Garlic Antimicrobial Spectrum — Allicin, MRSA, H. pylori, Candida, Parasites
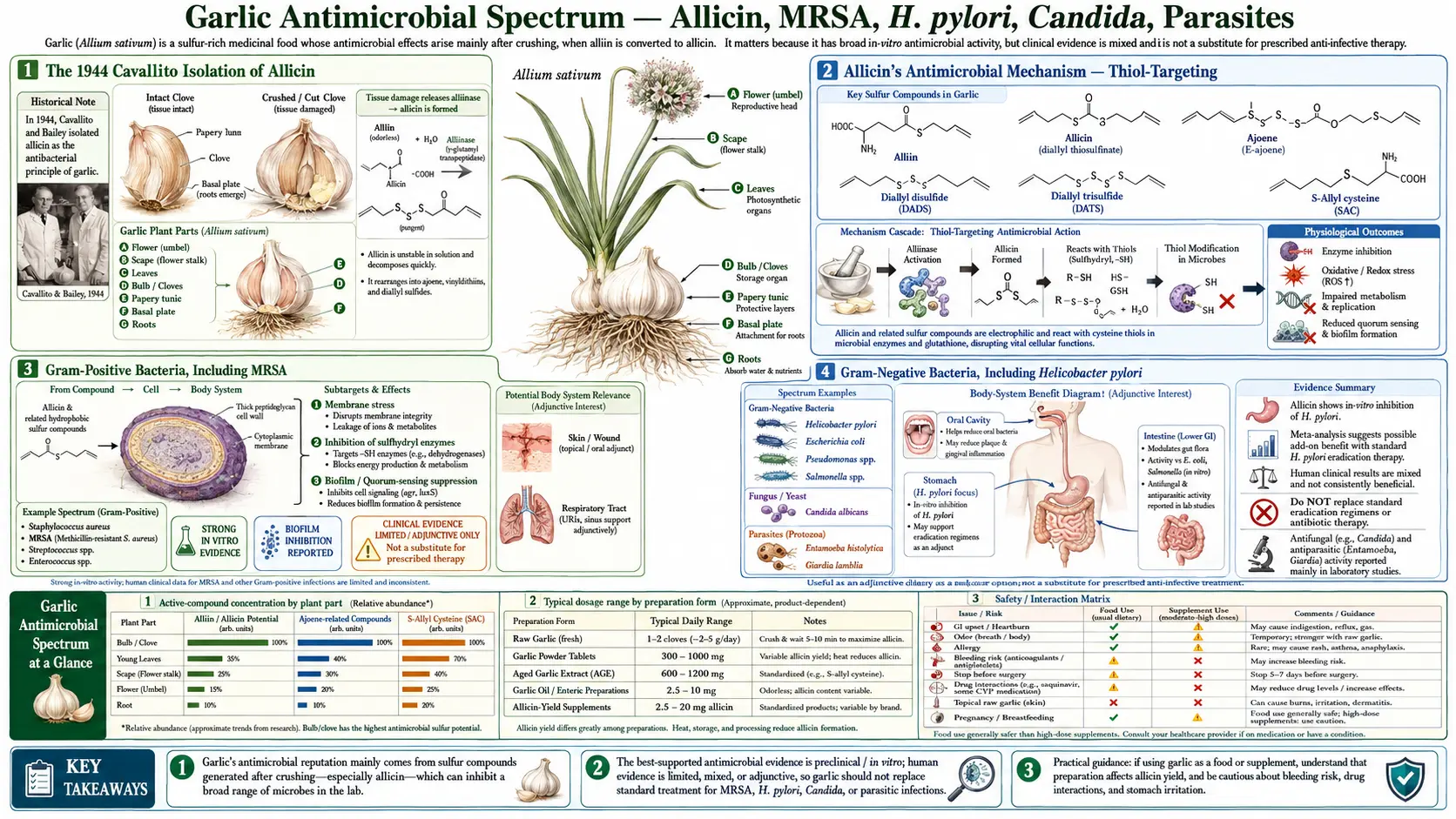
Allicin is the small-molecule antibiotic that Chester Cavallito and John Bailey isolated from crushed garlic in 1944 and characterized in a series of Journal of the American Chemical Society papers that established it as the molecule responsible for garlic's well-known antibacterial activity. Cavallito's pure allicin had broad-spectrum activity against Gram-positive and Gram-negative bacteria including Staphylococcus aureus, Escherichia coli, Salmonella enterica, and Shigella dysenteriae, with minimum inhibitory concentrations comparable to penicillin against susceptible organisms — remarkable performance for a plant-derived compound discovered in the same era as the early antibiotics. Eight decades later, allicin has not become a clinical antibiotic, primarily because it is too unstable for systemic pharmaceutical formulation. But the antimicrobial breadth has been confirmed against modern targets including methicillin-resistant Staphylococcus aureus (MRSA), Helicobacter pylori (where garlic has a documented adjunctive role in eradication therapy), Candida albicans and other fungi, and several enteric parasites including Giardia lamblia. This page maps the spectrum, the mechanism (thiol-targeting via cysteine residue oxidation), and the realistic place of garlic alongside — not as a substitute for — modern antimicrobial therapy.
