Chamomile for Skin Healing
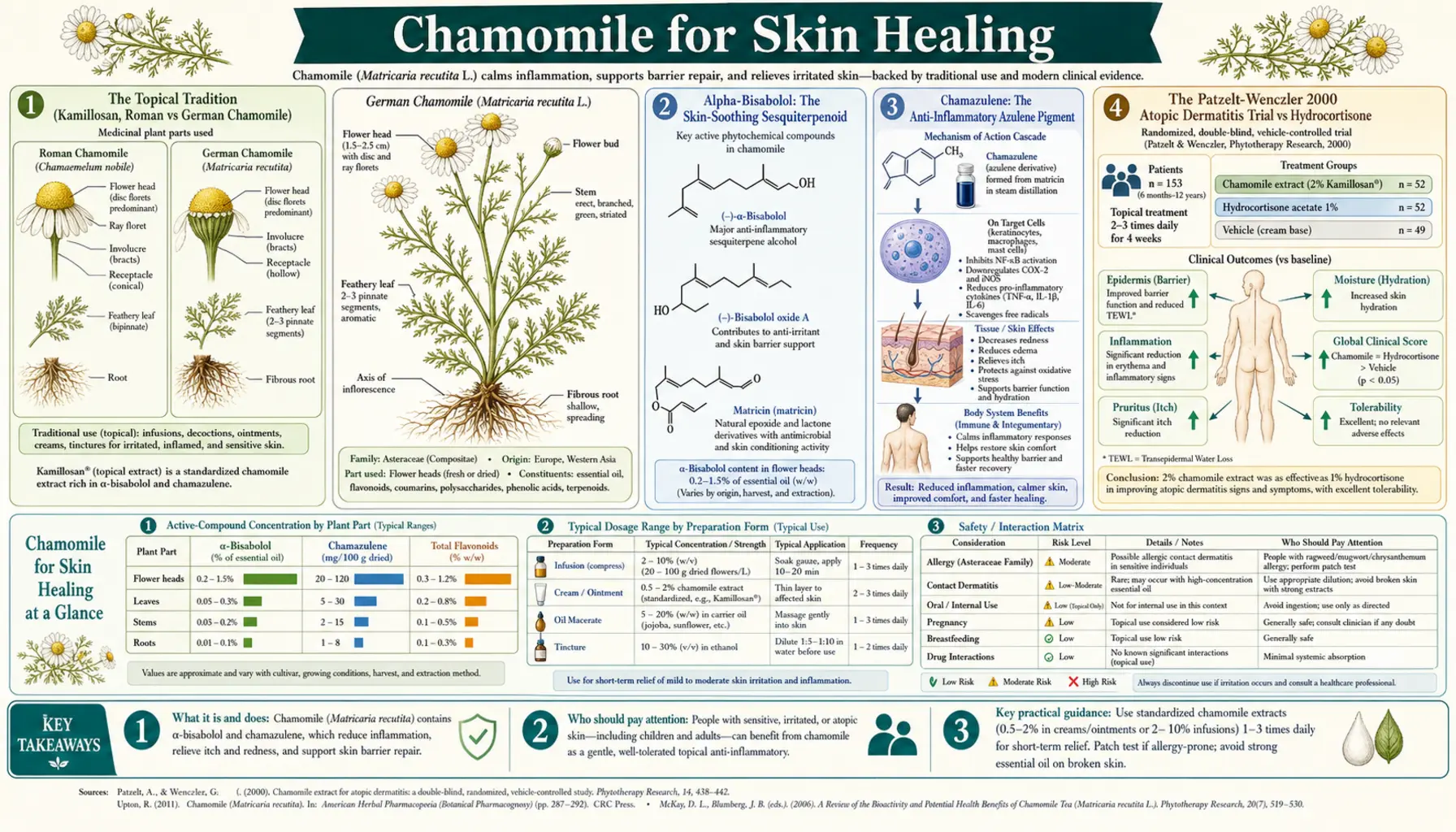
Topical chamomile has the deepest evidence base of any traditional herbal skin remedy. The pivotal study is Patzelt-Wenczler and Ponce-Pöschl 2000, a randomized partially double-blind half-side comparison of the standardized German chamomile cream Kamillosan against 0.5% hydrocortisone in atopic eczema — chamomile cream was approximately equivalent to topical hydrocortisone in symptom reduction, with the safety advantage of not being a topical steroid. The active anti-inflammatory components are alpha-bisabolol (the dominant sesquiterpenoid in chamomile essential oil, a direct skin-soothing terpene used widely in cosmetic preparations) and chamazulene (the deep-blue azulene pigment formed during steam distillation, a 5-lipoxygenase inhibitor that reduces leukotriene-mediated inflammation). Additional evidence supports topical chamomile for episiotomy wound healing, postpartum perineal care, oral mucositis from chemotherapy and radiation, and minor diaper rash. The clinical positioning: a steroid-free option for chronic mild-to-moderate inflammatory skin conditions where long-term steroid use would be problematic.
