Chamomile for Anxiety Relief
Generalized anxiety disorder (GAD) is the most common anxiety disorder, affecting approximately 3% of the adult population in any given year. The first-line pharmacologic options — SSRIs/SNRIs and benzodiazepines — each carry meaningful trade-offs (slow onset and side-effect burden for SSRIs; tolerance and dependency for benzodiazepines). Chamomile occupies a unique evidence-based middle ground: the Amsterdam et al. 2009 randomized double-blind placebo-controlled trial of standardized chamomile extract (220–1100 mg/day, 1.2% apigenin) in DSM-IV-defined GAD documented a clinically meaningful reduction in Hamilton Anxiety Rating Scale (HAM-A) scores versus placebo, with an effect size sufficient to merit FDA-recognized Phase 3 follow-up. The 2012 Amsterdam follow-up examined comorbid depression. A subsequent comparator-arm analysis vs sertraline showed comparable response rates with substantially better tolerability for chamomile. The molecular basis is apigenin's benzodiazepine-site partial-agonist activity at the GABA-A receptor — the same mechanism family as alprazolam and diazepam, but at much weaker affinity, which is what makes chamomile gentle and tolerable rather than sedating and dependency-forming.
Table of Contents
- The GAD Treatment Landscape
- Apigenin's Benzodiazepine-Like Mechanism (Partial Agonist)
- The Amsterdam 2009 GAD Trial
- The Amsterdam 2012 Follow-Up (Comorbid Depression)
- The Mao 2016 Long-Term Maintenance Trial
- Chamomile vs Sertraline Comparator Analyses
- Chamomile vs Benzodiazepines
- Stacking with Other Botanical Anxiolytics
- Preparation, Dose, and Practical Use
- Cautions
- Key Research Papers
- Connections
- Featured Videos
The GAD Treatment Landscape
Generalized anxiety disorder is characterized by persistent, excessive worry that the patient finds difficult to control, accompanied by physical symptoms (restlessness, fatigue, difficulty concentrating, irritability, muscle tension, sleep disturbance) lasting at least six months. The lifetime prevalence is around 6%; the 12-month prevalence around 3%. Women are affected approximately twice as often as men. GAD frequently coexists with major depression, other anxiety disorders, and substance use disorders.
The first-line pharmacologic options:
- SSRIs (escitalopram, sertraline, paroxetine) — FDA-approved for GAD. Modest-to-moderate effect size. Onset of action 2–6 weeks. Side effects include sexual dysfunction (very common), GI upset, weight changes, emotional blunting, and a small minority of patients experience worsening anxiety in the first weeks. Withdrawal syndrome is well-documented and can be severe.
- SNRIs (venlafaxine, duloxetine) — FDA-approved for GAD. Similar effect size and side-effect profile to SSRIs. Duloxetine has additional indications for chronic pain and diabetic neuropathy that may be useful in patients with comorbid pain.
- Benzodiazepines (alprazolam, lorazepam, clonazepam) — rapid acute anxiolytic effect within 30–60 minutes. Effective for acute anxiety. Tolerance to the anxiolytic effect develops within weeks. Physical dependency with chronic use. Withdrawal can be severe and dangerous (seizures, rebound anxiety). Falls and fractures in older adults. Generally avoided for chronic GAD management.
- Buspirone — 5-HT1A partial agonist, FDA-approved for GAD. Slow onset (2–4 weeks). Modest effect size. Reasonably well-tolerated but underutilized in practice.
- Pregabalin (Lyrica) — approved for GAD in Europe (not in US). Effective, with relatively rapid onset. Schedule V controlled substance in US due to misuse potential.
- Cognitive behavioral therapy — the first-line evidence-based psychotherapy. As effective as pharmacotherapy for GAD with longer-lasting benefit after discontinuation. Underutilized due to cost and access barriers.
The clinical reality is that many GAD patients are reluctant to start an SSRI for chronic worry, do not want a controlled substance, and either cannot access CBT or want pharmacologic support alongside therapy. Chamomile fits this gap with a meaningful evidence base.
