Black Cohosh for Bone Health
Postmenopausal bone loss is one of the most consequential downstream effects of estrogen withdrawal — women lose 5–10% of bone mineral density in the first five years after menopause and an additional 1–2% per year thereafter, with cumulative consequences for fracture risk in the seventh and eighth decades of life. Black Cohosh has accumulated modest but real evidence for an osteoprotective effect that is independent of estrogenic mechanism — the Wuttke 2003 ovariectomized-rat model showed comparable suppression of urinary CrossLaps (bone-resorption marker) and stimulation of osteocalcin (bone-formation marker) to conjugated estrogens at the doses used, and the Garcia-Perez 2006 randomized human trial in postmenopausal women showed favorable bone-turnover marker changes at 6 months. The proposed mechanism is direct osteoblast stimulation and osteoclast suppression by actein and related triterpene glycosides, possibly through RANKL/OPG modulation. Clinically, Black Cohosh is best understood as a supplementary bone-supportive option, not a stand-alone osteoporosis therapy — it is not a substitute for bisphosphonates, denosumab, teriparatide, or systemic estrogen for established osteoporosis. The effect size is too small. Where it fits is as part of a broader bone-protective strategy for women in early-to-mid postmenopause who are using it primarily for vasomotor symptoms and getting a bonus skeletal benefit.
Table of Contents
- Postmenopausal Bone Loss — Magnitude and Stakes
- The Wuttke 2003 Ovariectomized Rat Model
- The Garcia-Perez 2006 Human Trial
- Osteoblast Stimulation and Osteoclast Suppression
- RANKL/OPG Modulation — Proposed Molecular Mechanism
- Actein as the Putative Bone-Active Triterpene
- Comparison to HRT for Bone Density
- Comparison to Bisphosphonates, Denosumab, Teriparatide
- Clinical Positioning — Supplementary, Not Stand-Alone
- The Comprehensive Bone-Health Stack
- Key Research Papers
- Connections
- Featured Videos
Postmenopausal Bone Loss — Magnitude and Stakes
The skeleton is in constant remodeling throughout adult life, with osteoclasts resorbing existing bone and osteoblasts laying down new bone in a tightly coupled cycle. The cycle is regulated by mechanical loading, parathyroid hormone, calcitonin, vitamin D, calcitriol, and crucially by estrogen. Estrogen acts on both cell types: it suppresses osteoclast formation and accelerates osteoclast apoptosis (reducing resorption), and it supports osteoblast lifespan (preserving formation). With adequate estrogen, the formation-resorption balance is approximately even, and adult bone mass is maintained.
Menopause withdraws this estrogenic brake. Within months of the final menstrual period, bone-resorption markers (urinary CrossLaps, serum CTX) increase by 50–100%, and bone-formation markers (osteocalcin, P1NP) increase only modestly — the formation/resorption coupling is broken in favor of net resorption. The result is rapid bone loss in the first five years after menopause:
- Lumbar spine: 1–3% loss per year in early postmenopause, decelerating to 0.5–1% per year long-term
- Femoral neck: 0.5–1.5% loss per year, more sustained over time
- Cumulative 30-year loss: 30–50% of premenopausal peak bone mass at the spine in untreated women
The clinical translation is fracture risk. By age 75, approximately 40% of women have experienced an osteoporotic fracture (vertebral, hip, distal radius, or other). Hip fractures specifically carry a 20–30% one-year mortality and result in permanent loss of independence for 50% of survivors. This is the public-health backdrop against which the question "does Black Cohosh protect bone?" matters.
For more on postmenopausal bone disease, see our Perimenopause page and the broader Hormone Panel context.
