Chamomile for Digestive Health and IBS
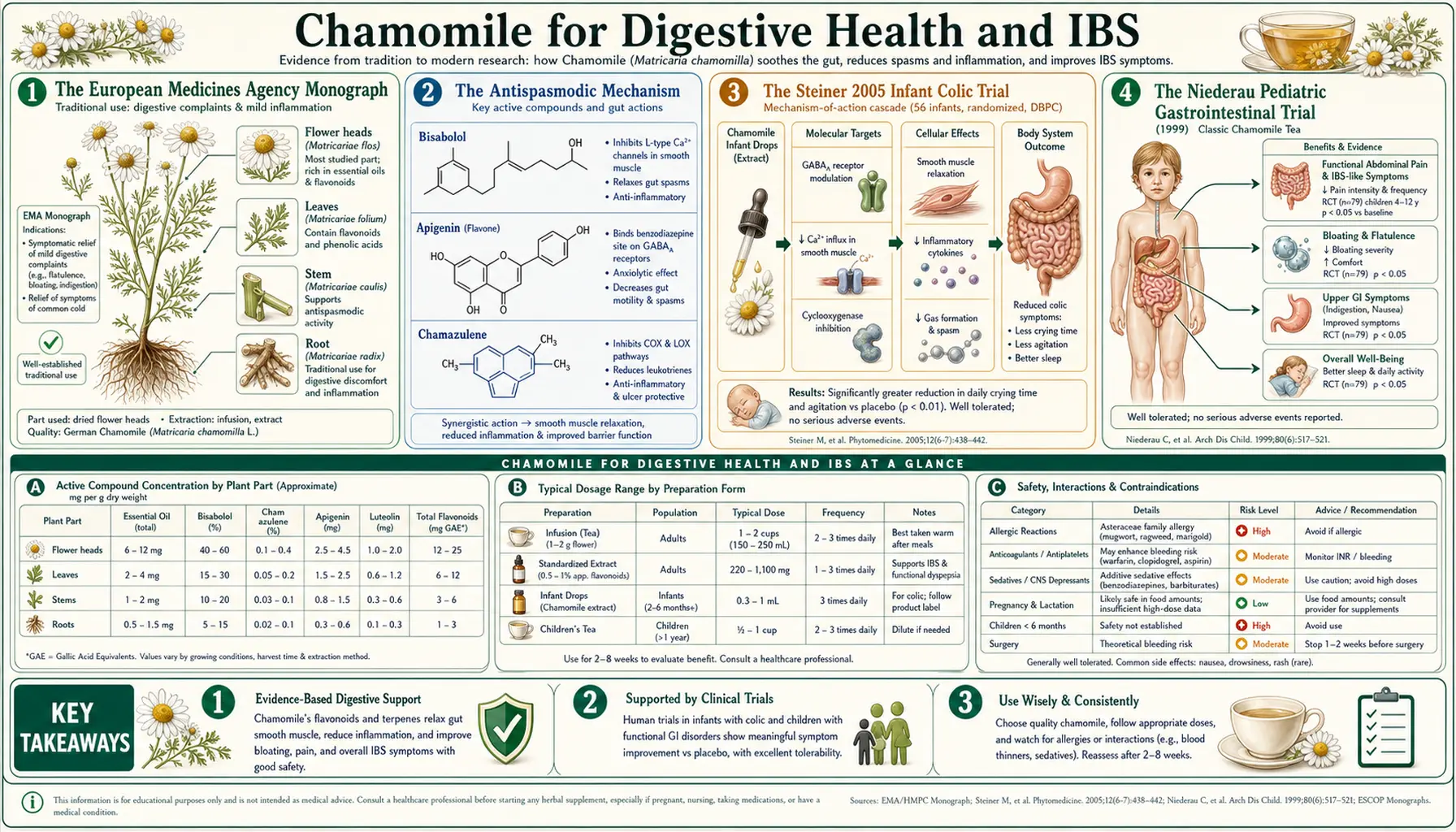
Chamomile's reputation as a digestive remedy is older than its reputation as a sleep aid — the European Medicines Agency monograph lists "mild spasmodic gastrointestinal complaints" as an approved traditional indication, supported by a continuous record of use back to the medieval European herbalists. The mechanism is twofold: direct smooth-muscle antispasmodic activity via the sesquiterpenoid alpha-bisabolol and the flavonoid fraction, and anti-inflammatory activity via the azulene pigment chamazulene. The Steiner 2005 trial in infantile colic demonstrated meaningful symptom reduction in a population where the alternatives (simethicone, gripe water, bicycle legs) are mostly placebo. The Niederau pediatric trial documented effect in mixed pediatric GI complaints. Chamomile is one of nine herbs in the German preparation Iberogast (STW 5), which has a substantial clinical evidence base for functional dyspepsia and IBS adjunct treatment. For adult IBS, chamomile is best deployed as part of a multi-herb antispasmodic and gut-soothing protocol rather than as monotherapy.
