Chamomile for Sleep Quality
A nighttime cup of chamomile tea is the most widely practiced herbal sleep ritual on Earth — the centuries-old folk medicine endorsement of Matricaria chamomilla as a gentle sleep aid is shared across European, Mediterranean, North African, and Latin American cultures. Modern pharmacology has now identified the molecular basis: the flavonoid apigenin binds the benzodiazepine-recognition site on the GABA-A receptor with measurable, low-micromolar affinity, producing a mild anxiolytic and sleep-promoting effect without the dependency, tolerance, cognitive impairment, or morning hangover of pharmaceutical benzodiazepines. Three randomized controlled trials — Adib-Hajbaghery 2017 in elderly nursing-home residents, Chang 2016 in sleep-disturbed postpartum women, and Zick 2011 in adults with chronic primary insomnia — each document measurable sleep-quality improvement on validated instruments (Pittsburgh Sleep Quality Index, Athens Insomnia Scale). The effect size is modest but reproducible, and the safety margin is generous — making chamomile a sensible first-line nighttime option before escalating to OTC antihistamines (diphenhydramine, doxylamine) with their substantial anticholinergic side-effect burden or prescription hypnotics with their dependency potential.
Table of Contents
- The Tradition: A Million Cups a Night
- Apigenin and the Benzodiazepine Receptor Site
- The Adib-Hajbaghery 2017 Elderly Nursing-Home RCT
- The Chang 2016 Postpartum RCT
- The Zick 2011 Chronic Insomnia RCT
- Chamomile vs OTC Sleep Aids (Diphenhydramine, Doxylamine, Melatonin)
- Chamomile vs Prescription Hypnotics (Benzodiazepines, Z-Drugs)
- Preparation and Dose (Tea, Standardized Extract, Tincture)
- Timing, Stacking, and Sleep-Hygiene Pairing
- Cautions and Interactions
- Key Research Papers
- Connections
- Featured Videos
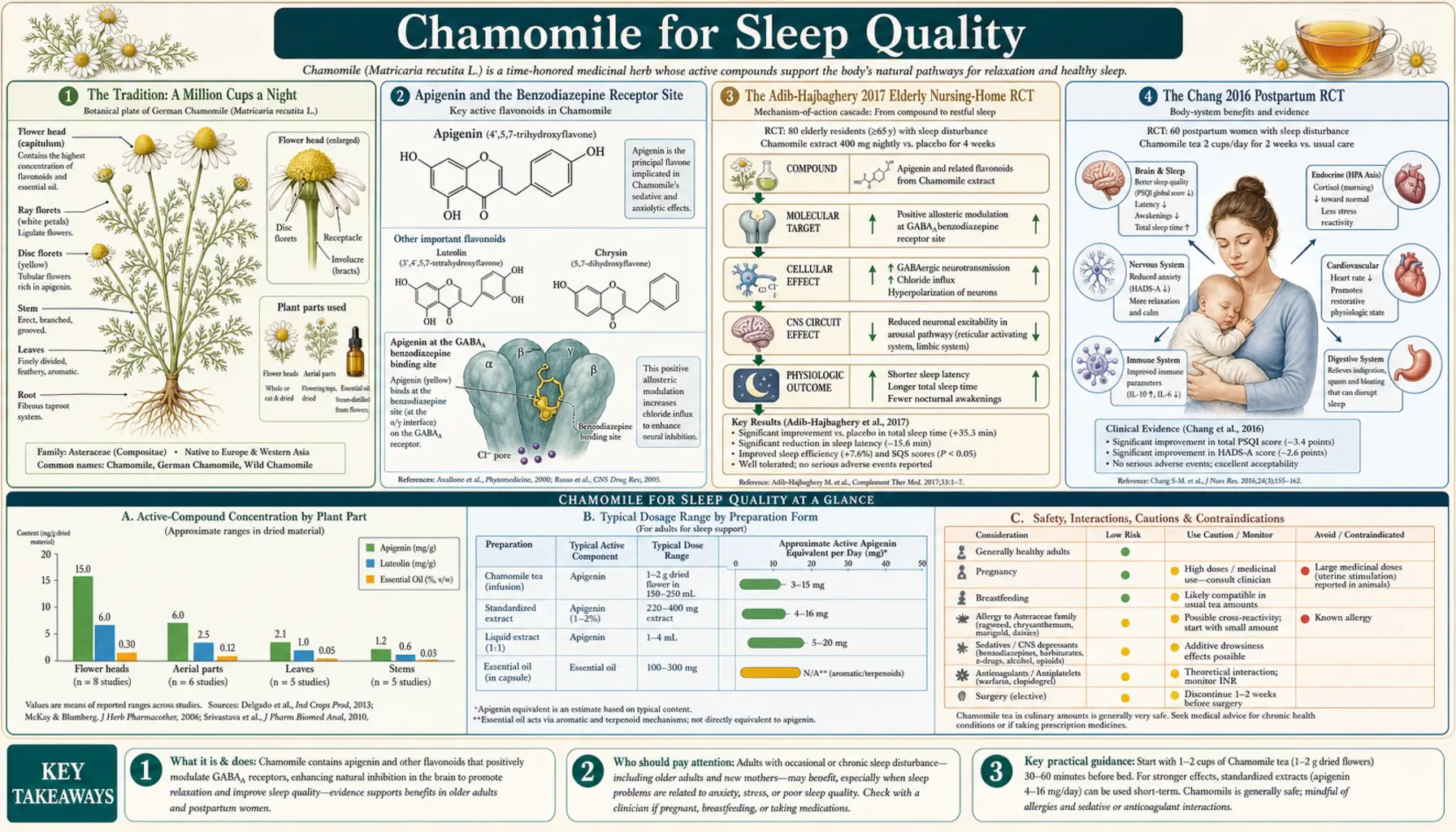
The Tradition: A Million Cups a Night
Chamomile is the most-consumed single-ingredient herbal tea on the planet. The conservative industry estimate is that more than one million cups of chamomile tea are brewed every day for sleep alone — not counting daytime digestive or calming use. The historical record reaches back at least to the ancient Egyptians, who dedicated chamomile to the sun god Ra for fevers; through the Greeks (who called it chamaimelon, "ground apple," for the apple-like aroma of the bruised flower head); through Dioscorides and the medieval European herbalists; through Peter Rabbit, whose mother gave him chamomile tea after his Mr. McGregor escapade because she knew, as every European grandmother knew, that it would settle his nerves and put him to sleep.