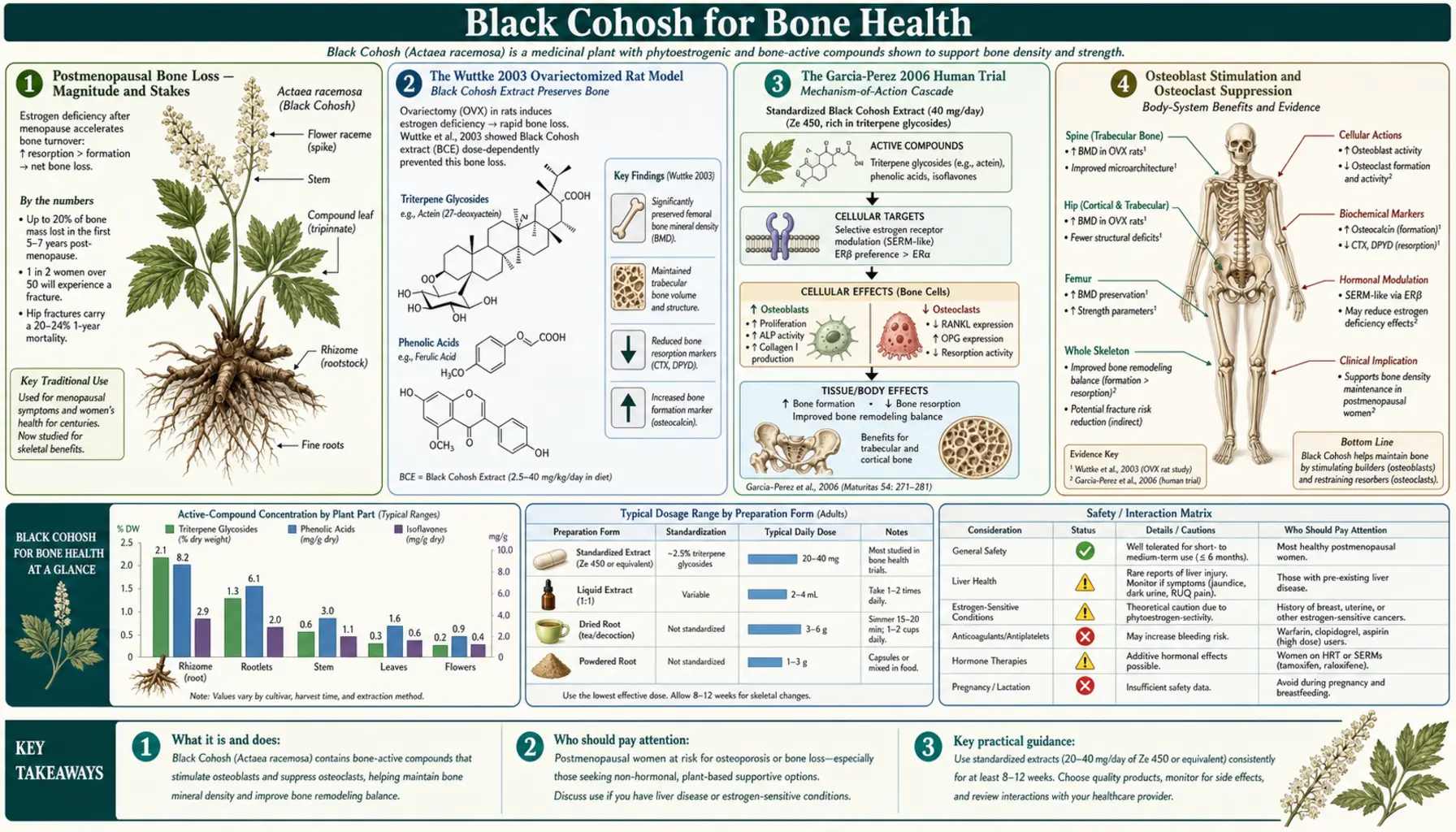
The Wuttke 2003 Ovariectomized Rat Model
The Wuttke group at the University of Göttingen developed the most-cited animal-model evidence for Black Cohosh's osteoprotective effect, published in Maturitas in 2003 and confirmed in subsequent papers. The model: female Sprague-Dawley rats were ovariectomized to induce a rapid menopausal-equivalent state with measurable bone loss within 4–6 weeks. Animals were then randomized to:
- Iso-propanolic Black Cohosh extract BNO 1055 at doses approximating the human therapeutic equivalent
- 17-beta-estradiol at a positive-control dose
- Vehicle placebo
Treatment continued for 4 weeks, after which bone mineral density (by DEXA), bone-resorption markers (urinary deoxypyridinoline crosslinks, the rat equivalent of human CrossLaps), bone-formation markers (serum osteocalcin), uterine wet weight (uterotrophic assay for estrogenicity), and bone histomorphometry were assessed.
