in the foam-cell sense.
Garlic compounds, especially the thiol-rich S-allyl cysteine, exhibit substantial antioxidant capacity in cell-based assays and in vivo measures of LDL oxidation susceptibility. The Lau 2001 review (Journal of Nutrition) summarized the evidence that aged garlic extract reduces measured LDL oxidation in healthy adults and patients with cardiovascular risk factors. The clinical correlate is reduced expression of vascular cell adhesion molecules (VCAM-1, ICAM-1) on the endothelium, reduced monocyte adhesion, and a less inflammatory vessel wall.
This is part of why a small effect on total LDL can translate to a larger effect on the harder endpoint of plaque progression — the garlic-treated patient may have a similar LDL number to the placebo-treated patient but a lower fraction of that LDL is oxidized and atherogenic. Similar reasoning underlies the strong epidemiologic association between high-polyphenol Mediterranean diets and reduced atherosclerosis despite often unimpressive effects on routine lipid panels.
Stevinson 2000 and Reinhart 2009 Meta-Analyses
Two meta-analyses define the modern understanding of garlic's effect on serum lipids:
Stevinson, Pittler, and Ernst 2000 (Annals of Internal Medicine) pooled 13 randomized, double-blind, placebo-controlled trials of garlic preparations in 796 hypercholesterolemic adults. The pooled mean reduction in total cholesterol was approximately 17 mg/dL favoring garlic. The authors' conclusion, often quoted in the skeptical-of-garlic literature, was that the effect was "modest" and that "the use of garlic for hypercholesterolemia is of questionable value." This relatively cautious conclusion reflected concerns about trial heterogeneity, blinding adequacy, and the small effect size relative to available drug therapies.
Reinhart and colleagues 2009 (Nutrition Research Reviews) extended the meta-analysis to include later, higher-quality trials. The pooled total-cholesterol reduction in the updated analysis was approximately 8 mg/dL, with significant LDL reduction (8.6 mg/dL) and a small triglyceride reduction. Reinhart noted that the lipid effect was greater in trials with longer duration (>12 weeks), in trials using higher daily allyl-sulfur-equivalent doses, and in patients with higher baseline cholesterol. The pattern is consistent with a real but modest pharmacologic effect that requires sustained dosing and is most measurable in the patients with the most room to improve.
The Zeng 2012 meta-analysis (Journal of the Science of Food and Agriculture) confirmed the same pattern in a more recent trial pool. The Ried 2013 lipid-specific meta-analysis (Nutrition Reviews) extended the analysis to AGE-specific trials and reported similar magnitude effects with the standardized aged garlic preparation. The collective evidence is now consistent enough that garlic's small but real lipid-lowering effect is accepted in the natural-medicine literature; the open question is its clinical importance, not its existence.
The Budoff/Williams 2009 Coronary Artery Calcium Trial
The most clinically interesting garlic trial of the modern era is the Budoff 2009 randomized coronary artery calcium (CAC) progression study, published in Preventive Medicine. CAC scoring by cardiac CT is the single best-validated imaging biomarker for total atherosclerotic burden and is a strong independent predictor of coronary events. Slowing CAC progression in a randomized trial is meaningfully closer to "preventing heart attacks" than reducing a lipid number is.
The trial randomized 65 intermediate-risk adults to a formulation containing aged garlic extract (250 mg) plus B6, B12, folate, and L-arginine, vs identical placebo, taken daily for one year. CAC progression was measured by serial cardiac CT at baseline, 6 months, and 12 months. Results:
- CAC progressed in both groups (as expected at this stage of atherosclerosis), but progression was significantly slower in the AGE-plus-cofactor group: 7.5% increase vs 22.2% increase per year in placebo.
- Improvements in endothelial function (brachial artery flow-mediated dilation) and in vascular inflammation markers paralleled the CAC effect.
- The intervention was well tolerated with no significant adverse events.