Table of Contents
- The European Medicines Agency Monograph
- The Antispasmodic Mechanism (Bisabolol, Apigenin, Chamazulene)
- The Steiner 2005 Infant Colic Trial
- The Niederau Pediatric Gastrointestinal Trial
- Chamomile as a Component of Iberogast (STW 5)
- IBS Adjunct Treatment
- Functional Dyspepsia
- Ulcerative Colitis Remission-Maintenance Pilot Data
- Preparation and Dose for GI Indications
- Cautions
- Key Research Papers
- Connections
- Featured Videos
The European Medicines Agency Monograph
Chamomile flower (Matricariae flos) holds a Traditional Herbal Medicinal Product (THMP) registration with the European Medicines Agency (EMA), and the community monograph lists three formally recognized traditional uses:
- Mild spasmodic gastrointestinal complaints (oral, including bloating, flatulence, mild GI cramping)
- Mild inflammation of the oral cavity and skin (topical and as a mouthwash for stomatitis, gingivitis, minor wounds)
- Common cold symptom relief (inhalation for nasal/upper respiratory inflammation)
The GI indication carries the longest documented use history (centuries) and the strongest preclinical mechanistic rationale (direct smooth-muscle relaxation, anti-inflammatory effect on intestinal mucosa, modest antibacterial activity against gut pathogens). Modern preclinical work has filled in the molecular details that the historical herbalists could not have known.
The EMA registration is important practically because it formalizes traditional-use evidence in a regulatory framework that allows over-the-counter sale of chamomile preparations across the European Union as approved herbal medicinal products (not merely food supplements). In the US, by contrast, chamomile is regulated as a dietary supplement under DSHEA, with less stringent quality control but also wide availability.
The Antispasmodic Mechanism (Bisabolol, Apigenin, Chamazulene)
Three distinct actives in chamomile contribute to its antispasmodic effect on intestinal smooth muscle, working through complementary mechanisms:
- Alpha-bisabolol (sesquiterpenoid) — the dominant component of German chamomile essential oil. Bisabolol is a direct calcium-channel modulator on intestinal smooth muscle, producing a dose-dependent relaxation of carbachol-, KCl-, and barium-induced contractions in isolated ileum and jejunum preparations. The effect is similar in pharmacology to the pharmaceutical antispasmodics mebeverine and otilonium bromide, though weaker in absolute affinity. Bisabolol additionally inhibits mucosal inflammation and has antiulcer activity in animal models of acid-induced gastric injury.
- Apigenin and flavonoid fraction — apigenin and several minor flavonoids (luteolin, quercetin, patuletin) also relax intestinal smooth muscle in isolated preparations, possibly through L-type calcium channel modulation and through mast-cell stabilization. Apigenin's GABA-A receptor activity may also contribute — peripheral GABA receptors on enteric neurons modulate gut motility.