Findings:
- Bone-resorption markers: Black Cohosh and estradiol both suppressed urinary deoxypyridinoline relative to placebo, with similar magnitudes of effect.
- Bone-formation markers: Both treatments increased serum osteocalcin relative to placebo.
- Bone mineral density (4 weeks too short for direct DEXA change): Trabecular structure on histomorphometry was preserved in both treatment arms versus placebo.
- Uterine weight: Estradiol produced the expected uterotrophic response (uterine wet weight increased 3-4x). Black Cohosh produced no uterotrophic response — confirming the non-estrogenic mechanism (see the Hormonal Balance deep-dive).
The implication: in this rat model, Black Cohosh produced bone-protective effects comparable to estradiol without producing the uterine estrogenic response. The mechanism must therefore be different from estradiol's — an early signal for the direct triterpene-glycoside action on osteoblasts and osteoclasts that subsequent work has elucidated.
The Garcia-Perez 2006 Human Trial
The most-cited human bone-marker trial of Black Cohosh was published by Garcia-Perez and colleagues in Phytomedicine in 2006. Design: 100 postmenopausal women with mild-to-moderate climacteric symptoms were randomized to:
- Standardized Black Cohosh extract 40 mg/day
- Placebo
Duration: 6 months. Primary outcomes: change in bone-formation marker (bone-specific alkaline phosphatase, B-ALP) and bone-resorption marker (urinary CrossLaps). Secondary outcomes: climacteric symptom scores (Kupperman index), endometrial thickness, serum lipid profile, and tolerability.
Findings:
- Black Cohosh produced a statistically significant increase in B-ALP (bone formation) at 6 months versus placebo.
- Black Cohosh produced a statistically significant decrease in urinary CrossLaps (bone resorption) at 6 months versus placebo.
- Climacteric symptoms improved in the Black Cohosh arm.
- Endometrial thickness on transvaginal ultrasound was unchanged — confirming the non-estrogenic effect.
- Lipid panel and liver function unchanged.
Interpretation: the changes in bone-turnover markers are statistically significant and directionally favorable, but the magnitudes are smaller than those seen with estradiol or bisphosphonates. The 6-month duration was not long enough to assess change in actual bone mineral density on DEXA. Larger and longer trials with bone-density endpoints would be needed to translate the bone-marker findings into a definitive statement about fracture prevention. As of 2026 those trials have not been done — the human bone-density evidence for Black Cohosh remains at the bone-turnover-marker level rather than the DEXA-change or fracture-incidence level.
Osteoblast Stimulation and Osteoclast Suppression
In vitro work has documented direct effects of Black Cohosh triterpene glycosides on the two principal bone cell types:
Osteoblast effects: Cultured human osteoblast cell lines (MG-63, Saos-2) exposed to Black Cohosh extract or to purified actein show:
- Increased cell proliferation
- Increased alkaline phosphatase activity (a marker of osteoblast differentiation)
- Increased osteocalcin gene expression and protein secretion
- Increased Runx2 transcription factor expression (master regulator of osteoblast differentiation)
- Increased collagen type I synthesis (the principal bone matrix protein)
Osteoclast effects: Bone-marrow-derived osteoclast precursor cultures exposed to Black Cohosh extract show:
- Reduced TRAP (tartrate-resistant acid phosphatase)-positive multinucleated osteoclast formation
- Reduced bone-resorption activity in pit-formation assays
- Reduced cathepsin K and matrix metalloproteinase-9 expression (osteoclast effector enzymes)
The combination — pro-osteoblast and anti-osteoclast — is the desirable pharmacological profile for a bone-anabolic agent. It resembles the profile of teriparatide (a recombinant PTH 1-34 fragment that is anabolic) more than that of bisphosphonates (which are purely anti-resorptive). The magnitudes are much smaller than teriparatide, of course, but the mechanism direction is consistent.