Table of Contents
- The 1944 Cavallito Isolation of Allicin
- Allicin's Antimicrobial Mechanism — Thiol-Targeting
- Gram-Positive Bacteria, Including MRSA
- Gram-Negative Bacteria, Including Helicobacter pylori
- Antifungal Spectrum — Candida and Beyond
- Antiparasitic Activity — Giardia, Entamoeba, Others
- Garlic as Adjunctive Therapy in H. pylori Eradication
- Topical Uses — Skin, Ear, Vaginal Considerations
- Why Allicin Is Not a Clinical Antibiotic
- Cautions — What Garlic Is Not For
- Key Research Papers
- Connections
- Featured Videos
The 1944 Cavallito Isolation of Allicin
The systematic biochemistry of garlic's antibacterial activity begins with Chester J. Cavallito and John Hays Bailey's 1944 paper in the Journal of the American Chemical Society: "Allicin, the antibacterial principle of Allium sativum. I. Isolation, physical properties and antibacterial action." Cavallito, working at the Sterling-Winthrop Research Institute, was attempting to characterize the long-observed but mechanistically obscure antibacterial activity of crushed garlic. He successfully isolated a pure compound from steam-distilled crushed garlic that exhibited the full antibacterial activity of the parent extract, determined its empirical formula, and named it allicin (a contraction of Allium).
Cavallito's 1944 papers and the immediate follow-ups characterized:
- Structure — diallyl thiosulfinate (CH2=CH-CH2-S(=O)-S-CH2-CH=CH2), an unusual sulfenyl sulfide
- Stability — allicin decomposes in aqueous solution at room temperature with a half-life of hours, and in cooking oil at sauteing temperatures within seconds
- Antibacterial spectrum — activity against Staphylococcus aureus, Streptococcus species, Bacillus, Escherichia coli, Salmonella enterica (typhi), Shigella dysenteriae, Vibrio cholerae, and other organisms, with minimum inhibitory concentrations in the low μg/mL range
- Comparison with penicillin — allicin's MIC against susceptible S. aureus was comparable to penicillin in vitro, although potency varied with bacterial species
- Mechanistic observations — activity was rapidly destroyed by reducing agents (glutathione, cysteine), implicating a thiol-targeting mechanism even in the pre-modern-biochemistry era
The historical context matters: the 1944 publication came at the dawn of the modern antibiotic era. Penicillin was just being scaled for wartime use; streptomycin was a year away; the era of chemically synthesized antibiotics (sulfonamides, chloramphenicol) was just beginning. Garlic-derived allicin was a serious candidate at the time. The chemical instability and pharmacokinetic challenges that have prevented its development as a clinical antibiotic became apparent only with subsequent attempts at systemic formulation.
Allicin's Antimicrobial Mechanism — Thiol-Targeting
The molecular mechanism of allicin's antimicrobial activity is well understood and unusual. Allicin contains the reactive thiosulfinate group, which is a potent electrophilic oxidizer of free cysteine thiol groups in proteins. When allicin encounters a microbial protein containing an exposed cysteine residue, the thiosulfinate sulfur reacts with the cysteine sulfhydryl to form a mixed S-allyl-S-protein disulfide bond, modifying the protein's structure and inactivating its function.
This thiol-targeting mechanism is broad in two senses:
- Many essential microbial enzymes contain catalytic cysteine residues — including thiol-dependent dehydrogenases, RNA polymerase, DNA gyrase, and the cysteine proteases. Targeting these enzymes simultaneously creates pleiotropic disruption of bacterial metabolism that is difficult to evolve resistance against, in contrast to single-target antibiotics where a single point mutation can confer resistance.