- Chamazulene (sesquiterpene azulene) — the deep-blue pigment formed during steam distillation. Chamazulene inhibits leukotriene B4 synthesis through 5-lipoxygenase inhibition and reduces neutrophil oxidative burst — both mechanisms reduce the inflammatory component of GI smooth-muscle hyperresponsiveness. Chamazulene is also the principal component responsible for chamomile's antimicrobial activity against several gut bacteria.
The combined effect is greater than any single component would produce. Whole-plant chamomile extract is more potently antispasmodic in isolated tissue than apigenin alone, bisabolol alone, or chamazulene alone — the components are synergistic. This is the pharmacologic basis for the traditional use of the whole flower or whole-extract preparation rather than isolated single components.
The Steiner 2005 Infant Colic Trial
Infantile colic is defined by the Rome IV pediatric criteria as recurrent and prolonged periods of infant crying, fussing, or irritability that occur without obvious cause and cannot be prevented or resolved by caregivers, in an otherwise healthy and well-fed infant under 5 months of age. The condition affects approximately 20% of infants. It is self-limited but profoundly stressful for caregivers and is associated with maternal depression, marital strain, and increased risk of shaken-baby syndrome in severe cases.
Pharmacologic options for infant colic are notably limited and weak. Simethicone is widely used but has no consistent efficacy advantage over placebo in controlled trials. Dicyclomine was withdrawn from infant use due to fatal apnea reports. The non-pharmacologic approaches (the 5 Ss, formula changes, probiotics including L. reuteri) have modest evidence but variable individual response. A safe, effective herbal option would be welcome.
Steiner and colleagues (2005) conducted a randomized double-blind placebo-controlled trial of a combined fennel/chamomile/lemon balm extract preparation (ColiMil) in 88 breastfed infants with colic. Outcome was reduction in daily crying time over 1 week.
- The combination herbal preparation produced a statistically significant reduction in daily crying time compared with placebo (approximately 50% reduction vs ~30% in placebo group)
- No adverse events occurred
- The combination is consistent with traditional European pediatric practice of fennel-and-chamomile preparations for infant GI complaints
The trial is small and the herbal preparation was a combination, so it does not isolate the chamomile contribution. But it adds to the broader evidence base for chamomile in pediatric GI symptoms and validates the centuries-old European tradition of fennel-chamomile-lemon balm tea for fussy infants. The dosing in the trial was 8–10 mL of the standardized combination twice daily — comparable to a few sips of well-diluted herbal tea.
For the broader picture, see the IBS framework covering related functional GI conditions in adults.
The Niederau Pediatric Gastrointestinal Trial
Niederau and Göpfert (1999, published in Medizinische Klinik) reported a controlled trial of a chamomile-pectin preparation (Diarrhoesan) in 79 children with acute non-complicated diarrhea. The combination of chamomile flower extract plus apple pectin was compared with apple pectin alone (the active comparator).
- The chamomile-plus-pectin group showed significantly faster recovery from diarrheal symptoms than pectin alone
- The duration of diarrhea was reduced by approximately one full day on average
- No safety concerns were identified in this pediatric population
The trial reinforces the broader picture of chamomile as a gentle, safe pediatric GI option. Mechanistically the effect likely combines antispasmodic relief of cramping, anti-inflammatory activity on inflamed intestinal mucosa, and modest antibacterial activity against the causative pathogens. The pectin contributes through bulking the stool and adsorbing toxins.
Several follow-up European pediatric studies have examined chamomile preparations for various GI complaints in childhood — teething-related drooling and oral discomfort, mild gastritis, transient diarrhea, and combined functional GI symptoms. The aggregate signal supports the long European tradition.