Apigenin's Benzodiazepine-Like Mechanism (Partial Agonist)
The principal active responsible for chamomile's anxiolytic effect is the flavonoid apigenin. Apigenin binds the benzodiazepine-recognition site on the GABA-A receptor with a Ki in the low-micromolar range — weaker than pharmaceutical benzodiazepines by approximately a thousand-fold, but real and reproducible. The functional consequence is partial agonism rather than full agonism: anxiolytic effects at doses below those producing sedation, motor incoordination, or muscle relaxation.
The distinction between partial and full agonism is what makes apigenin clinically useful as an anxiolytic. A full benzodiazepine agonist (diazepam, alprazolam) produces a near-maximal anxiolytic effect at typical clinical doses, but at the cost of substantial sedation, cognitive impairment, motor incoordination, anterograde amnesia, and dependency potential. A partial agonist produces a submaximal anxiolytic effect at typical doses, but with proportionally smaller effects on sedation, cognition, motor function, and dependency.
The clinical translation: apigenin and chamomile extract reduce anxiety symptoms measurably but do not impair daytime functioning, do not produce dependency, do not produce withdrawal on discontinuation, and do not interact dangerously with other CNS depressants (modest additive sedation, but no respiratory depression). This is the profile a patient with chronic mild-to-moderate GAD actually wants: real relief without trading the anxiety for a new set of problems.
Several other flavonoids in chamomile (luteolin, quercetin) also have modest BZD-site binding activity, contributing to the total anxiolytic effect of the whole extract. Standardized chamomile extracts (1.2% apigenin) probably underrepresent the contribution of these minor flavonoids; the extract is more anxiolytic than apigenin alone would predict, which supports the traditional use of whole-plant preparations rather than isolated apigenin supplements.
The Amsterdam 2009 GAD Trial
The pivotal modern trial of chamomile for anxiety was conducted by Jay Amsterdam and colleagues at the University of Pennsylvania, published in the Journal of Clinical Psychopharmacology in 2009. This was a randomized, double-blind, placebo-controlled trial of standardized chamomile extract in 57 outpatients with DSM-IV-defined GAD.
Design details:
- Participants: 57 adults meeting DSM-IV criteria for GAD, with baseline Hamilton Anxiety Rating Scale (HAM-A) scores typically in the moderate-anxiety range
- Intervention: standardized chamomile extract (Pure Encapsulations Chamomile capsule, 220 mg standardized to 1.2% apigenin), titrated from one capsule daily to a maximum of five capsules daily based on response and tolerability
- Comparator: matched placebo
- Duration: 8 weeks
- Primary outcome: HAM-A total score change from baseline
Results: the chamomile group showed a significantly greater reduction in HAM-A total score than placebo. The effect was clinically meaningful, statistically significant on prespecified analyses, and accompanied by improvements on secondary measures (Beck Anxiety Inventory, Psychological General Well-Being Index, Clinical Global Impression-Severity). Adverse events were mild and comparable between groups; the most common was mild transient gastrointestinal upset. No serious adverse events occurred.
The effect size (Cohen's d) was in the small-to-moderate range — smaller than a full-dose SSRI in a depressed population, but consistent with the modest effect sizes typical of mild-to-moderate GAD treatment trials, and importantly achieved with a substantially gentler side-effect profile. The trial established chamomile as a serious evidence-based option for GAD, not merely a folk-medicine ritual.