The folk-medicine endorsement is unusually consistent across cultures. Spanish manzanilla, Italian camomilla, German Kamille, French camomille, Arabic babunaj, Mexican manzanilla — everywhere the plant grows, the same evening cup for the same indications. When a folk indication is reproduced across cultures that did not share information, that is non-trivial epidemiologic evidence that there is a real underlying effect being detected by ordinary people in ordinary settings.
Modern pharmacology has confirmed that intuition. The question is no longer whether chamomile produces a measurable nighttime calming effect — it does — but how it does so, how big the effect is, and how it stacks against the alternatives a sleep-deprived adult in 2026 actually has in front of them at the drugstore. For broader sleep strategy and non-pharmacologic context, see our Sleep Hygiene page.
Apigenin and the Benzodiazepine Receptor Site
The GABA-A receptor is the principal inhibitory neurotransmitter receptor in the brain. When the inhibitory neurotransmitter GABA (gamma-aminobutyric acid) binds GABA-A, the receptor opens a chloride channel, hyperpolarizing the neuron and reducing its firing probability. This is the single most important "brake" on neural activity in the central nervous system.
The receptor has multiple modulatory sites in addition to the principal GABA-binding site. The most clinically important is the benzodiazepine-recognition site, located at the interface of the alpha and gamma subunits. Drugs that bind here do not open the chloride channel directly — they amplify the effect of endogenous GABA, making the receptor more responsive to whatever GABA happens to be in the synaptic cleft. This is the mechanism of diazepam (Valium), alprazolam (Xanax), lorazepam (Ativan), clonazepam (Klonopin), and the entire benzodiazepine class. It is also the mechanism of the so-called "Z-drugs" — zolpidem (Ambien), zaleplon (Sonata), and eszopiclone (Lunesta) — which bind a different subset of GABA-A receptor subunits but at the same general allosteric site.
Apigenin, the principal flavonoid of chamomile, binds the benzodiazepine site with measurable affinity. The classic Viola et al. demonstration in 1995 showed that apigenin displaces tritiated flunitrazepam from rat cortical membranes with a Ki in the low micromolar range. This is dramatically weaker affinity than a pharmaceutical benzodiazepine — diazepam binds in the low nanomolar range, roughly a thousand-fold tighter — but it is real binding, and it is reproducible across laboratories.
