Black Cohosh for Menopause & Hot Flashes
Vasomotor symptoms — hot flashes and night sweats — affect approximately 75% of perimenopausal and postmenopausal women in Western populations and persist a median of 7.4 years (the long-running Study of Women's Health Across the Nation, SWAN). For women who cannot or choose not to use systemic hormone therapy, Black Cohosh is the most-studied herbal alternative. The pivotal Wuttke 2006 trial of the iso-propanolic extract Remifemin BNO 1055 demonstrated equivalence to 0.6 mg conjugated estrogens at 12 weeks for both the Kupperman menopause index and a daily hot-flash count, with a clean side-effect profile. The Cochrane 2012 review of 16 trials concluded the overall evidence is mixed but acknowledged the positive signal from the standardized iso-propanolic preparations. The canonical dose is 40 mg/day of standardized extract divided into one or two doses, with a realistic expectation that meaningful symptom reduction takes 4 to 8 weeks to develop and that 12 weeks is the typical timepoint at which efficacy is assessed.
Interactive Visualization Menopause — run the hormones down and set off a hot flash Empty the ovarian follicle pool and watch estradiol swing, then flatten, while FSH climbs — then trigger a hot flash and see the narrowed thermoneutral zone behind it. Launch →
Table of Contents
- The Vasomotor-Symptom Burden of Menopause
- The Wuttke 2006 BNO 1055 vs Conjugated Estrogens Trial
- Cochrane 2012 Review — Why the Evidence Looks Mixed
- The 40 mg/day Standardized Dose and 8–12 Week Timeline
- Extract Standardization — Why Brand Matters
- Comparison to HRT — When Black Cohosh Is the Right Choice
- Women with Breast-Cancer History
- Combination Protocols (Black Cohosh + St. John's Wort, SERMs)
- Non-Responders — What to Try Next
- Safety, Monitoring, and Discontinuation
- Key Research Papers
- Connections
- Featured Videos
The Vasomotor-Symptom Burden of Menopause
Hot flashes are not "just" an annoyance. The Study of Women's Health Across the Nation (SWAN), a multi-ethnic longitudinal cohort begun in 1994, has produced the most authoritative natural-history data we have. SWAN documented that 75% of women experience vasomotor symptoms during the menopause transition, that the median total duration of symptoms is 7.4 years, that African American women experience longer symptom duration (median 10.1 years) than non-Hispanic White women (6.5 years), and that women with severe symptoms have measurable disruptions in sleep, mood, cognitive function, work productivity, and cardiovascular risk markers.
The clinical impact: severe vasomotor symptoms triple the risk of clinically significant insomnia, double the rate of depressive symptoms during the perimenopausal window, and contribute to a measurable increase in systolic blood pressure, fasting glucose, and adverse cardiovascular events over the symptomatic years. This is not a "soft" indication — it is a major source of morbidity for the half of the adult population that lives through menopause.
Systemic estrogen therapy (transdermal estradiol or oral conjugated estrogens) reduces vasomotor symptoms by approximately 75–90% in randomized trials and remains the most effective therapy. For women who cannot use hormone therapy — due to personal or family breast-cancer history, prior thromboembolic disease, active liver disease, or simply patient preference — the non-hormonal options are SSRIs (paroxetine 7.5 mg/day is FDA-approved for vasomotor symptoms), SNRIs (venlafaxine 75 mg/day), gabapentin 300–900 mg/day, clonidine, and herbal therapies. Among the herbal options, Black Cohosh has by far the deepest clinical-trial evidence base.