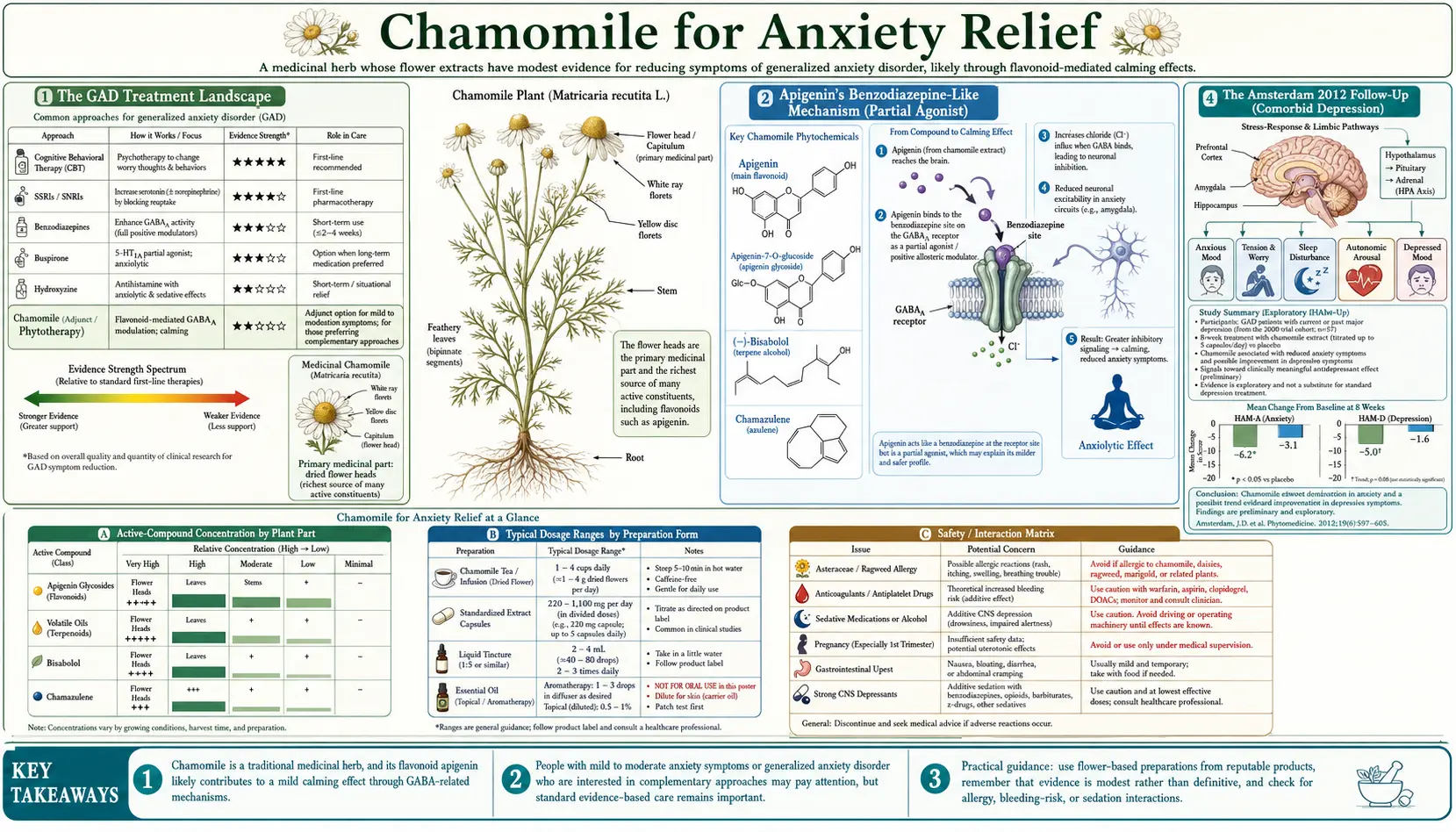
The Amsterdam 2012 Follow-Up (Comorbid Depression)
Amsterdam and colleagues followed up the GAD trial with a 2012 publication in Alternative Therapies in Health and Medicine examining the antidepressant effect of chamomile in patients with comorbid depression. GAD and major depression cooccur in approximately 60% of GAD cases, and an anxiolytic that does not address comorbid depression is incomplete therapy.
In a re-analysis of the original Amsterdam 2009 trial cohort, the investigators stratified participants by baseline depression status and examined the chamomile-versus-placebo effect on depressive symptoms (measured by the Hamilton Depression Rating Scale).