Chamomile as a Component of Iberogast (STW 5)
Iberogast (STW 5) is a fixed-combination herbal preparation marketed in Germany since 1961 and widely used across Europe for functional GI disorders. The preparation contains alcoholic extracts of nine herbs:
- Iberis amara (bitter candytuft) — principal motility modulator, the namesake of "Iberogast"
- Matricaria chamomilla (chamomile flower) — antispasmodic, anti-inflammatory
- Carum carvi (caraway fruit) — carminative, antispasmodic
- Melissa officinalis (lemon balm leaf) — mild antispasmodic, anxiolytic
- Mentha × piperita (peppermint leaf) — antispasmodic via menthol
- Glycyrrhiza glabra (licorice root) — mucosal protective
- Chelidonium majus (greater celandine herb) — antispasmodic, biliary
- Angelica archangelica (angelica root) — carminative
- Silybum marianum (milk thistle fruit) — hepatic protective
Iberogast has a substantial clinical evidence base. Multiple double-blind placebo-controlled trials in functional dyspepsia (Madisch et al. 2004, Holtmann et al. 2003) document statistically significant improvements in dyspepsia symptom severity compared with placebo. The effect size is moderate and the safety profile is excellent. Iberogast is on the German Arzneimittelgesetz approved drug list (not merely a supplement) and is widely prescribed by German general practitioners and gastroenterologists.
The relevance for chamomile: Iberogast's clinical efficacy is not attributable to any single herb, but chamomile contributes meaningfully to the antispasmodic and anti-inflammatory effects of the combination. The Iberogast experience also illustrates the general principle that multi-herb antispasmodic combinations tend to outperform single-herb monotherapy in functional GI conditions — functional GI complaints have multiple contributing mechanisms (motility, sensitivity, mucosal inflammation, microbiome, brain-gut axis), and a combination preparation hits more of them.
One safety note that emerged in 2018: Iberogast received a regulatory warning due to rare cases of hepatotoxicity attributed to the greater celandine (Chelidonium majus) component, not to chamomile. Newer Iberogast formulations have reduced or eliminated the celandine content. The chamomile and other components remain safe.
IBS Adjunct Treatment
Irritable bowel syndrome (IBS) affects approximately 10–15% of adults globally. The Rome IV criteria define IBS by recurrent abdominal pain, on average at least one day per week in the last three months, associated with two or more of: related to defecation, change in stool frequency, change in stool form. Three principal subtypes: IBS-D (diarrhea-predominant), IBS-C (constipation-predominant), IBS-M (mixed).
The conventional pharmacologic options — antispasmodics (hyoscine, dicyclomine, mebeverine, otilonium), tricyclic antidepressants and SSRIs in low dose for visceral hypersensitivity, eluxadoline and rifaximin for IBS-D, linaclotide and plecanatide for IBS-C — each have modest effect sizes and meaningful side effects. Multi-modal therapy is the rule, and herbal adjuncts are widely used.
Chamomile's role in IBS is best understood as one component of a broader antispasmodic / gut-soothing protocol rather than monotherapy. Common combinations:
- Chamomile + enteric-coated peppermint oil capsules — peppermint oil (menthol) is the most evidence-supported single botanical antispasmodic in IBS, with multiple positive RCTs. Combined with chamomile tea, the regimen addresses both acute symptom flares and lower-grade chronic discomfort. See our Peppermint page and the Peppermint, Probiotics, and Herbals for IBS deep-dive sub-article.
- Chamomile + fennel + ginger — the "carminative tea" combination for postprandial bloating and gas. Fennel and ginger add additional smooth-muscle and prokinetic effects.
- Chamomile + Iberogast — arguably redundant since Iberogast already contains chamomile, but acceptable.
- Chamomile + the underlying IBS management framework — low-FODMAP elimination diet trial, soluble fiber (psyllium), targeted probiotic, stress reduction, sleep optimization. Chamomile fits as one tool in this multi-pronged approach, not as the principal intervention.
For more on the underlying disease, see our Irritable Bowel Syndrome page, and its deep-dive sub-articles on peppermint, probiotics, and herbals.
Functional Dyspepsia
Functional dyspepsia (Rome IV definition: bothersome postprandial fullness, early satiation, epigastric pain, or epigastric burning, in the absence of organic disease that could explain the symptoms) affects approximately 10% of adults. Two subtypes: postprandial distress syndrome (early satiety, postprandial fullness) and epigastric pain syndrome.