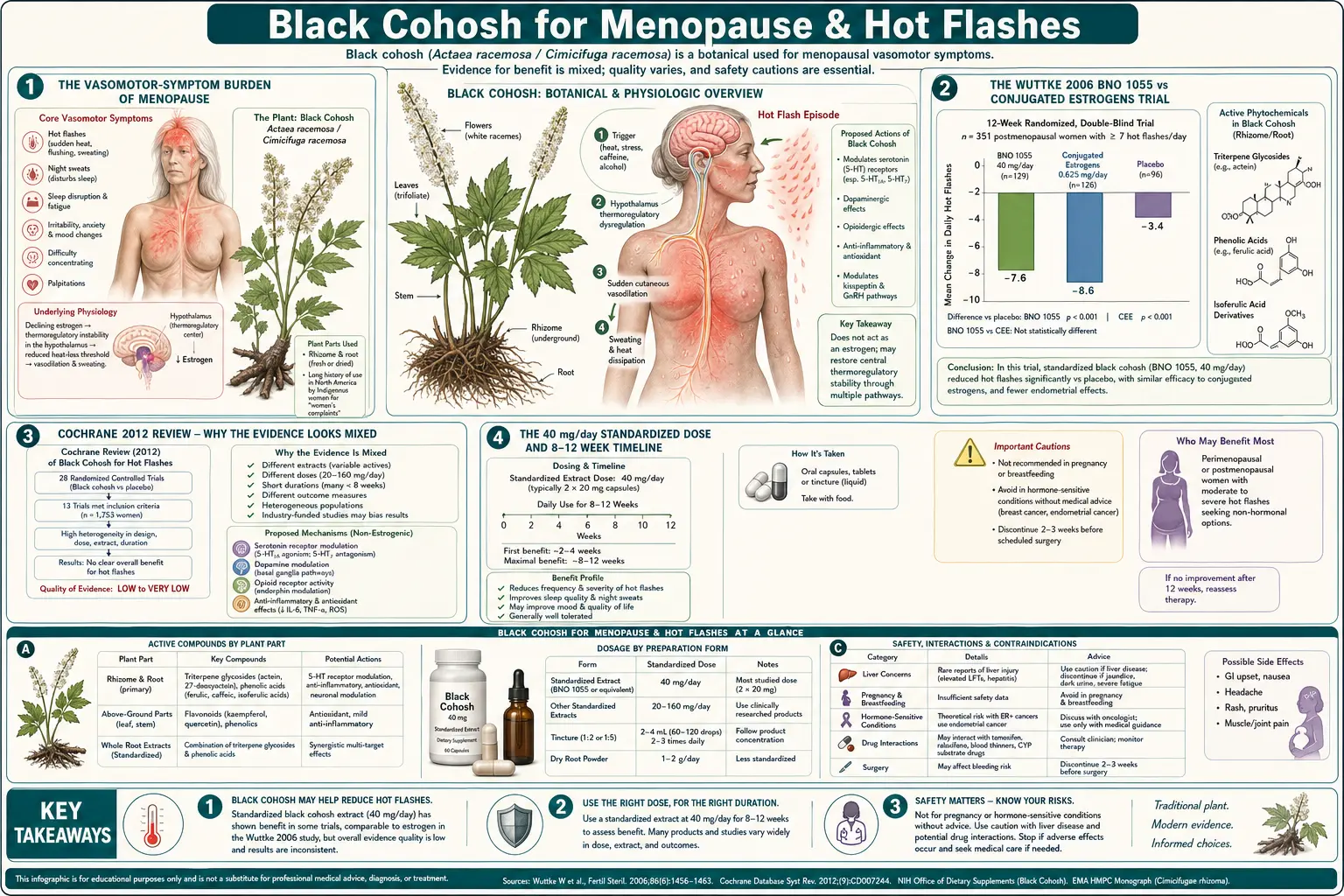
The Wuttke 2006 BNO 1055 vs Conjugated Estrogens Trial
The most influential single clinical trial of Black Cohosh for vasomotor symptoms was conducted by Wolfgang Wuttke and colleagues at the University of Göttingen, published in Maturitas in 2006 (the design and primary endpoints were reported earlier in Wuttke 2003, also in Maturitas). The trial was a three-arm randomized, double-blind, placebo-controlled comparison:
- Arm 1: Iso-propanolic Black Cohosh extract Remifemin BNO 1055, 40 mg/day (corresponding to 40 mg dried rhizome equivalent)
- Arm 2: Conjugated equine estrogens 0.6 mg/day (the low-dose Premarin formulation that became standard after the Women's Health Initiative results scaled back high-dose use)
- Arm 3: Matched placebo
62 postmenopausal women with menopausal symptoms were randomized for 12 weeks of treatment, with the Menopause Rating Scale (MRS) as the primary endpoint along with bone-formation markers (serum osteocalcin, bone-specific alkaline phosphatase) and bone-resorption markers (urinary CrossLaps). Key findings:
- MRS reduction: Black Cohosh arm reduced MRS by an average of 50%; conjugated estrogens arm reduced MRS by an average of 47%; placebo arm by 22%. The difference between active treatments and placebo was statistically significant for both; the difference between Black Cohosh and estrogens was not significant (equivalence).