Table of Contents
- The Topical Tradition (Kamillosan, Roman vs German Chamomile)
- Alpha-Bisabolol: The Skin-Soothing Sesquiterpenoid
- Chamazulene: The Anti-Inflammatory Azulene Pigment
- The Patzelt-Wenczler 2000 Atopic Dermatitis Trial vs Hydrocortisone
- Episiotomy and Postpartum Perineal Wound Healing
- Oral Mucositis (Chemotherapy and Radiation)
- Diaper Rash and Pediatric Skin Care
- Wound Healing and Post-Surgical Use
- Topical Preparations and Application
- Cautions (Contact Dermatitis, Asteraceae Allergy)
- Key Research Papers
- Connections
- Featured Videos
The Topical Tradition (Kamillosan, Roman vs German Chamomile)
The European topical-chamomile tradition is centuries deep. The standard German pharmaceutical preparation is Kamillosan (manufactured by Mylan / Viatris), a 2% chamomile extract cream that has been a pharmacy-shelf staple in German-speaking Europe for decades. The British, French, Italian, and Eastern European pharmacopoeias each include analogous standardized preparations. In the US, chamomile-based cosmetic and OTC topical products are widespread but more variable in standardization and active content.
Two species are conflated in the common name "chamomile" and warrant distinction:
- German chamomile (Matricaria chamomilla, also M. recutita) — the higher-bisabolol, higher-chamazulene species used in nearly all clinical chamomile trials and in Kamillosan. This is the chamomile referenced in essentially all of the topical evidence discussed below.
- Roman chamomile (Chamaemelum nobile) — lower bisabolol content, different essential-oil profile dominated by isobutyl angelate and methylallyl angelate. Used traditionally in English herbalism and as a perfume ingredient. Less clinical evidence as a topical anti-inflammatory.
When the herbal literature, the EMA monograph, the German Commission E, or modern clinical trials refer to topical chamomile, they essentially always mean German chamomile. The two species are not interchangeable for therapeutic purposes — Roman chamomile is more of a fragrance herb than a clinical anti-inflammatory.
Alpha-Bisabolol: The Skin-Soothing Sesquiterpenoid
Alpha-bisabolol is a monocyclic sesquiterpene alcohol, the dominant component of German chamomile essential oil (typically 25–65% of the oil, depending on chemotype and growing conditions). It is the principal anti-inflammatory and skin-soothing component for topical use. The pharmacology has been extensively characterized in dermatologic models:
- Direct anti-inflammatory effect via inhibition of inducible nitric oxide synthase (iNOS) and reduction of NF-kB-mediated cytokine production in keratinocytes
- Mast cell stabilization, reducing histamine release in allergic and irritant skin reactions
- Antibacterial activity against common skin pathogens including Staphylococcus aureus
- Penetration enhancement, allowing co-administered topical actives to reach deeper skin layers
- Direct skin barrier support — bisabolol has documented effects on keratinocyte differentiation and stratum corneum integrity
Bisabolol is so reliably skin-soothing that it has become a standard ingredient in commercial cosmetic and OTC topical formulations, often synthesized rather than chamomile-extracted because synthetic bisabolol is purer and more consistent. The chamomile origin is incidental to the commercial use — bisabolol stands on its own pharmacology. When you see "bisabolol" on the ingredient label of a calming facial cream or a baby wash, the active is the same molecule that gives chamomile cream its clinical effect.