- The reactive sulfur chemistry is conserved across phylogenetic kingdoms — bacterial, fungal, and parasite proteins all use cysteine residues in catalytic and structural roles, which is why allicin has activity against organisms across very different taxonomic groups.
The Ankri and Mirelman 1999 review in Microbes and Infection provides the canonical mechanistic synthesis. The same thiol reactivity that makes allicin a broad-spectrum antimicrobial also makes it short-lived in vivo: it is rapidly inactivated by the host's own thiol pool (glutathione, free cysteine), which means systemic exposure of pathogens to active allicin from oral garlic is minimal after first-pass thiol scavenging. This is the principal reason allicin does not work systemically the way it works in vitro.
The follow-on compounds — diallyl polysulfides (DAS, DADS, DATS) — have somewhat different reactivity profiles. They are less acutely reactive than allicin but more lipid-soluble and longer-lived, accumulating in tissues over hours to days with sustained intake. They also exhibit antimicrobial activity but through somewhat different mechanisms including disruption of bacterial membrane integrity and induction of host antimicrobial peptides.
Gram-Positive Bacteria, Including MRSA
Allicin has consistently strong in vitro activity against Gram-positive pathogens, including the drug-resistant strains that are a major modern problem. The Cutler and Wilson 2004 study in British Journal of Biomedical Science tested a stable aqueous allicin extract against 30 clinical isolates of methicillin-resistant Staphylococcus aureus (MRSA) and reported minimum inhibitory concentrations in the 8-64 μg/mL range — clinically meaningful in vitro activity that included strains resistant to vancomycin and mupirocin.
Subsequent in vitro and small clinical studies have explored topical allicin formulations for MRSA decolonization of the nares and skin, with some encouraging early-phase results. However, no commercial allicin-based antimicrobial has reached clinical practice, again because of formulation stability challenges. The most well-developed topical garlic formulations for MRSA are research-grade products that have not yet successfully completed phase-3 clinical trials.
The Iwalokun 2004 study (Journal of Medicinal Food) extended this work to a panel of multidrug-resistant Gram-positive and Gram-negative bacteria from Nigerian clinical isolates, finding broad inhibitory activity for aqueous garlic extract. The Reuter / Koch / Lawson 1996 garlic textbook compiles the broader Gram-positive activity data — Streptococcus, Enterococcus, Listeria, Bacillus, Corynebacterium, and other genera all show in vitro susceptibility.
The clinical translation: garlic is not a substitute for vancomycin, linezolid, or daptomycin in serious MRSA infection. But for the patient interested in chronic decolonization adjunct (recurrent staph furunculosis, recurrent nasal MRSA carriage), garlic extracts may have a role as part of a layered strategy that also includes nasal mupirocin (if susceptible), chlorhexidine washes, and household-level hygiene measures.
Gram-Negative Bacteria, Including Helicobacter pylori
Gram-negative susceptibility to allicin is generally somewhat lower than Gram-positive (the lipopolysaccharide-rich outer membrane is a partial barrier to small-molecule penetration), but meaningful activity has been documented against Escherichia coli, Salmonella, Shigella, Klebsiella, Pseudomonas aeruginosa, and Helicobacter pylori. The H. pylori activity is the most clinically relevant.
The Sivam 2001 review in Journal of Nutrition summarized the in vitro evidence that garlic extracts inhibit H. pylori growth at minimum inhibitory concentrations achievable by oral garlic intake. The mechanism includes both direct thiol-targeting of H. pylori cysteine-rich virulence factors and disruption of the bacterium's urease enzyme (which neutralizes gastric acid to allow colonization). Garlic-treated H. pylori cultures show morphologic changes consistent with cell wall stress and metabolic disruption.
The clinical translation to adjunctive H. pylori eradication is discussed in its own section below. The broader point is that gastric and small-intestinal pathogens are an unusual case for orally administered garlic because they encounter relatively high local concentrations of allicin and polysulfides before systemic absorption and thiol-mediated inactivation. This is the mechanistic reason garlic has more credible activity against gut-lumen pathogens than against systemic pathogens.