The functional consequence appears to be partial agonism rather than full agonism. Apigenin produces measurable anxiolytic effects in standard rodent models (elevated plus maze, light-dark box) at doses below the threshold for sedation, motor incoordination, or muscle relaxation. Higher doses do produce mild sedation but never the deep sedation or anterograde amnesia of pharmaceutical benzodiazepines, even at orders-of-magnitude higher exposure. This profile — mild anxiolytic and sleep-promoting effects without the deeper benzodiazepine pharmacology — is exactly what the clinical chamomile RCTs report. The molecular mechanism predicts the clinical effect; the clinical effect validates the molecular mechanism.
One important detail: most of the apigenin in dried chamomile flowers is present as the 7-O-glucoside or related glycosides. The glycosides are hydrolyzed to the aglycone in the small intestine and by colonic bacteria. The aglycone is the form that crosses the blood-brain barrier and binds the receptor. Bioavailability is modest (5–15% depending on preparation) but reproducible, and the slow conversion in the gut produces a sustained-release pharmacokinetic profile that suits a nighttime sleep aid.
The Adib-Hajbaghery 2017 Elderly Nursing-Home RCT
Sleep complaints in elderly nursing-home residents are extraordinarily common — surveys consistently report that 50–70% of long-term-care residents report clinically meaningful insomnia. The clinical response to this is unfortunately often a benzodiazepine or Z-drug prescription, both of which are on the Beers Criteria list of medications to avoid in the elderly because of their well-documented increase in fall risk, fracture risk, and confusion. A safer alternative is badly needed.
Adib-Hajbaghery and Mousavi (2017) conducted a randomized clinical trial in 60 elderly nursing-home residents in Iran, randomized to either 200 mg standardized chamomile extract capsule twice daily for 28 days, or matched placebo. The primary outcome was the Pittsburgh Sleep Quality Index (PSQI) total score, a 19-item validated instrument that captures sleep duration, latency, efficiency, disturbances, daytime dysfunction, and use of sleep medication.
- The chamomile group showed a statistically significant reduction in mean PSQI total score from baseline of approximately 3 points on the 0–21 scale
- The placebo group showed no significant change from baseline
- The between-group difference at 4 weeks was clinically meaningful and persisted to study completion
- No serious adverse events occurred in either group; the safety profile was excellent
A 3-point PSQI improvement is not large in absolute terms — pharmacologic interventions can produce larger changes — but it is meaningful in a population where the alternatives carry substantial adverse-effect burdens. For an 80-year-old nursing-home resident, replacing a nightly zolpidem with a twice-daily chamomile capsule (or, perhaps more palatable, a nighttime cup of chamomile tea) and accepting a modest reduction in pharmacologic efficacy may be the right trade in exchange for a substantial reduction in fall and fracture risk.
The Chang 2016 Postpartum RCT
Postpartum sleep disturbance is nearly universal and often accompanied by depressive symptoms. The conventional pharmacologic options (benzodiazepines, antihistamines, antidepressants) are complicated by breastfeeding, where any sedating medication transfers into breast milk to some degree and can produce drowsiness in the nursing infant. A non-pharmacologic or minimally pharmacologic option that does not contraindicate breastfeeding is badly needed.
Chang and Chen (2016) randomized 80 Taiwanese postpartum women with self-reported sleep disturbance to either chamomile tea twice daily for 2 weeks, or routine postpartum care alone. The outcome measures were the PSQI and the Edinburgh Postnatal Depression Scale (EPDS).
- The chamomile-tea group showed statistically significant reductions in both PSQI and EPDS scores at 2 weeks
- The advantage was lost by 4 weeks (1 month after stopping the tea), suggesting the effect requires continued use
- No adverse events were reported in either mothers or breastfeeding infants
The transient nature of the benefit (lost when use stops) is consistent with a mild pharmacologic effect rather than a disease-modifying one — chamomile is not curing postpartum depression, it is producing a temporary sleep and mood improvement while consumed. That is, however, exactly what is needed in the early postpartum period: gentle help bridging the most sleep-deprived months without committing to a medication that complicates breastfeeding.
Chamomile is generally regarded as safe in breastfeeding by lactation pharmacology references, with the caveat that high-concentration extracts (capsules at hundreds of milligrams) have less safety data in lactation than the tea preparation used in this trial. For breastfeeding mothers, the tea is the preferred preparation. For more on postpartum support, see our Postpartum Depression page, and the Sleep Hygiene framework.