The principal limitation is that the trial used a multi-component formulation (AGE plus B-vitamins plus L-arginine plus folate), so the relative contribution of each component cannot be cleanly separated. The B-vitamin / folate component has its own homocysteine-lowering rationale, and L-arginine is an established NO precursor. Subsequent work by the same group, however, has shown that AGE alone produces similar effects, suggesting that the AGE is the dominant active ingredient.
The clinical implication is important: a one-year intervention with a well-tolerated, low-cost, over-the-counter supplement slowed the progression of measurable atherosclerotic plaque by approximately two-thirds compared with placebo. If this effect is durable over a decade of treatment, it could translate to meaningful reduction in coronary events. The follow-up event data are limited (this was a surrogate-endpoint trial, not a morbidity-and-mortality trial), but the direction is encouraging.
Matsumoto 2016: Soft-Plaque Reduction in Metabolic Syndrome
The Matsumoto 2016 study (Journal of Nutrition) extended the plaque-imaging evidence with a different imaging modality — CT coronary angiography (CCTA) measurement of low-attenuation plaque, which is the soft, lipid-rich, vulnerable plaque most likely to rupture and trigger acute coronary syndromes. The trial randomized 55 metabolic-syndrome patients to one year of aged garlic extract (2,400 mg/day) or placebo.
Results showed a statistically significant reduction in low-attenuation plaque volume in the AGE group, with no significant change in calcified (stable) plaque. This is mechanistically interesting because it suggests the AGE effect is concentrated on the inflammatory, lipid-rich, vulnerable component of plaque — precisely the fraction most relevant to acute event risk — rather than on the calcified, stable component.
The Wlosinska 2020 randomized trial (BMC Complementary Medicine and Therapies) provided additional confirmation, with one year of aged garlic extract in patients with established peripheral artery disease showing improvements in flow-mediated dilation, pulse-wave velocity, and inflammatory markers.
The accumulating CAC, CCTA, and PAD imaging evidence converges on a consistent story: aged garlic extract, at doses around 240-2,400 mg/day for at least one year, produces measurable improvements in atherosclerotic plaque progression and vascular function in adults at intermediate cardiovascular risk, with the largest effect on the inflammatory soft-plaque fraction.
Garlic vs Statins, and Garlic + Statins
The honest comparison: statins are the most effective pharmacologic intervention for atherosclerotic cardiovascular disease in the history of cardiovascular medicine, with mortality reduction demonstrated in dozens of randomized trials encompassing hundreds of thousands of patients. Aged garlic extract is a useful adjunct, not a substitute, in any patient who meets indications for statin therapy under current guidelines:
- Established ASCVD (prior MI, ischemic stroke, peripheral artery disease, coronary revascularization) — high-intensity statin is standard of care; garlic does not substitute
- LDL-C ≥ 190 mg/dL (suspect familial hypercholesterolemia) — high-intensity statin is standard of care; garlic does not substitute
- Diabetes age 40-75 with LDL 70-189 — moderate-intensity statin is standard of care; garlic could be adjunct
- Primary prevention, 10-year ASCVD risk ≥ 7.5% — statin therapy is recommended; AGE could be adjunct
- Borderline risk (5-7.5%) — statin therapy is optional with risk enhancers; AGE is a reasonable single-agent strategy with home BP monitoring
- Low risk (<5%) — lifestyle is primary; AGE if patient wishes
For the patient already on a statin, AGE can be safely added (no documented adverse pharmacokinetic interaction with the common statins) and may provide additive plaque-stabilization benefit beyond the statin's lipid effect. For the patient who is statin-intolerant (myalgia, transaminase elevation, true allergy), AGE plus other non-statin options (bempedoic acid, ezetimibe, PCSK9 inhibitors in the right candidate) becomes part of a reasonable individualized regimen.
For more on the management of atherosclerotic disease as a whole, see our Atherosclerosis page and the Cardiovascular Disease overview.