Antifungal Spectrum — Candida and Beyond
Ledezma and Apitz-Castro's 2006 review in Revista Iberoamericana de Micologia documents ajoene — one of the principal allicin decomposition products — as the most active antifungal component of garlic, with substantial in vitro activity against Candida albicans, Cryptococcus neoformans, Aspergillus species, and dermatophyte fungi (the causes of athlete's foot and ringworm). The Davis 2005 review in Mycoses provides additional spectrum data on allicin breakdown products.
The Iwalokun 2004 work on Nigerian clinical isolates included multiple Candida species, demonstrating inhibitory activity at concentrations achievable in topical or oral garlic preparations.
The most realistic clinical applications:
- Vulvovaginal candidiasis (recurrent) — some practitioners use vaginal garlic preparations as adjunctive therapy. The evidence base is anecdotal/case-series, not randomized-trial-level. Concerns about local irritation and the unreliable allicin yield of homemade preparations limit recommendation. Standard antifungal therapy (oral fluconazole, topical azoles) remains first-line.
- Oral candidiasis — oral garlic intake may have adjunctive effect; topical raw garlic application to the oral mucosa is not recommended because of risk of chemical burn.
- Dermatophyte infections (athlete's foot, ringworm) — topical garlic preparations have small studies supporting use; topical terbinafine and clotrimazole remain first-line.
- Gastrointestinal candidiasis / SIBO overgrowth — AGE may have a place in adjunctive management; standard antifungal and antimicrobial therapy remains first-line. See our SIBO page for more.
Antiparasitic Activity — Giardia, Entamoeba, Others
The Soffar and Mokhtar 1991 trial in Journal of the Egyptian Society of Parasitology evaluated aqueous garlic extract for human giardiasis. 26 patients with confirmed Giardia lamblia infection were treated with garlic extract for three days; parasitologic cure (stool clearance) was reported in the majority of treated patients, and clinical symptom resolution was rapid. The trial was small, single-arm, and not blinded, but it documented a real-world clinical effect of garlic against an enteric parasite at a culturally appropriate dose.
Other parasitic targets with in vitro or small-trial garlic activity:
- Entamoeba histolytica — in vitro activity demonstrated; clinical use historical, particularly in folk medicine of regions where amebiasis is endemic
- Hymenolepis nana (dwarf tapeworm) — the Soffar 1991 trial included tapeworm cases with reported clinical clearance
- Cryptosporidium parvum — in vitro evidence; clinically untested at scale
- Trichomonas vaginalis — in vitro evidence; standard treatment (metronidazole) remains first-line
- Intestinal nematodes (roundworms, hookworms, pinworms) — historical use in folk medicine; modern antihelminthic drugs (albendazole, mebendazole, ivermectin) are vastly more effective and should be first-line
The pattern with parasites is similar to that with bacteria: garlic has documented activity, but the modern targeted antiparasitic drugs are dramatically more effective for serious parasitic disease. Garlic's realistic role is as an adjunct or as a historical traditional intervention in settings where standard drugs are not available, not as first-line therapy in modern clinical practice.
Garlic as Adjunctive Therapy in H. pylori Eradication
Standard Helicobacter pylori eradication uses combination antibiotic therapy — usually triple therapy (proton pump inhibitor + amoxicillin + clarithromycin), quadruple therapy with bismuth (PPI + bismuth + metronidazole + tetracycline), or one of the newer regimens (PPI + amoxicillin + levofloxacin, or rifabutin-based regimens) — for 10-14 days, with eradication rates of 70-90% depending on local resistance patterns. Rising clarithromycin resistance is a major problem and is reducing the effectiveness of standard triple therapy in many regions.
Garlic's potential role is as an adjunct to standard antibiotic therapy, intended to improve eradication rates or reduce the duration of antibiotic exposure required. The published evidence is suggestive but not yet at the level of routine guideline recommendation. The Sivam 2001 review summarized early in vitro and pilot clinical data; subsequent small randomized trials have explored aged garlic extract or fresh garlic as add-ons to triple therapy with modestly improved eradication in some studies.
The mechanism is plausible: garlic-derived compounds inhibit H. pylori in vitro at concentrations achievable by oral intake, the gastric environment provides locally high concentrations before thiol-mediated inactivation, and garlic does not produce the cross-resistance that complicates antibiotic-only regimens. A reasonable clinical approach for the patient with previously failed eradication is to discuss with the gastroenterologist whether adjunctive aged garlic extract (1-2 g/day) for the duration of the antibiotic course represents a reasonable addition. See our H. pylori page for the broader management context.