The Zick 2011 Chronic Insomnia RCT
Chronic primary insomnia — insomnia not attributable to a medical, psychiatric, or environmental cause and lasting more than three months — affects approximately 10% of adults. The first-line management is cognitive behavioral therapy for insomnia (CBT-I), but access barriers (cost, time, available therapists) often push patients toward pharmacologic options. Chamomile would be welcome as a low-risk adjunct.
Zick and colleagues (2011) at the University of Michigan conducted a preliminary efficacy and safety trial of standardized chamomile extract in 34 adults with DSM-IV-defined chronic primary insomnia. Participants were randomized to either 270 mg standardized chamomile extract (standardized to 1.2% apigenin) twice daily for 28 days, or matched placebo. Outcome measures were sleep diary parameters and validated instruments.
- Chamomile produced modest improvements in sleep diary–measured sleep latency and total sleep time, though several individual outcomes did not achieve statistical significance in the small sample
- Daytime functioning measures and the Athens Insomnia Scale trended favorably
- The trial confirmed safety and feasibility for a larger Phase 3 design
- The standardized extract (Pure Encapsulations Chamomile capsule, 1.2% apigenin) became a reference preparation cited in subsequent Phase 3 designs
Zick et al. concluded that chamomile may have modest benefit in chronic insomnia and that a larger trial was warranted. The signal was consistent with the broader chamomile literature: a real but modest effect, safer than pharmaceutical alternatives, suitable as a first-line option or an adjunct to behavioral therapy.
Chamomile vs OTC Sleep Aids (Diphenhydramine, Doxylamine, Melatonin)
For an adult at the drugstore at 10 PM looking at a sleepless night, the practical comparator for chamomile is the OTC sleep aid shelf. The major options:
- Diphenhydramine (Benadryl, ZzzQuil, Unisom SleepGels) — the first-generation antihistamine in nearly all OTC sleep aids. Strongly anticholinergic. Produces meaningful sedation, but at substantial cost: anticholinergic side effects (dry mouth, constipation, urinary retention, blurred vision), morning grogginess and impaired psychomotor performance the following day, and accumulating evidence that chronic anticholinergic use in older adults raises dementia risk (Gray et al. JAMA Internal Medicine 2015). Beers Criteria flags diphenhydramine as a medication to avoid in elderly.
- Doxylamine (Unisom SleepTabs) — another first-generation antihistamine, even more strongly sedating than diphenhydramine. Same anticholinergic burden and morning grogginess issues. Suitable for occasional use; problematic for chronic use.
- Melatonin — sold OTC in the US (prescription-only in most other countries). Most useful for circadian phase shifting (jet lag, shift work, delayed sleep phase syndrome). Modest effect on sleep maintenance insomnia. Overdosing is common because consumers do not realize that physiologic doses (0.3–0.5 mg) are typically as effective as the 5–10 mg doses commercially sold. Generally safe but with some interaction with autoimmune disease and pregnancy.
- Valerian extract — another GABA-A modulating herb. Modest sleep-onset benefit in meta-analyses. Strong, unpleasant odor that limits compliance. See our Valerian page.
Chamomile's practical advantages: no anticholinergic burden, no morning grogginess, no dementia signal, generally well-tolerated, available either as tea (most flexible dosing, slowest onset) or standardized capsule (more reproducible, faster onset). The disadvantage: smaller average effect size than diphenhydramine. The right comparator framework is "Beers-Criteria-safe alternative with measurable benefit," not "match a sedating antihistamine on knockout potency."
Chamomile vs Prescription Hypnotics (Benzodiazepines, Z-Drugs)
Prescription hypnotics — benzodiazepines (temazepam, lorazepam, alprazolam) and Z-drugs (zolpidem, eszopiclone, zaleplon) — produce dramatically larger acute effects on sleep than chamomile or any OTC option. They also carry dramatically larger risks:
- Tolerance develops within weeks for the sleep-onset benefit, requiring escalating doses
- Physical dependency develops, with withdrawal insomnia that can be worse than the original baseline
- Rebound anxiety on discontinuation
- Anterograde amnesia and unusual sleep behaviors (sleep-driving, sleep-eating, especially with zolpidem)
- Increased fall and fracture risk, especially in older adults
- Mortality signals in observational data with chronic use (controversial but persistent in the literature)
The clinical positioning of chamomile relative to prescription hypnotics is straightforward: chamomile is not a substitute for prescription hypnotics in severe insomnia, but it is a sensible first attempt before escalating to prescription pharmacotherapy, an adjunct that may reduce the prescription dose needed, and a safer maintenance option after CBT-I has resolved the acute insomnia and the patient wants gentle nighttime support without committing to a controlled substance.