An important distinction in the bisabolol literature: the natural (−)-alpha-bisabolol enantiomer (the one in German chamomile) is approximately twice as anti-inflammatory in standardized topical models as the racemic mixture sold for some industrial applications. High-quality dermatologic preparations specify (−)-alpha-bisabolol; cheaper preparations may use the less-active racemic form.
Chamazulene: The Anti-Inflammatory Azulene Pigment
Chamazulene is the deep indigo-blue tricyclic azulene that gives German chamomile essential oil its famous inky-blue color. The molecule is unusual in plant chemistry — the parent terpene azulenes are deep blue rather than the green or colorless typical of other sesquiterpenes. Chamazulene is not present in the intact plant tissue; it forms during the steam-distillation process from the sesquiterpene lactone precursor matricin, which undergoes thermal rearrangement at distillation temperatures to release chamazulene.
The pharmacology:
- 5-Lipoxygenase inhibition, blocking conversion of arachidonic acid to leukotriene B4 (a key chemotactic and pro-inflammatory mediator in atopic dermatitis, psoriasis, and inflammatory skin disease)
- Antioxidant activity, scavenging reactive oxygen species at sites of inflammation
- Inhibition of neutrophil oxidative burst
- Direct anti-inflammatory effect in topical croton-oil and arachidonic-acid-induced ear edema mouse models
The combination of bisabolol (mast cell, NF-kB, iNOS) and chamazulene (5-lipoxygenase, leukotrienes, oxidative stress) hits at least two non-overlapping arms of the cutaneous inflammatory cascade. The synergy explains why whole-extract topical chamomile preparations outperform isolated single components in dermatologic models, and supports the traditional preference for whole-flower or whole-oil topical use rather than purified single-component cosmetic ingredients.
The Patzelt-Wenczler 2000 Atopic Dermatitis Trial vs Hydrocortisone
Atopic dermatitis (eczema) affects approximately 10% of children and 3% of adults in the developed world. The mainstay of pharmacologic management is topical corticosteroids, used in graduated potency from over-the-counter 0.5–1% hydrocortisone (low potency) up to prescription super-potent clobetasol. Topical steroids work, but chronic use carries meaningful risks: skin atrophy, telangiectasia, perioral dermatitis, tachyphylaxis, and HPA-axis suppression with extensive use. A steroid-sparing topical anti-inflammatory option would be welcome.
Patzelt-Wenczler and Ponce-Pöschl (2000) at the German Hospital in Berlin conducted a randomized, partially double-blind, half-side comparison study in 161 patients with mild-to-moderate atopic eczema of the limbs. Design:
- Each patient applied a different topical treatment to each side of the body (right vs left limb)
- Treatment options compared: Kamillosan chamomile cream, 0.5% hydrocortisone cream, 5% bufexamac cream (a non-steroidal topical anti-inflammatory), and placebo cream
- Duration: 2 weeks twice-daily application
- Outcome: dermatologist-rated severity score (erythema, edema, pruritus, lichenification, excoriation)
Results:
- Kamillosan cream produced approximately the same improvement as 0.5% hydrocortisone cream on all measured parameters
- Both Kamillosan and hydrocortisone were significantly better than bufexamac and placebo
- The chamomile cream had no steroid-class adverse effects (no skin thinning, no telangiectasia, no rebound on discontinuation)
- Tolerability was excellent in both active groups
The interpretation needs some nuance: 0.5% hydrocortisone is the lowest-potency topical steroid, suitable for mild eczema only. Chamomile cream matching low-dose hydrocortisone does not mean it matches the high-potency steroids needed for severe disease. But for the large population of patients with mild-to-moderate eczema where the realistic alternative is OTC hydrocortisone, chamomile cream is a credible alternative with a better long-term safety profile and no concern about steroid-induced skin changes.