Topical Uses — Skin, Ear, Vaginal Considerations
Topical garlic applications have a long folk-medicine history. The modern clinical perspective is cautious about most of these uses, primarily because of two concerns:
- Chemical burns — raw garlic applied directly to skin or mucosa for more than brief contact can produce serious chemical burns. The thiosulfinate chemistry that targets bacterial proteins also damages human keratinocytes. Folk-medicine recipes that recommend prolonged skin application of raw garlic (for warts, fungal infections, or wound care) carry real risk of full-thickness burn.
- Allergic contact dermatitis — garlic is a recognized cause of occupational allergic contact dermatitis, particularly in restaurant workers, and personal sensitization can develop with repeated topical exposure
Specific topical considerations:
- Skin and wound — direct application of raw garlic is not recommended. Diluted garlic-oil preparations may be used but should be tested on a small skin area first.
- Ear (otic instillation) — some folk-medicine traditions instill garlic-infused oil for otitis externa or otitis media. There are small studies of commercial garlic ear-oil products for ear pain, but routine use of homemade preparations is not recommended; for any suspected serious ear infection, conventional evaluation and antibiotic therapy as indicated are appropriate.
- Vaginal — insertion of raw garlic cloves for vaginal candidiasis is a common folk-medicine practice but carries risk of irritation, retained foreign body, and inadequate antifungal effect. Topical or oral azole antifungals are dramatically more reliable.
- Nasal — nasal application of raw garlic is not recommended; it produces severe mucosal irritation.
The general principle: garlic at culinary doses ingested orally is well-tolerated and represents the vast majority of safe traditional use. Direct topical application of concentrated raw garlic to skin or mucosa is high-risk and should be approached with caution or avoided.
Why Allicin Is Not a Clinical Antibiotic
Given allicin's broad-spectrum in vitro activity, low toxicity to mammalian cells at moderate doses, and 80-year history of safety in dietary use, it is reasonable to ask why allicin has not become a clinical antibiotic. The reasons are essentially pharmaceutical:
- Chemical instability — allicin decomposes in aqueous solution at body temperature with a half-life of hours, faster at higher pH and in the presence of any reducing agent. It cannot be formulated as a conventional tablet or injectable that maintains active concentration through normal pharmaceutical shelf life.
- Pharmacokinetic challenges — oral allicin is largely inactivated by gastric acidity and first-pass thiol scavenging in the gut and liver. Achieving meaningful systemic free allicin concentrations from oral dosing is impractical.
- Lack of intellectual property — allicin is a natural product that cannot be patented as such. Without patent protection, no pharmaceutical company will fund the multi-hundred-million-dollar clinical trial program required to obtain regulatory approval.
- Tolerability — oral allicin at therapeutic doses produces severe gastrointestinal effects, halitosis, and body odor at levels incompatible with sustained clinical use.
Research-grade allicin formulations (stabilized aqueous extracts, sustained-release matrices, prodrug strategies) have been developed in academic settings, and there is ongoing work on chemically synthesized allicin analogs (allyl-substituted thiosulfinates with improved stability) as drug candidates. None has yet reached clinical practice.
The pragmatic implication: garlic's antimicrobial role in modern medicine is realistically limited to dietary intake (which provides modest, broad, low-grade antimicrobial activity), adjunctive use alongside conventional antibiotics in selected indications, and continued laboratory study as a chemistry inspiration for next-generation antimicrobial drug design. It is not a substitute for appropriate antibiotic therapy in any serious bacterial infection.
Cautions — What Garlic Is Not For
- Serious bacterial infection — garlic is not a substitute for appropriate culture-directed antibiotic therapy in any serious infection (sepsis, pneumonia requiring hospitalization, abscess, endocarditis, bacterial meningitis, urinary tract infection with pyelonephritis, surgical-site infection). Seek prompt medical evaluation and follow guideline-directed antimicrobial therapy.
- Methicillin-resistant S. aureus (MRSA) infection — documented in vitro activity does not translate to clinical adequacy in serious MRSA infection. Standard intravenous therapy (vancomycin, daptomycin, linezolid) is required.