For prescription benzodiazepine and Z-drug users actively trying to taper, the typical clinical approach is to introduce chamomile (and other gentle GABAergic herbs like lemon balm and valerian, plus melatonin for circadian support, plus aggressive sleep hygiene) early in the taper as part of the supportive scaffolding. None of these is as potent as the drug being tapered, but together they take the edge off withdrawal insomnia and rebound anxiety.
Preparation and Dose (Tea, Standardized Extract, Tincture)
- Tea (the traditional preparation, lowest dose, most flexible) — one or two teaspoons of dried chamomile flowers (or 1–2 tea bags) per cup of just-boiled water, steeped 10–15 minutes with the cup covered to retain the volatile essential-oil terpenoids. Loose-leaf chamomile from a bulk-herb supplier is typically higher quality than mass-market tea bags. One to three cups per evening for sleep. Children: half-strength tea, half-cup, with parent supervision.
- Standardized extract (capsule, most reproducible) — the form used in most modern RCTs, typically standardized to 1.2% apigenin. The Pure Encapsulations Chamomile capsule (used in the Zick trial) and similar products are widely available. Dose: 220–540 mg one hour before bed, can be doubled if tolerated. Up to 1100 mg/day in divided doses for higher anxiety and sleep targets.
- Tincture (alcoholic or glycerite) — 1:5 strength in 25% alcohol, dosed at 1–3 mL one hour before bed. Glycerite preparations are alcohol-free and suitable for children and recovery populations.
- Essential oil — do not ingest. Chamomile essential oil is for topical use (skin, aromatherapy diffuser) only. Ingestion of essential oil bypasses the safety profile of the whole-plant preparation.
The single most common preparation mistake is steeping the tea uncovered for 3–5 minutes, like a regular black tea. The active volatile terpenoids (bisabolol, chamazulene) and a fraction of the apigenin escape with the steam. Always cover the cup or use a teapot with a lid, and steep at least 10 minutes for full extraction.
Timing, Stacking, and Sleep-Hygiene Pairing
Timing matters. The apigenin glycosides require gut hydrolysis to release the active aglycone, which then needs to cross the blood-brain barrier. Realistic onset is 30–60 minutes after the tea or capsule. Drinking chamomile tea at lights-out is too late; the practical window is 45–90 minutes before intended sleep.
Stacking with other gentle nighttime herbs is reasonable and traditional. Common combinations:
- Chamomile + lemon balm — lemon balm (Melissa officinalis) also has gentle GABAergic activity, plus a pleasant lemon-citrus flavor that complements chamomile. See our Lemon Balm page.
- Chamomile + passionflower — passionflower (Passiflora incarnata) modulates GABA through a different mechanism, mostly via direct GABA-receptor binding rather than the BZD site. The combination is widely sold as a sleep tea blend.
- Chamomile + magnesium glycinate — magnesium is a separate GABAergic modulator at the NMDA receptor. Glycine (the carrier amino acid in magnesium glycinate) is itself an inhibitory neurotransmitter at spinal and brainstem glycine receptors. See our Magnesium Glycinate page.
- Chamomile + L-theanine + glycine — the "alpha-wave plus inhibitory amino acid" stack popular among biohacker / sleep-tracking enthusiasts.
Stacking with melatonin (for circadian phase shifting) and with valerian (for sleep-onset latency in severe insomnia) is also common. The combinations are additive in effect; none are synergistic to a degree that would replace prescription hypnotics in true severe insomnia, but for mild-to-moderate complaints they substantially reduce the perceived need for pharmaceutical options.
Pair with non-pharmacologic sleep hygiene: consistent sleep schedule, cool bedroom (65–68°F), blue-light avoidance for 1–2 hours before bed, no caffeine after noon. See our full Sleep Hygiene framework for the underlying behavioral foundation that any nighttime herb is meant to support, not replace.
Cautions and Interactions
- Asteraceae family allergy — chamomile is in the daisy/aster family (Asteraceae, also called Compositae) along with ragweed, daisy, marigold, and chrysanthemum. Individuals with documented ragweed allergy may cross-react to chamomile. Rare anaphylaxis has been reported. Caution in patients with known Asteraceae allergy.