- Hot-flash frequency: reduced from a baseline of 4.9 to 1.2 per day in the Black Cohosh arm and 4.7 to 1.3 in the estrogen arm; placebo reduced from 4.8 to 3.1.
- Bone markers: Both Black Cohosh and conjugated estrogens decreased the bone-resorption marker CrossLaps and increased the bone-formation marker osteocalcin, suggesting a positive net effect on bone remodeling for both treatments. Placebo showed no change.
- Endometrial thickness: Conjugated estrogens caused statistically significant endometrial thickening on transvaginal ultrasound at 12 weeks. Black Cohosh did NOT cause endometrial thickening — this is the strongest single piece of clinical evidence that Black Cohosh is not acting as an estrogen.
- Side effects: Both active arms had a low adverse-event rate; the only between-group difference was that the conjugated-estrogens arm had more breast tenderness and a small but real signal for breakthrough vaginal bleeding.
The Wuttke 2006 paper established BNO 1055 as the reference standard among Black Cohosh extracts and provided the strongest single piece of evidence for clinical equivalence to low-dose conjugated estrogens at 12 weeks. Critics have pointed out the small sample size (n=62) and the relatively short follow-up; defenders have pointed to the consistency with other Wuttke-group results and the mechanistic plausibility from the same group's receptor-binding studies. See the related Hormonal Balance deep-dive for the mechanism work.
Cochrane 2012 Review — Why the Evidence Looks Mixed
The Cochrane Collaboration published a systematic review and meta-analysis of Black Cohosh for menopausal symptoms in September 2012 (Leach & Moore, Cochrane Database CD007244). The review included 16 randomized controlled trials enrolling 2,027 perimenopausal and postmenopausal women, with treatment durations ranging from 8 to 52 weeks.
The headline conclusion was that "there is currently insufficient evidence to support the use of black cohosh for menopausal symptoms." The pooled analysis of standardized mean difference for hot-flash frequency was not statistically significant. This conclusion has been widely cited in subsequent reviews and clinical guidelines as evidence against Black Cohosh efficacy.
However, the Cochrane review also acknowledged substantial between-study heterogeneity (I-squared = 60–80% depending on outcome), and a subgroup analysis showed clear divergence between trials using the standardized iso-propanolic BNO 1055 extract (which showed benefit) and trials using other less-well-characterized preparations (which did not). The Cochrane authors explicitly noted that "future trials should use a well-characterised black cohosh preparation, such as the isopropanolic extract."
The interpretive question is whether the average effect across all preparations is the relevant clinical answer, or whether the effect of the best-studied preparation (BNO 1055) is the relevant answer for women considering using it. The German Commission E monograph and the European Medicines Agency herbal monograph both accept Black Cohosh as efficacious based largely on the BNO 1055 trials, while the U.S. NIH Office of Dietary Supplements takes a more cautious "evidence is mixed" position consistent with the Cochrane meta-analysis pooling all preparations together.
Two large negative U.S. trials are often cited as evidence against efficacy: the Newton 2006 HALT trial (Herbal Alternatives for Menopause, Annals of Internal Medicine) and the Reed 2008 trial (Menopause). Both used 160 mg/day of a CO2-extracted preparation (not BNO 1055) and showed no benefit over placebo. The interpretation depends on whether you believe the CO2 extract is pharmacologically equivalent to the iso-propanolic extract — the available phytochemical evidence suggests it is not.