The clinical positioning: chamomile cream is first-line steroid-free option for chronic mild atopic dermatitis, particularly for facial application (where topical steroid use is limited by atrophy and periocular complications) and for areas where the patient anticipates needing repeated treatment over weeks to months. For severe eczema flares, high-potency topical steroid is still the right acute treatment; chamomile is then useful for maintenance and steroid-sparing during taper. For more on the disease, see our Eczema page.
Episiotomy and Postpartum Perineal Wound Healing
Episiotomy and perineal lacerations are common complications of vaginal delivery, affecting a large majority of first-time mothers and a meaningful fraction of multiparous deliveries. Recovery is often painful and slow, and is complicated by the obligate exposure of the wound to urine and stool. Topical preparations that accelerate healing and reduce pain are clinically valuable in the postpartum period.
Several controlled trials have examined topical chamomile preparations for episiotomy and perineal wound healing in postpartum women. Aggregate findings:
- Chamomile ointment or sitz-bath application produces faster wound healing on the standardized REEDA (Redness, Edema, Ecchymosis, Discharge, Approximation) scale than no intervention or routine care alone
- Topical chamomile is approximately comparable to topical almond oil in healing rates in one Iranian RCT
- Pain scores are reduced compared with placebo
- No safety concerns in the postpartum perineal use context
The mechanism likely combines the bisabolol anti-inflammatory effect on damaged tissue, the chamazulene leukotriene-modulating effect on the local inflammatory response, modest antibacterial activity against perineal flora (reducing infection risk), and the warm-moist application's general physical benefit on wound closure.
Practical use: post-delivery sitz baths with strong chamomile tea infusion (1 cup dried chamomile flowers infused in 4 cups boiling water for 15 minutes, then strained and added to a basin of warm bath water) two to three times daily for the first one to two weeks postpartum. Alternative: pre-made chamomile sitz-bath sachets sold by herbal-pharmacy retailers. Cream formulations can be applied after sitz bath.
Oral Mucositis (Chemotherapy and Radiation)
Oral mucositis — severe inflammation and ulceration of the oral mucosa — is one of the most distressing toxicities of cancer chemotherapy and head-and-neck radiation therapy. Severe oral mucositis can require parenteral nutrition, opioid pain management, and treatment dose reduction. The conventional management includes meticulous oral hygiene, ice chip prophylaxis, and a variety of topical agents (lidocaine, sucralfate suspension, "magic mouthwash" combinations).
Chamomile mouthwash has been studied as an adjunct for chemotherapy and radiation oral mucositis with mixed but generally encouraging results:
- Several small RCTs report reduction in mucositis severity scores in patients using chamomile mouthwash three to five times daily during chemotherapy or head-and-neck radiation
- The mechanism is the same bisabolol + chamazulene anti-inflammatory pair, applied topically to the inflamed oral mucosa
- Tolerability is generally excellent — chamomile mouthwash is much better tolerated than alcohol-based mouthwashes or hydrogen peroxide
- The Mayo Clinic North Central Cancer Treatment Group trial of chamomile mouthwash for 5-FU-induced mucositis was negative, but that trial used a non-standardized preparation and the methodology has been criticized
The clinical positioning is best summarized as a reasonable, low-cost, well-tolerated adjunct in addition to standard oral mucositis management. It is not a substitute for ice-chip prophylaxis during high-dose chemotherapy, professional dental evaluation prior to head-and-neck radiation, or opioid pain management of severe established mucositis. Standardized preparations or freshly brewed strong chamomile tea, swished and spat three to five times daily, are the typical application.
Diaper Rash and Pediatric Skin Care
Chamomile-containing baby washes and creams have a long European tradition for routine pediatric skin care and for diaper rash. The evidence base is less formal than the eczema literature but supports the practical use:
- Chamomile cream applied to mild-to-moderate diaper rash produces faster resolution than petroleum jelly alone in small comparison studies
- For severe diaper rash with secondary candidiasis, antifungal treatment (clotrimazole, nystatin) is needed in addition to chamomile
- For severe diaper rash with bacterial superinfection, topical antibiotic is needed
- Chamomile is suitable as a preventive routine application or as primary treatment of uncomplicated mild diaper rash
Pediatric topical chamomile use carries an important caveat: avoid in infants and children with known or suspected Asteraceae allergy. The atopic-dermatitis context is particularly relevant — children with eczema are at elevated risk of cross-sensitization to topical herbal allergens including chamomile. Patch test on a small area first if there is any history of atopic disease in the child.