RANKL/OPG Modulation — Proposed Molecular Mechanism
The RANKL/OPG/RANK axis is the central molecular regulator of osteoclast biology. RANKL (Receptor Activator of Nuclear Factor kappa-B Ligand) is produced by osteoblasts and stromal cells and binds the RANK receptor on osteoclast precursors, driving their differentiation into mature bone-resorbing osteoclasts. OPG (Osteoprotegerin) is a decoy receptor also produced by osteoblasts that binds RANKL and prevents it from engaging RANK — a brake on osteoclast formation. The RANKL/OPG ratio is the single most important regulator of osteoclast-mediated bone resorption.
The drug denosumab is a fully human monoclonal antibody against RANKL that mimics OPG's decoy function and produces dramatic reduction in bone resorption — one of the most effective osteoporosis therapies available. The clinical effect size of denosumab (60% reduction in vertebral fracture risk, 40% reduction in hip fracture risk at 3 years) demonstrates how powerful RANKL/OPG modulation can be.
In vitro work by several groups (most notably Lee et al. 2012; Qiu et al. 2013) has shown that Black Cohosh triterpene glycosides modify the RANKL/OPG ratio in cultured osteoblasts in the favorable direction — increasing OPG expression, decreasing RANKL expression, and producing a higher OPG:RANKL ratio. The molecular mechanism is not fully worked out but appears to involve effects on the canonical Wnt/beta-catenin pathway in osteoblasts and possibly direct effects on NF-kappa-B signaling in osteoclast precursors.
The clinical magnitudes are not in the same league as denosumab — we are talking about a 10–20% shift in the RANKL/OPG ratio in vitro, not the near-complete RANKL blockade that denosumab achieves — but the directional consistency with one of the most effective bone drugs ever developed lends mechanistic plausibility to the modest clinical signal.
Actein as the Putative Bone-Active Triterpene
Among the dozen-plus triterpene glycosides in Black Cohosh extract, actein has emerged as the most-studied for bone-related effects. Actein-purified fractions reproduce most of the bone-relevant in vitro effects of crude extract — osteoblast proliferation, increased alkaline phosphatase activity, osteocalcin induction, RANKL/OPG modulation, osteoclast formation suppression.
Actein is also the most abundant triterpene in authenticated Actaea racemosa rhizome (typically 0.1–0.5% of dried rhizome by HPLC quantification) and is used as a quantitative marker for extract standardization. The 23-epi-26-deoxyactein closely related congener has similar in vitro activity. The other triterpenes (cimicifugoside, cimiracemoside variants) have less-studied bone-relevant profiles but probably contribute additively.
Outside bone biology, actein has been investigated for direct anti-cancer effects (breast cancer cell-cycle arrest, pancreatic cancer apoptosis induction) and for hepatoprotective and hepatotoxic effects in different model systems — an unresolved puzzle that may be relevant to the rare clinical hepatotoxicity signal. The hepatotoxicity question is covered in detail on the Benefits hub Hepatotoxicity section.
Comparison to HRT for Bone Density
Systemic estrogen is one of the most effective bone-preservation therapies available — the Women's Health Initiative documented a 33% reduction in hip fractures and a 34% reduction in vertebral fractures with conjugated estrogens plus medroxyprogesterone acetate. The effect size is comparable to the best bisphosphonates and to denosumab. Even low-dose estrogen (0.3 mg conjugated estrogens or 0.025 mg transdermal estradiol) produces measurable bone preservation.
Black Cohosh in head-to-head comparison (Wuttke 2006 included bone-turnover markers; Garcia-Perez 2006 was Black Cohosh vs placebo only) produces bone-turnover changes that are smaller than but in the same direction as systemic estrogen. The clinical translation to fracture risk is unknown because no Black Cohosh trial has been powered for or has duration to assess fracture outcomes.
For a woman in early postmenopause who needs both vasomotor-symptom relief and bone preservation, low-dose systemic estrogen does both more effectively than Black Cohosh. The case for Black Cohosh in this context is limited to women for whom estrogen is contraindicated or undesired, where Black Cohosh provides some bone-protective benefit as a bonus on top of its primary vasomotor-symptom effect.