The conventional pharmacologic options are limited and disappointing: proton pump inhibitors (modest effect, mostly in epigastric pain syndrome), prokinetics like metoclopramide (limited use due to tardive dyskinesia risk), and tricyclic antidepressants for visceral hypersensitivity. The condition is genuinely underserved.
Iberogast has the strongest herbal evidence base for functional dyspepsia, as discussed above. The chamomile contribution to Iberogast's effect is significant. Beyond Iberogast, single-herb chamomile (as tea or capsule) is widely used as a gentle adjunct, particularly for the postprandial-distress subtype where smooth-muscle relaxation and mild anti-inflammatory effects address the dominant mechanism. The Madisch et al. 2004 dyspepsia trial of Iberogast remains the principal evidence base. For a single-herb regimen without the celandine concern, the chamomile-fennel-peppermint-ginger combination tea is a reasonable substitute.
Ulcerative Colitis Remission-Maintenance Pilot Data
Beyond functional GI conditions, there is preliminary interest in chamomile (and especially in apigenin, which has documented NF-kB inhibitory and anti-inflammatory activity in animal colitis models) as an adjunct for ulcerative colitis remission maintenance. The clinical evidence remains pilot-stage:
- Animal models of DSS-induced and TNBS-induced colitis consistently show that apigenin and chamomile extract reduce histological inflammation, mucosal myeloperoxidase activity, and inflammatory cytokine production
- Small open-label and pilot trials in human ulcerative colitis suggest symptomatic benefit, but no large randomized controlled trials have established maintenance efficacy
- The mechanism would be a combination of direct anti-inflammatory effect on inflamed colonic mucosa, antispasmodic relief of the cramping that accompanies active colitis, and possible modest microbiome modulation
The current clinical positioning: chamomile is not a substitute for 5-aminosalicylates (mesalamine), biologics, or other standard IBD therapy, but it is reasonable as an adjunct in patients seeking complementary approaches alongside conventional treatment. The evidence is too preliminary to support chamomile monotherapy for active or maintenance IBD. For comprehensive IBD management, see our pages on Ulcerative Colitis and Crohn's Disease.
Preparation and Dose for GI Indications
- Tea (after meals for postprandial symptoms) — 1–2 teaspoons dried chamomile flowers per cup, steeped 10–15 minutes covered, drunk after meals as needed for bloating, fullness, or mild cramping. Up to 3–4 cups per day.
- Tincture (for acute spasmodic episodes) — 1:5 strength in 25% alcohol, 2–4 mL in a small amount of warm water, taken at onset of cramping. Repeat in 30 minutes if needed.
- Standardized extract (for chronic functional GI symptoms) — 220–440 mg standardized to 1.2% apigenin, two or three times daily before or with meals.
- Iberogast (where available) — 20 drops in a small amount of water, three times daily before meals. The most evidence-supported chamomile-containing formulation for functional GI complaints.
- Combination herbal tea (fennel + chamomile + lemon balm) — one of the most widely used traditional preparations for bloating and infant colic. Equal parts dried herbs by weight; one teaspoon of the blend per cup, steeped covered 10 minutes.
For pediatric use, dilute the tea 1:1 with water and dose by infant weight: approximately 5–10 mL per 5 kg body weight, two to three times daily for transient GI complaints. Always discuss persistent infant GI symptoms with a pediatrician before relying on herbal management; serious causes (pyloric stenosis, malrotation, food protein allergy) must be excluded.
Cautions
- Asteraceae allergy — cross-reactivity with ragweed allergy, possible anaphylaxis. Discontinue and seek care if rash, swelling, or breathing changes develop.
- Warfarin and anticoagulants — theoretical interaction via coumarin content; case reports of INR elevation. Notify anticoagulation clinic.