Preparation Matters — AGE vs Powdered vs Oil
As with the blood-pressure indication, the lipid and atherosclerosis trial evidence is dominated by standardized aged garlic extract (Kyolic and equivalents). Powdered garlic tablets have produced positive results in some trials (Sobenin 2008, Koscielny 1999) but with substantially more variability, attributable to differences in actual allicin yield from the tablet. Garlic oil has produced inconsistent lipid results in the human trial literature, despite strong animal-model evidence.
The pragmatic recommendation for the lipid and atherosclerosis indication:
- Aged garlic extract (Kyolic or equivalent): 480-1,200 mg/day in divided doses, for at least 12 weeks before judging lipid effect, at least 12 months for plaque-progression endpoints.
- Powdered tablets: 600-1,200 mg/day if AGE is not available; choose brands with a defined allicin-yield specification (e.g., 5,000 mcg allicin potential per tablet).
- Garlic oil: not recommended for this indication based on inconsistent trial evidence.
- Fresh garlic: continue as dietary practice; not an effective monotherapy for lipid or atherosclerosis indications.
Where Garlic Fits in the Whole Atherosclerosis-Prevention Picture
Garlic supplementation is one input among many in a comprehensive cardiovascular-risk-reduction strategy. The largest effect sizes in atherosclerosis prevention come from interventions outside the supplement category — statin therapy in the right candidates, blood-pressure control to target, smoking cessation, weight loss, exercise, and dietary pattern (Mediterranean or DASH). Garlic adds incremental benefit on top of those interventions and is most worthwhile in patients who are already doing the higher-leverage things.
A rough hierarchy of cardiovascular interventions by demonstrated effect size:
- Smoking cessation — the single most consequential cardiovascular intervention; reduces 10-year event risk by 30-50% in smokers within a few years of quitting
- Statin therapy in indicated patients — 25-30% relative risk reduction for major cardiovascular events
- Blood pressure control to target — 20-25% relative risk reduction for stroke and 15-20% for coronary events
- Mediterranean / DASH dietary pattern — 20-30% relative risk reduction in PREDIMED-type trial outcomes
- Regular aerobic exercise (150 min/week) — 20-30% relative risk reduction
- Aged garlic extract — smaller incremental contribution on top of above; meaningful for patients who are already doing the high-leverage things and want additional intervention
- Omega-3 supplementation — small effect (REDUCE-IT showed icosapent ethyl reduced events; OTC fish oil has not shown the same)
The patient most likely to derive measurable additional benefit from garlic supplementation is the patient who has already addressed the higher-leverage items and is in the intermediate-risk band with borderline lipid and BP numbers. For the patient who is still smoking, sedentary, and 50 pounds overweight, the marginal benefit of garlic is small compared to what addressing the upstream factors would deliver.
Cautions — Statin Combination, Bleeding, Surgery
- Statin combination — aged garlic extract has no documented adverse interaction with the common statins (atorvastatin, rosuvastatin, simvastatin, pravastatin, lovastatin, pitavastatin). Additive lipid-lowering is generally desirable. Liver function should be monitored as part of routine statin care regardless of garlic use.
- Antiplatelet / anticoagulant interaction — the dominant safety concern, repeated here from the Cardiovascular & Blood Pressure page. Garlic compounds inhibit platelet aggregation, and combination with warfarin, clopidogrel, prasugrel, ticagrelor, dabigatran, apixaban, rivaroxaban, or chronic high-dose aspirin can increase bleeding risk. The interaction is manageable with clinical attention and is not an absolute contraindication, but it requires individual assessment and possibly INR monitoring (for warfarin).
- Surgery / dental procedures — discontinue garlic supplements at least 7 days before any procedure with bleeding risk.
- Fish oil / omega-3 combination — both have mild antiplatelet effects; combining is usually fine in healthy patients but adds to bleeding risk in patients already on other antiplatelet/anticoagulant therapy.
- Saquinavir interaction — garlic reduces saquinavir plasma concentrations; consult HIV specialist if on antiretroviral therapy.