Pediatric chamomile bath is a centuries-old European tradition for calming fussy babies and treating mild skin irritation. Add one cup of strong chamomile tea infusion to the bath water. The fragrance has a calming effect on caregivers as well, which is not a trivial benefit during a difficult bedtime.
Wound Healing and Post-Surgical Use
Beyond episiotomy, topical chamomile has been studied in a variety of wound-healing contexts:
- Post-cesarean section wound healing — small studies suggest topical chamomile applied to the C-section incision after dressing removal accelerates closure and reduces scar prominence at 1-month follow-up
- Hemorrhoid topical use — chamomile sitz baths or cream application reduce pain and pruritus of external hemorrhoids and post-hemorrhoidectomy wounds
- Phlebitis at IV cannula sites — an Iranian RCT reported reduced phlebitis severity with topical chamomile gel applied to peripheral IV insertion sites
- Pressure ulcers (decubitus) — preliminary evidence supports topical chamomile as an adjunct in stage I-II pressure ulcer care, in combination with standard pressure relief and nutritional support. Not adequate as primary treatment for stage III-IV ulcers
- Burns — chamomile preparations have traditional use for minor first-degree burns (sunburn, minor thermal burns). Aloe vera has stronger evidence in this setting and is preferred. Chamomile is reasonable for second-line use or in combination
The mechanism across these wound contexts is consistent: the bisabolol-chamazulene anti-inflammatory pair, modest antibacterial activity reducing wound bioburden, mucosal-barrier and keratinocyte support during re-epithelialization. The effect is supportive rather than dramatic; chamomile is a useful adjunct, not a substitute for primary wound care.
Topical Preparations and Application
- Standardized chamomile cream (Kamillosan, 2% standardized extract) — the reference product from the Patzelt-Wenczler trial. Apply thinly to affected area two to three times daily. Pharmacy-shelf product in German-speaking Europe; mail-order in US.
- Generic chamomile creams (US OTC) — widely available but variable in active content. Look for products specifying bisabolol concentration or standardized extract content.
- Strong tea infusion as compress or sitz bath — 1 cup dried chamomile flowers steeped in 4 cups just-boiled water for 15 minutes covered, then strained. Apply as warm compress to affected skin, or add to sitz-bath basin for perineal indications, or use as oral mouthwash for stomatitis.
- Essential oil dilution — 1–3 drops German chamomile essential oil per teaspoon of carrier oil (jojoba, sweet almond, fractionated coconut). Apply to affected area. Never apply undiluted essential oil to skin — risk of sensitization is meaningful.
- Tincture — 1:5 in 40% alcohol, applied diluted 1:10 in water as a topical wash for inflamed skin. The alcohol content is drying and not appropriate for chronic eczema use; suits transient acute inflammation.
- Combination products — chamomile is commonly combined with calendula, lavender, and aloe vera in commercial topical preparations. Each adds complementary anti-inflammatory or wound-healing activity. See our Calendula page and Lavender page.
For any new chamomile topical, patch test on the inner forearm before applying to larger areas, especially in patients with atopic disease or known plant allergies. Apply a small amount, wait 24 hours, look for any redness, itching, or rash. If clear, proceed to broader use.
Cautions (Contact Dermatitis, Asteraceae Allergy)
- Asteraceae allergy and contact dermatitis — the single most important safety concern with topical chamomile. Patients with known ragweed, daisy, or chrysanthemum allergy are at elevated risk of cross-reactivity. Chamomile contact dermatitis is well-documented in dermatologic literature, particularly with high-concentration essential oil exposure. Patch test before extensive use.
- Photosensitization (rare) — isolated case reports of chamomile-associated phototoxic reactions, mostly with essential oil application. Not a major clinical concern at typical cream concentrations.