- Tuberculosis — garlic has no established role in TB therapy. Standard four-drug regimen (rifampin, isoniazid, pyrazinamide, ethambutol) is mandatory.
- HIV infection — garlic is not an antiviral substitute and interacts with the protease inhibitor saquinavir (reducing plasma concentrations). Consult HIV specialist before use.
- Topical chemical burns — do not apply raw garlic directly to skin for more than brief contact. Burns from prolonged garlic poultice application are a recognized clinical entity.
- Bleeding-risk situations — the same antiplatelet caution from the other Garlic Benefits pages applies. Discontinue garlic supplements 7 days before any surgical or dental procedure with bleeding risk.
- Pregnancy and lactation — dietary garlic is safe; high-dose antimicrobial-intent garlic supplementation has not been well-studied and should be discussed with obstetric or pediatric care provider.
- Pediatric infectious disease — garlic does not substitute for appropriate pediatric antibiotic therapy. Children with serious bacterial infection require conventional medical care.
- Realistic expectations — garlic's antimicrobial role in modern medicine is as a low-risk adjunct, dietary contribution, and chemistry-inspiration for drug discovery — not as a substitute for guideline-directed therapy in serious infection.
Key Research Papers
- Cavallito CJ, Bailey JH (1944). Allicin, the antibacterial principle of Allium sativum. I. Isolation, physical properties and antibacterial action. Journal of the American Chemical Society 66:1950-1951. — PubMed
- Ankri S, Mirelman D (1999). Antimicrobial properties of allicin from garlic. Microbes and Infection 1:125-129. — PubMed
- Cutler RR, Wilson P (2004). Antibacterial activity of a new, stable, aqueous extract of allicin against methicillin-resistant Staphylococcus aureus. British Journal of Biomedical Science 61:71-74. — PubMed
- Sivam GP (2001). Protection against Helicobacter pylori and other bacterial infections by garlic. Journal of Nutrition 131:1106S-1108S. — PubMed
- Ledezma E, Apitz-Castro R (2006). Ajoene the main active compound of garlic (Allium sativum): a new antifungal agent. Revista Iberoamericana de Micologia 23:75-80. — PubMed
- Soffar SA, Mokhtar GM (1991). Evaluation of the antiparasitic effect of aqueous garlic (Allium sativum) extract in hymenolepiasis nana and giardiasis. Journal of the Egyptian Society of Parasitology 21:497-502. — PubMed
- Davis SR (2005). An overview of the antifungal properties of allicin and its breakdown products — the possibility of a safe and effective antifungal prophylactic. Mycoses 48:95-100. — PubMed
- Iwalokun BA, Ogunledun A, Ogbolu DO, Bamiro SB, Jimi-Omojola J (2004). In vitro antimicrobial properties of aqueous garlic extract against multidrug-resistant bacteria and Candida species from Nigeria. Journal of Medicinal Food 7:327-333. — PubMed
- Reuter HD, Koch HP, Lawson LD (1996). Therapeutic effects and applications of garlic and its preparations. In: Garlic: The Science and Therapeutic Application of Allium sativum L. and Related Species. Williams & Wilkins. — PubMed
- Bayan L, Koulivand PH, Gorji A (2014). Garlic: a review of potential therapeutic effects. Avicenna Journal of Phytomedicine 4:1-14. — PubMed
- Tsai CW, Chen HW, Sheen LY, Lii CK (2012). Garlic: Health benefits and actions. BioMedicine 2:17-29. — PubMed
- Lawson LD, Hunsaker SM (2018). Allicin Bioavailability and Bioequivalence from Garlic Supplements and Garlic Foods. Nutrients 10(7):812. — PubMed
PubMed Topic Searches
- PubMed: Allicin and broad-spectrum antimicrobial
- PubMed: Garlic and MRSA
- PubMed: Garlic and H. pylori eradication
- PubMed: Ajoene / garlic antifungal
- PubMed: Garlic antiparasitic
Connections
- Garlic Overview
- Garlic Benefits Hub
- Garlic for Cardiovascular & Blood Pressure
- Garlic for Cholesterol & Atherosclerosis
- Garlic for Immune Function & Cold
- Oregano (Carvacrol Antimicrobial)
- Manuka Honey
- Echinacea
- Thyme (Thymol)
- Immune Boosting
- Helicobacter pylori
- SIBO
- Glutathione
- Cysteine
- All Herbs