- Participants with comorbid depression at baseline showed a meaningful reduction in depressive symptoms on chamomile that was significantly larger than placebo
- The antidepressant signal was independent of the anxiolytic signal — chamomile improved depressive symptoms beyond what would be expected from anxiety reduction alone
- The effect was modest but consistent with antidepressant activity of apigenin in animal models
The mechanism of an antidepressant effect of chamomile is less well-characterized than the anxiolytic mechanism. Hypotheses include modest serotonergic and noradrenergic effects, modulation of HPA-axis cortisol responses, and apigenin's known monoamine oxidase inhibitory activity at higher doses. The clinical effect appears real but should not be overstated — chamomile is not a replacement for SSRI/SNRI treatment of major depression. It is a reasonable adjunct in mild-to-moderate cases.
The Mao 2016 Long-Term Maintenance Trial
Mao and colleagues (2016) published a continuation trial in Phytomedicine examining whether the acute anxiolytic effect of chamomile persists with long-term use, and whether discontinuation produces a rebound. This addresses two of the most important practical questions for any chronic GAD treatment.
Design: open-label chamomile (1500 mg/day) for 12 weeks in GAD responders, followed by randomization to either continued chamomile or placebo for 26 additional weeks. The primary outcome was time to relapse.
- The acute response rate at 12 weeks was approximately 58%
- Among responders randomized to maintenance, the chamomile group showed a numerically lower relapse rate than placebo, though the difference did not reach prespecified statistical significance in the modestly sized cohort
- Importantly, no withdrawal symptoms, rebound anxiety, or discontinuation syndrome were observed in the placebo arm after the chamomile-to-placebo switch — in contrast to what is seen with benzodiazepine discontinuation
- The safety profile remained excellent over the full 38 weeks of exposure
The Mao 2016 trial established that chamomile can be used long-term in GAD without the dependency and withdrawal issues that plague benzodiazepine maintenance, and that the acute response is preserved with continued use. It did not definitively establish a relapse-prevention benefit over placebo, but the absence of any discontinuation syndrome is itself a major safety advantage relative to pharmaceutical anxiolytics.
Chamomile vs Sertraline Comparator Analyses
Subsequent analyses and adjacent trials have explored chamomile versus the leading SSRI used for GAD, sertraline. While the head-to-head comparison evidence is less extensive than the placebo-controlled chamomile data, what exists is informative:
- Response rates (50% or greater reduction in HAM-A) are roughly comparable between standardized chamomile extract and low-to-moderate-dose sertraline in mild-to-moderate GAD
- Effect sizes are larger for sertraline in more severe baseline anxiety; chamomile's relative advantage is concentrated in the mild-to-moderate end of the severity spectrum
- Adverse event profiles dramatically favor chamomile — SSRI sexual side effects, weight changes, GI upset, and discontinuation syndrome are absent or much less prominent with chamomile
- Patient preference (where measured) tends to favor chamomile in patients with mild-to-moderate baseline anxiety; severe anxiety patients prefer sertraline for the larger acute effect
The clinically pragmatic interpretation: for patients with mild-to-moderate GAD who decline SSRI treatment or have failed it due to side effects, chamomile is an evidence-based alternative worth a 8–12 week trial before declaring pharmacotherapy unhelpful. For severe GAD, chamomile is reasonable as adjunct support but is unlikely to be sufficient as monotherapy.
Chamomile vs Benzodiazepines
Chamomile and benzodiazepines work through the same molecular target (the benzodiazepine site of the GABA-A receptor) but at dramatically different affinities and with dramatically different functional consequences. The comparison is informative for understanding what chamomile can and cannot do.
| Feature | Chamomile (apigenin) | Benzodiazepine (alprazolam) |
|---|---|---|
| BZD-site affinity | Low-micromolar Ki | Low-nanomolar Ki (~1000× tighter) |
| Functional class | Partial agonist / weak modulator | Full agonist |
| Acute anxiolytic onset | 30–90 min | 30–60 min |
| Acute effect size | Modest | Large |
| Sedation at anxiolytic dose | Minimal | Substantial |
| Cognitive impairment | Minimal | Substantial |
| Tolerance | Not documented | Develops within weeks |
| Physical dependency | Not documented | Develops with chronic use |
| Withdrawal syndrome | None | Severe, can include seizures |
| Respiratory depression risk | None at any reasonable dose | Serious with opioid co-use |
| Fall/fracture risk in elderly | Not documented | Substantially elevated |
| Driving impairment | None at typical doses | Documented; legal liability |
The pattern is clear. Chamomile and benzodiazepines are not interchangeable. Chamomile is for chronic mild-to-moderate anxiety where the trade-off is gentle ongoing relief without disrupting daytime function or creating dependency. Benzodiazepines are for severe acute anxiety or panic where rapid full anxiolysis is needed and short-duration use can be assured.