- Periorbital application — avoid direct application to the eyelids or near the eye. Diluted compress for blepharitis or stye is traditional and generally safe but should be made with care and discarded if eye irritation occurs.
- Open wound application — standardized chamomile creams are generally safe on minor wounds. Avoid essential oil or alcoholic tincture on open wounds (irritation, sensitization risk).
- Pregnancy (topical) — topical chamomile is generally considered safe in pregnancy at standard concentrations. Avoid essential oil use in early pregnancy.
- Pediatric — topical chamomile has long traditional safe use in infants and children, but caution in atopic children with high risk of contact sensitization. Always patch test in atopic children before broader use.
- Not a substitute for diagnosis of skin disease — new-onset rash, lesions that are not resolving, lesions with unusual features (asymmetric pigmented lesions, ulceration without clear cause, bleeding), or systemic symptoms warrant dermatologic evaluation. Chamomile is appropriate for diagnosed inflammatory skin conditions, not for undiagnosed worrisome lesions.
Key Research Papers
- Patzelt-Wenczler R, Ponce-Pöschl E (2000). Proof of efficacy of Kamillosan(R) cream in atopic eczema. European Journal of Medical Research, 5(4):171-175. — PubMed
- Albring M et al. (1983). The measuring of the anti-inflammatory effect of a compound on the skin of volunteers. Methods and Findings in Experimental and Clinical Pharmacology, 5(8):575-577. — PubMed
- Glowania HJ, Raulin C, Swöboda M (1987). Effect of chamomile on wound healing — a clinical double-blind study. Z Hautkr, 62(17):1262, 1267-1271. — PubMed
- Mazokopakis EE et al. (2005). Wild chamomile (Matricaria recutita L.) mouthwashes in methotrexate-induced oral mucositis. Phytomedicine, 12(1-2):25-27. — PubMed
- Fidler P et al. (1996). Prospective evaluation of a chamomile mouthwash for prevention of 5-FU-induced oral mucositis. Cancer, 77(3):522-525. — PubMed
- Reuter J et al. (2008). Investigation of the anti-inflammatory potential of Aloe vera gel (97.5%) in the ultraviolet erythema test. — PubMed
- Kamatou GPP, Viljoen AM (2010). A review of the application and pharmacological properties of alpha-bisabolol and alpha-bisabolol-rich oils. Journal of the American Oil Chemists' Society, 87:1-7. — PubMed
- Safayhi H et al. (1994). Chamazulene: an antioxidant-type inhibitor of leukotriene B4 formation. Planta Medica, 60(5):410-413. — PubMed
- Srivastava JK, Shankar E, Gupta S (2010). Chamomile: A herbal medicine of the past with bright future. Molecular Medicine Reports, 3(6):895-901. — PubMed
- Aertgeerts P et al. (1985). Comparative testing of Kamillosan cream and steroidal (0.25% hydrocortisone, 0.75% fluocortin butyl ester) and non-steroidal (5% bufexamac) dermatologic agents in maintenance therapy of eczematous diseases. Z Hautkr, 60(3):270-277. — PubMed
- Saller R et al. (2010). Chamomile preparations for the topical treatment of atopic eczema: clinical evidence review. — PubMed
- Pirzad A et al. (2011). Essential oil content and composition of German chamomile cultivated in Iran. Journal of Medicinal Plants Research. — PubMed
PubMed Topic Searches
- PubMed: Chamomile and atopic dermatitis
- PubMed: Chamomile episiotomy and wound healing
- PubMed: Chamomile and oral mucositis
- PubMed: Alpha-bisabolol anti-inflammatory skin
- PubMed: Chamazulene and 5-lipoxygenase
- PubMed: Kamillosan eczema studies
Connections
- Chamomile Overview
- Chamomile Benefits Hub
- Chamomile for Sleep Quality
- Chamomile for Anxiety Relief
- Chamomile for Digestive and IBS
- Calendula
- Lavender
- Aloe Vera
- Eczema (Atopic Dermatitis)
- Psoriasis
- Contact Dermatitis
- Wound Healing
- Gut Healing
- Vitamin A for Skin
- All Herbs