- Anticoagulant interaction (theoretical) — chamomile contains small amounts of coumarin derivatives. The clinical magnitude of warfarin interaction is debated and probably small, but case reports exist. Patients on warfarin should mention chamomile use to their anticoagulation clinic.
- Pregnancy — small amounts of chamomile tea are widely consumed in pregnancy without apparent harm, but high-dose extracts and chamomile essential oil are not recommended. Some sources list chamomile as a uterine stimulant in concentrated form. Moderate tea use is generally considered acceptable; standardized extract capsules are not.
- Sedation with other CNS depressants — modest additive sedation with benzodiazepines, opioids, alcohol, and prescription hypnotics. Not a contraindication at typical doses but worth noting if multiple sedating substances are stacked.
- Cyclosporine and CYP3A4 substrates — apigenin is a weak CYP3A4 inhibitor in vitro. Clinical magnitude is probably small at typical chamomile doses but high-dose standardized extracts should be flagged in patients on narrow-therapeutic-index CYP3A4 substrates.
- Not a substitute for diagnosis — chronic insomnia (more than 3 months) warrants medical evaluation for sleep apnea, restless legs syndrome, depression, thyroid disease, and other treatable underlying causes. Chamomile is appropriate for short-term, mild, or transient sleep complaints; it should not delay workup of persistent severe insomnia.
Key Research Papers
- Adib-Hajbaghery M, Mousavi SN (2017). The effects of chamomile extract on sleep quality among elderly people: A clinical trial. Complementary Therapies in Medicine, 35:109-114. — PubMed
- Chang SM, Chen CH (2016). Effects of an intervention with drinking chamomile tea on sleep quality and depression in sleep disturbed postnatal women: a randomized controlled trial. Journal of Advanced Nursing, 72(2):306-315. — PubMed
- Zick SM et al. (2011). Preliminary examination of the efficacy and safety of a standardized chamomile extract for chronic primary insomnia: a randomized placebo-controlled pilot study. BMC Complementary and Alternative Medicine, 11:78. — PubMed
- Viola H et al. (1995). Apigenin, a component of Matricaria recutita flowers, is a central benzodiazepine receptors-ligand with anxiolytic effects. Planta Medica, 61(3):213-216. — PubMed
- Salehi B et al. (2019). The therapeutic potential of apigenin. International Journal of Molecular Sciences, 20(6):1305. — PubMed
- Avallone R et al. (2000). Pharmacological profile of apigenin, a flavonoid isolated from Matricaria chamomilla. Biochemical Pharmacology, 59(11):1387-1394. — PubMed
- Srivastava JK, Shankar E, Gupta S (2010). Chamomile: A herbal medicine of the past with bright future. Molecular Medicine Reports, 3(6):895-901. — PubMed
- Hieu TH et al. (2019). Therapeutic efficacy and safety of chamomile for state anxiety, generalized anxiety disorder, insomnia, and sleep quality: A systematic review and meta-analysis. Phytotherapy Research, 33(6):1604-1615. — PubMed
- Miraj S, Alesaeidi S (2016). A systematic review study of therapeutic effects of Matricaria recutita chamomile. Electronic Physician, 8(9):3024-3031. — PubMed
- Kasper S, Müller WE (2010). Phytopharmaceuticals for treating anxiety disorders — mechanism of action and recent clinical studies. — PubMed
- McKay DL, Blumberg JB (2006). A review of the bioactivity and potential health benefits of chamomile tea (Matricaria recutita L.). Phytotherapy Research, 20(7):519-530. — PubMed
- Gray SL et al. (2015). Cumulative use of strong anticholinergics and incident dementia: a prospective cohort study. JAMA Internal Medicine, 175(3):401-407. — PubMed
PubMed Topic Searches
- PubMed: Chamomile sleep quality RCTs
- PubMed: Apigenin and GABA-A receptor
- PubMed: Matricaria chamomilla insomnia
- PubMed: Chamomile elderly nursing-home sleep
- PubMed: Chamomile postpartum sleep
- PubMed: Diphenhydramine anticholinergic dementia risk
Connections
- Chamomile Overview
- Chamomile Benefits Hub
- Chamomile for Anxiety Relief
- Chamomile for Digestive and IBS
- Chamomile for Skin Healing
- Lemon Balm
- Lavender
- Passionflower
- Valerian
- Insomnia
- Anxiety
- Sleep Hygiene
- Natural Anxiety Relief
- All Herbs