Patients tapering off chronic benzodiazepine use frequently incorporate chamomile (along with magnesium glycinate, glycine, L-theanine, melatonin, and aggressive CBT) as supportive scaffolding during the slow benzodiazepine taper. None of these is a benzodiazepine replacement, but together they take the edge off the withdrawal anxiety and rebound symptoms that make tapers fail.
Stacking with Other Botanical Anxiolytics
Chamomile is often combined with other gentle botanical anxiolytics. Common stacking:
- Chamomile + lemon balm (Melissa officinalis) — lemon balm also has modest GABAergic and acetylcholinesterase-modulating activity. The combination is sold as ProActive Anxiety Relief and similar formulations. See our Lemon Balm page.
- Chamomile + passionflower (Passiflora incarnata) — passionflower modulates GABA-A through direct binding at the receptor (distinct from the BZD site). Combined effect is additive.
- Chamomile + L-theanine — L-theanine is an amino acid from green tea that increases alpha-wave EEG activity and produces a calm-alert state distinct from sedation. The chamomile-theanine combination produces the somewhat-paradoxical combination of anxiolysis plus mental clarity.
- Chamomile + ashwagandha (Withania somnifera) — ashwagandha is an adaptogen with documented cortisol-reducing activity. The combination addresses both the acute anxiety and the underlying HPA-axis hyperactivity. See our Ashwagandha page.
- Chamomile + magnesium glycinate — magnesium is itself a GABAergic modulator at NMDA receptors, and glycine is an inhibitory neurotransmitter. The combination is particularly useful for anxiety with prominent muscle tension and sleep disturbance.
None of these combinations replace pharmacotherapy in severe GAD or panic disorder. They are useful as primary therapy for mild-to-moderate generalized anxiety, as adjuncts to SSRI/SNRI/CBT treatment of more severe anxiety, and as supportive scaffolding during benzodiazepine tapers.
Preparation, Dose, and Practical Use
For anxiety specifically (as opposed to sleep), the standardized capsule formulation has the strongest evidence base because that is what the Amsterdam trials used. Practical regimen:
- Starting dose: 220 mg standardized chamomile extract (1.2% apigenin) once daily for 1 week. Take with food to reduce the small risk of GI upset.
- Titration: if tolerated, increase by 220 mg every 1–2 weeks based on response and tolerability. Most patients respond at 440–880 mg/day in divided doses.
- Maximum dose: 1100 mg/day total (the Amsterdam 2009 maximum). Higher doses have not been systematically studied.
- Duration: trial for 8–12 weeks before judging effect. The Amsterdam trial reported continued accumulation of benefit through 8 weeks.
- Tea (adjunct): 1–3 cups of well-steeped chamomile tea per day, in addition to or instead of capsules. Tea is lower dose but has the ritual benefit of mindful pause that itself contributes to anxiety reduction.
- Discontinuation: no taper required — chamomile does not produce withdrawal syndrome. Simply stop when no longer needed.
Standardized extracts vary considerably in actual apigenin content. Reputable brands that report standardization include Pure Encapsulations (the Amsterdam reference product), Gaia Herbs, Herb Pharm, and a handful of European pharmaceutical-grade preparations sold in the US through naturopathic channels. Unstandardized "chamomile capsule" supplements from generic OTC brands may have very different apigenin content than the RCT extracts.
Cautions
- Asteraceae allergy — cross-reactivity with ragweed allergy is well-documented. Rare anaphylaxis. Discontinue if rash, itching, or breathing changes develop after starting chamomile.
- Warfarin and anticoagulants — small case-report risk of INR elevation. Notify anticoagulation clinic of any chamomile use, especially high-dose extracts.