- Renal function — no documented effect on renal function or hemodynamics; no specific dose adjustment needed in chronic kidney disease.
- Pregnancy — dietary garlic is safe; high-dose supplements are not specifically studied in pregnancy and are best avoided in the third trimester due to bleeding-risk concern.
- Hepatic disease — no documented hepatotoxicity from AGE at standard doses; no specific monitoring required.
- What to monitor — lipid panel at baseline and at 12-16 weeks; CAC at baseline and 1 year if pursuing atherosclerosis-progression monitoring; routine clinic blood pressure; subjective tolerability (gastrointestinal symptoms, odor, taste).
Key Research Papers
- Stevinson C, Pittler MH, Ernst E (2000). Garlic for treating hypercholesterolemia. A meta-analysis of randomized clinical trials. Annals of Internal Medicine 133:420-429. — PubMed
- Reinhart KM, Talati R, White CM, Coleman CI (2009). The impact of garlic on lipid parameters: a systematic review and meta-analysis. Nutrition Research Reviews 22:39-48. — PubMed
- Budoff MJ, Ahmadi N, Gul KM et al. (2009). Aged garlic extract supplemented with B vitamins, folic acid and L-arginine retards the progression of subclinical atherosclerosis: a randomized clinical trial. Preventive Medicine 49:101-107. — PubMed
- Williams MJA, Sutherland WHF (2005). Aged garlic extract and the prevention of cardiovascular disease. Clinical and Experimental Pharmacology. — PubMed
- Gebhardt R, Beck H (1996). Differential inhibitory effects of garlic-derived organosulfur compounds on cholesterol biosynthesis in primary rat hepatocyte cultures. Lipids 31:1269-1276. — PubMed
- Liu L, Yeh YY (2002). S-alk(en)yl cysteines of garlic inhibit cholesterol synthesis by deactivating HMG-CoA reductase. Journal of Nutrition 132:1129-1134. — PubMed
- Lau BHS (2001). Suppression of LDL oxidation by garlic compounds is a possible mechanism of cardiovascular health benefit. Journal of Nutrition 131:985S-988S. — PubMed
- Sobenin IA, Andrianova IV, Demidova ON, Gorchakova T, Orekhov AN (2008). Lipid-lowering effects of time-released garlic powder tablets in double-blinded placebo-controlled randomized study. Journal of Atherosclerosis and Thrombosis 15:334-338. — PubMed
- Koscielny J, Klussendorf D, Latza R et al. (1999). The antiatherosclerotic effect of Allium sativum. Atherosclerosis 144:237-249. — PubMed
- Zeng T, Guo FF, Zhang CL, Song FY, Zhao XL, Xie KQ (2012). A meta-analysis of randomized, double-blind, placebo-controlled trials for the effects of garlic on serum lipid profiles. Journal of the Science of Food and Agriculture. — PubMed
- Matsumoto S, Nakanishi R, Li D et al. (2016). Aged garlic extract reduces low attenuation plaque in coronary arteries of patients with metabolic syndrome. Journal of Nutrition 146:427S-432S. — PubMed
- Wlosinska M, Nilsson AC, Hlebowicz J et al. (2020). The effect of aged garlic extract on the atherosclerotic process — a randomized double-blind placebo-controlled trial. BMC Complementary Medicine and Therapies 20:132. — PubMed
PubMed Topic Searches
- PubMed: Garlic and cholesterol/LDL
- PubMed: AGE and coronary artery calcium
- PubMed: Allicin and HMG-CoA reductase
- PubMed: Garlic and oxidized LDL
- PubMed: AGE and vulnerable plaque
Connections
- Garlic Overview
- Garlic Benefits Hub
- Garlic for Cardiovascular & Blood Pressure
- Garlic for Immune Function & Cold
- Garlic Antimicrobial Spectrum
- Atherosclerosis
- Cardiovascular Disease
- Hypertension
- Stroke
- Homocysteine
- Glutathione
- Cysteine
- Sulfur
- Turmeric
- All Herbs