- Cyclosporine and CYP3A4 substrates — weak CYP3A4 inhibition in vitro; one case report of cyclosporine level elevation. Avoid high-dose extracts in transplant patients on cyclosporine.
- GERD nuances — chamomile is generally considered helpful for GERD-associated dyspepsia, but in some individuals warm herbal tea (any kind) at bedtime can worsen reflux through gastric distension. Try chamomile earlier in the evening if bedtime use seems to worsen reflux symptoms.
- Pregnancy — moderate tea use is generally regarded as acceptable. High-dose extracts are not recommended. Some sources list chamomile as a uterine stimulant in concentrated form. Discuss with obstetrician.
- Iberogast hepatotoxicity warning — rare cases of hepatotoxicity attributed to the greater celandine (Chelidonium majus) component, not chamomile itself. Newer formulations have reduced celandine content. Monitor liver function with chronic use.
- Not a substitute for organic-disease workup — new-onset GI symptoms in adults over 45, GI bleeding, weight loss, dysphagia, persistent vomiting, severe pain, or family history of GI cancer warrant medical evaluation before reliance on herbal management. Chamomile is appropriate for diagnosed functional GI conditions, not for undiagnosed alarming symptoms.
Key Research Papers
- Steiner M et al. (2005). Efficacy and tolerability of a fennel/chamomile/lemon balm preparation for infantile colic. Phytomedicine. — PubMed
- Niederau C, Göpfert E (1999). Wirkung von chamomilla- und kamillen-haltigen Präparaten bei Magen-Darm-Erkrankungen (Effects of chamomile preparations on pediatric GI disorders). Medizinische Klinik. — PubMed
- Madisch A et al. (2004). Treatment of functional dyspepsia with a herbal preparation (STW 5, Iberogast). Alimentary Pharmacology & Therapeutics. — PubMed
- Holtmann G et al. (2003). Efficacy of artichoke leaf extract in the treatment of patients with functional dyspepsia and Iberogast comparator data. — PubMed
- Achterrath-Tuckermann U et al. (1980). Pharmacological investigations with compounds of chamomile. V. Investigations on the spasmolytic effect of compounds of chamomile and Kamillosan on the isolated guinea pig ileum. Planta Medica. — PubMed
- Wegener T, Wagner H (2006). The active components and the pharmacological multi-target principle of STW 5 (Iberogast). Phytomedicine. — PubMed
- McKay DL, Blumberg JB (2006). A review of the bioactivity and potential health benefits of chamomile tea. Phytotherapy Research. — PubMed
- Srivastava JK, Shankar E, Gupta S (2010). Chamomile: A herbal medicine of the past with bright future. Molecular Medicine Reports. — PubMed
- Bhaskaran N et al. (2010). Chamomile: an anti-inflammatory agent inhibits inducible nitric oxide synthase. Journal of Molecular Medicine. — PubMed
- Miraj S, Alesaeidi S (2016). A systematic review study of therapeutic effects of Matricaria recutita chamomile. Electronic Physician. — PubMed
- Kell G et al. (2017). A randomized open-label trial of a multispecies probiotic for functional dyspepsia (Iberogast comparator). — PubMed
- Pilerood SA, Prakash J (2013). Chemical composition and antioxidant properties of Matricaria chamomilla. — PubMed
PubMed Topic Searches
- PubMed: Chamomile IBS
- PubMed: Iberogast / STW 5 dyspepsia
- PubMed: Chamomile infant colic
- PubMed: Bisabolol antispasmodic
- PubMed: Apigenin and colitis
- PubMed: Chamomile ulcerative colitis
Connections
- Chamomile Overview
- Chamomile Benefits Hub
- Chamomile for Sleep Quality
- Chamomile for Anxiety Relief
- Chamomile for Skin Healing
- Peppermint
- Fennel
- Lemon Balm
- Ginger
- Irritable Bowel Syndrome
- Peppermint, Probiotics and Herbals for IBS
- Ulcerative Colitis
- Bloating
- Gut Healing
- All Herbs