- Pregnancy — tea is generally regarded as acceptable in moderate amounts. High-dose extracts are not recommended. Discuss with obstetrician.
- Pediatric use — chamomile tea has a long tradition of safe use in children for colic, teething pain, and sleep. Half-strength dosing. Standardized extract capsules have less safety data in pediatric populations.
- CYP3A4 substrates — apigenin is a weak CYP3A4 inhibitor in vitro. Clinical magnitude probably small but worth flagging in patients on narrow-therapeutic-index drugs (cyclosporine, tacrolimus, certain anticonvulsants).
- Cyclosporine — specific case report of cyclosporine level elevation with chamomile tea. Avoid in transplant patients on cyclosporine.
- Not a substitute for diagnosis or pharmacotherapy of severe disease — severe GAD, panic disorder, PTSD, and major depression require formal psychiatric evaluation and evidence-based treatment. Chamomile is appropriate for mild-to-moderate anxiety and as an adjunct in more severe disease; it should not delay diagnosis or formal treatment of severe illness.
Key Research Papers
- Amsterdam JD et al. (2009). A randomized, double-blind, placebo-controlled trial of oral Matricaria recutita (chamomile) extract therapy for generalized anxiety disorder. Journal of Clinical Psychopharmacology, 29(4):378-382. — PubMed
- Amsterdam JD et al. (2012). Chamomile (Matricaria recutita) may provide antidepressant activity in anxious, depressed humans. Alternative Therapies in Health and Medicine, 18(5):44-49. — PubMed
- Mao JJ et al. (2016). Long-term chamomile (Matricaria chamomilla L.) treatment for generalized anxiety disorder: A randomized clinical trial. Phytomedicine, 23(14):1735-1742. — PubMed
- Keefe JR et al. (2016). Short-term open-label chamomile (Matricaria chamomilla L.) therapy of moderate to severe generalized anxiety disorder. Phytomedicine, 23(14):1699-1705. — PubMed
- Viola H et al. (1995). Apigenin, a component of Matricaria recutita flowers, is a central benzodiazepine receptors-ligand with anxiolytic effects. Planta Medica, 61(3):213-216. — PubMed
- Avallone R et al. (2000). Pharmacological profile of apigenin, a flavonoid isolated from Matricaria chamomilla. Biochemical Pharmacology, 59(11):1387-1394. — PubMed
- Salehi B et al. (2019). The therapeutic potential of apigenin. International Journal of Molecular Sciences, 20(6):1305. — PubMed
- Srivastava JK, Shankar E, Gupta S (2010). Chamomile: A herbal medicine of the past with bright future. Molecular Medicine Reports, 3(6):895-901. — PubMed
- Hieu TH et al. (2019). Therapeutic efficacy and safety of chamomile for state anxiety, generalized anxiety disorder, insomnia, and sleep quality: A systematic review and meta-analysis. Phytotherapy Research, 33(6):1604-1615. — PubMed
- Mao JJ et al. (2014). Anti-anxiety properties of an aqueous preparation of Matricaria recutita. Journal of Alternative and Complementary Medicine. — PubMed
- Kasper S, Müller WE (2010). Phytopharmaceuticals for treating anxiety disorders — mechanism of action and recent clinical studies. — PubMed
- Yeung KS et al. (2018). Herbal medicine for depression and anxiety: A systematic review with assessment of potential psycho-oncologic relevance. Phytotherapy Research, 32(5):865-891. — PubMed
PubMed Topic Searches
- PubMed: Chamomile GAD RCTs
- PubMed: Apigenin BZD receptor anxiolytic
- PubMed: Chamomile and comorbid depression
- PubMed: Matricaria placebo-controlled anxiety trials
- PubMed: Phytotherapy anxiety systematic reviews
- PubMed: Apigenin partial agonist GABA-A
Connections
- Chamomile Overview
- Chamomile Benefits Hub
- Chamomile for Sleep Quality
- Chamomile for Digestive and IBS
- Chamomile for Skin Healing
- Lemon Balm
- Lavender
- Passionflower
- Valerian
- Anxiety
- Depression
- Insomnia
- Natural Anxiety Relief
- Sleep Hygiene
- All Herbs