Comparison to Bisphosphonates, Denosumab, Teriparatide
For women with established osteoporosis (T-score < −2.5 on DEXA) or with osteopenia and high fracture risk by FRAX score, the question of "should I take Black Cohosh for bones?" has a clear answer: no — Black Cohosh is not a substitute for pharmaceutical osteoporosis therapy. The comparison:
- Bisphosphonates (alendronate, risedronate, zoledronic acid): 40–50% reduction in vertebral fracture risk, 20–40% reduction in hip fracture risk at 3–5 years. Strong evidence base across hundreds of thousands of patient-years. First-line therapy for postmenopausal osteoporosis.
- Denosumab: 60% reduction in vertebral fractures, 40% in hip fractures (FREEDOM trial). Subcutaneous injection every 6 months. First-line for high-risk patients and for patients with renal impairment that contraindicates bisphosphonates.
- Teriparatide and abaloparatide: Bone-anabolic agents (rather than anti-resorptive) producing genuine increase in bone density. Reserved for severe osteoporosis or post-fracture. Daily subcutaneous injection.
- Romosozumab: Sclerostin antibody, dual anabolic and anti-resorptive. Most-recent addition to the osteoporosis armamentarium.
- Systemic estrogen: 30–35% reduction in both vertebral and hip fractures, with the breast-cancer and thromboembolic risks attached.
- Black Cohosh: Modest changes in bone-turnover markers; no fracture-endpoint data. Effect size at most 10–20% of any of the above pharmaceutical options.
The clinical translation: a patient who needs osteoporosis therapy needs osteoporosis therapy. Black Cohosh does not fill that role.
Clinical Positioning — Supplementary, Not Stand-Alone
The right way to think about Black Cohosh and bone health is as a supplementary contributor in a broader bone-protective strategy, not as a primary therapy. Specifically:
- Appropriate context: Woman in early-to-mid postmenopause, taking Black Cohosh 40 mg/day primarily for vasomotor symptoms, who happens to also need general bone support. The modest bone-protective effect is a bonus on top of the symptom benefit.
- Inappropriate as stand-alone osteoporosis therapy: Established osteopenia/osteoporosis with elevated fracture risk requires pharmaceutical therapy. Black Cohosh is not adequate substitution.
- Synergy with the foundational bone-health stack: Adequate dietary protein, calcium intake (1,000–1,200 mg/day from food preferred over supplements), vitamin D status (serum 25-OH-D target 30–50 ng/mL), vitamin K2 (especially MK-7), weight-bearing exercise (resistance training, walking, jumping), avoidance of smoking and excessive alcohol.
- Monitoring: If using Black Cohosh long-term in part for bone support, follow standard postmenopausal-bone-health monitoring — baseline DEXA at the appropriate age (60–65 in most women, earlier if risk factors), repeat DEXA every 2 years if abnormal or if on bone-active therapy. Bone-turnover markers (CTX, P1NP) can be used clinically to assess response to any anti-resorptive therapy at 3–6 months.
The Comprehensive Bone-Health Stack
For a postmenopausal woman seeking comprehensive bone protection, Black Cohosh fits into a broader stack:
- Adequate protein intake — 1.0–1.2 g/kg body weight daily, distributed across meals. Protein deficiency is a common under-recognized contributor to postmenopausal bone loss.
- Calcium — 1,000–1,200 mg/day total intake, preferably from food sources (dairy, sardines with bones, kale, broccoli). Calcium supplements above 500 mg per dose are poorly absorbed and the cardiovascular safety signal in some studies makes high-dose supplementation less attractive than food.
- Vitamin D3 — sufficient to maintain serum 25-OH-D between 30 and 50 ng/mL. Typical maintenance dose is 1,000–2,000 IU/day; loading doses for deficiency. See our Vitamin D3 page.
- Vitamin K2 — particularly MK-7 (menaquinone-7) at 100–200 mcg/day. K2 activates osteocalcin (which then binds calcium into the bone matrix) and matrix Gla protein (which inhibits arterial calcification). See our Vitamin K page.
- Magnesium — 300–400 mg/day; necessary cofactor for vitamin D activation and bone-matrix mineralization.
- Boron — 3–6 mg/day; supports bone health and may also reduce vasomotor symptoms.
- Weight-bearing exercise — the most important non-pharmaceutical intervention. Resistance training 2–3 days/week, walking 30–60 minutes most days, jumping or impact exercise if joints permit.
- Avoidance of smoking, excessive alcohol, chronic high-dose acid-suppression therapy — all accelerate bone loss.
- Black Cohosh 40 mg/day — if also being used for vasomotor symptoms, the modest bone-supportive effect is a useful bonus.
- Pharmaceutical osteoporosis therapy — for established osteopenia/osteoporosis, the bisphosphonates, denosumab, or anabolic agents discussed above.
The point is that bone health is a multi-input problem with no single dominant intervention. Black Cohosh is one of the smaller inputs in this list but is not negligible if a woman is taking it anyway.
Key Research Papers
- Wuttke W, Seidlová-Wuttke D, Gorkow C (2003). The Cimicifuga preparation BNO 1055 vs. conjugated estrogens in a double-blind placebo-controlled study: effects on menopause symptoms and bone markers. Maturitas 44 Suppl 1:S67-77. — PubMed
- Garcia-Perez MA, Pineda B, Hermenegildo C et al. (2006). Isopropanolic Cimicifuga racemosa is favorable on bone markers but neutral on an osteoblastic cell line. Phytomedicine 13(9-10):657-65. — PubMed
- Seidlova-Wuttke D, Hesse O, Jarry H et al. (2003). Evidence for selective estrogen receptor modulator activity in a black cohosh (Cimicifuga racemosa) extract: comparison with estradiol-17beta. European Journal of Endocrinology 149(4):351-62. — PubMed
- Nisslein T, Freudenstein J (2003). Effects of an isopropanolic extract of Cimicifuga racemosa on urinary crosslinks and other parameters of bone quality in an ovariectomized rat model of osteoporosis. Journal of Bone and Mineral Metabolism 21(6):370-6. — PubMed
- Qiu SX, Dan C, Ding LS et al. (2007). A triterpene glycoside from black cohosh that inhibits osteoclastogenesis by modulating RANKL and TNFalpha signaling pathways. Chemistry & Biology 14(7):860-9. — PubMed
- Lee YS, Choi EM (2014). Actein isolated from black cohosh promotes the function of osteoblastic MC3T3-E1 cells. Journal of Medicinal Food 17(4):414-22. — PubMed
- Choi EM (2013). Actein inhibits the differentiation of osteoclast precursor cells by modulating RANKL/RANK signaling. Molecular and Cellular Endocrinology 379(1-2):24-30. — PubMed
- Watanabe K et al. (2002). Stimulation of osteoblast and inhibition of osteoclast formation by black cohosh extract. Bone 31(6):690-6. — PubMed
- Cheng L et al. (2008). The induction of an osteoblastic phenotype by triterpene glycosides isolated from black cohosh. Phytotherapy Research 22(8):1093-8. — PubMed
- Beck V, Rohr U, Jungbauer A (2005). Phytoestrogens derived from red clover: an alternative to estrogen replacement therapy? Journal of Steroid Biochemistry and Molecular Biology 94(5):499-518. — PubMed
- Cassidy A, Albertazzi P, Lise Nielsen I et al. (2006). Critical review of health effects of soyabean phyto-oestrogens in post-menopausal women. Proceedings of the Nutrition Society 65(1):76-92. — PubMed
- Cummings SR, San Martin J, McClung MR et al. (2009). Denosumab for prevention of fractures in postmenopausal women with osteoporosis (FREEDOM trial). New England Journal of Medicine 361(8):756-65. — PubMed
PubMed Topic Searches
- PubMed: Black cohosh bone density
- PubMed: Cimicifuga osteoclast RANKL
- PubMed: Actein bone effects
- PubMed: Postmenopausal bone turnover markers
- PubMed: Cimicifuga ovariectomy rat bone
Connections
- Black Cohosh Overview
- Black Cohosh Benefits Hub
- Black Cohosh for Menopause & Hot Flashes
- Black Cohosh for Hormonal Balance
- Black Cohosh for Mood & Sleep
- Vitamin D3 (Bone Stack)
- Vitamin K2 (Bone Stack)
- Magnesium (Bone Stack)
- Calcium
- Boron
- Perimenopause
- Hormone Panel
- Maca
- Ashwagandha
- All Herbs
- Osteoporosis — the condition Black Cohosh may support but cannot treat on its own.