The 40 mg/day Standardized Dose and 8–12 Week Timeline
The canonical evidence-based dose of Black Cohosh, derived from the Wuttke trials and the German Commission E monograph, is 40 mg/day of standardized iso-propanolic extract — the BNO 1055 / Remifemin preparation. This corresponds to a daily dose equivalent to 40 mg of dried rhizome, delivered as one tablet twice daily or two tablets once daily depending on the brand's standardization. The 40 mg figure refers to the dried-herb equivalent, not the mass of pure extract powder — this is a frequent source of consumer confusion.
Some clinicians, particularly in the U.S. integrative-medicine community, use higher doses (80–160 mg/day). The HALT and Reed trials used 160 mg/day. There is no clear dose-response evidence that higher doses produce greater efficacy — if anything, the negative high-dose U.S. trials suggest that more is not better, possibly because the active triterpene-glycoside profile is different in the higher-dose CO2 extracts. The 40 mg/day BNO 1055 dose remains the most-evidence-based starting point.
Timeline expectations:
- Week 1–2: Most patients notice no change. Some report mild GI upset that typically resolves with food. A small fraction notice mild headache.
- Week 3–4: Approximately 30–40% of responders begin to notice reduction in hot-flash intensity or frequency. The reduction is typically partial — flashes are shorter, less intense, or less frequent rather than disappearing entirely.
- Week 6–8: Most of the eventual benefit is established. This is the timepoint at which a fair assessment of efficacy can be made. Patients who have noticed no improvement at all by week 8 are unlikely to respond.
- Week 12: The standard trial-endpoint timepoint. By this point, responders typically have 40–60% reduction in hot-flash frequency and intensity.
- Beyond 12 weeks: Most responders experience sustained benefit on continued therapy. The longest published continuous-use trials extend to 12 months with maintained efficacy and no signal of tachyphylaxis.
Patients should be counseled at the start of therapy that Black Cohosh is not a "take and feel better the next day" therapy — the response timeline is comparable to that of an SSRI for depression, requiring weeks of consistent dosing before efficacy can be assessed. Premature discontinuation at week 2 or 3 because "it's not working" is one of the most common reasons for apparent treatment failure.
Extract Standardization — Why Brand Matters
"Black Cohosh" on a U.S. supplement label can refer to several pharmacologically distinct preparations:
- Iso-propanolic extract (BNO 1055 / Remifemin) — the original German pharmaceutical-grade preparation, extracted from authenticated Actaea racemosa rhizome with iso-propanol (40% v/v). Standardized to a defined triterpene-glycoside content. This is the preparation used in most positive clinical trials, including the Wuttke series.
- Ethanolic extract — alcoholic tinctures and dried extracts using ethanol as the solvent. Pharmacologically similar to iso-propanolic but with subtle differences in the extracted triterpene profile.
- CO2 supercritical extract — uses pressurized carbon dioxide as the solvent. Produces a different phytochemical profile, with lower polar triterpene-glycoside content. Used in the negative U.S. HALT and Reed trials.
- Methanolic / aqueous extract — less commonly marketed; phytochemically quite different.
- Bulk powdered rhizome — ground dried herb, no extraction. Cheap but inconsistent and the most likely to be adulterated with related Asian Cimicifuga species.
HPLC and DNA-barcoding analyses of U.S. retail Black Cohosh products have repeatedly documented adulteration rates of 10–30% with related but distinct species — primarily Cimicifuga foetida, C. heracleifolia, and C. dahurica, which are cheaper and more widely cultivated in China. These species have different triterpene profiles and unknown efficacy and safety profiles in humans. The most reliable way to avoid adulteration is to use a brand that publishes batch-level Certificates of Analysis with HPLC fingerprints and DNA authentication. Remifemin (the original iso-propanolic preparation, manufactured by Schaper & Brümmer in Germany and imported into the U.S. by Enzymatic Therapy) is the most-documented option.
Comparison to HRT — When Black Cohosh Is the Right Choice
Systemic estrogen therapy is more effective than Black Cohosh for vasomotor-symptom relief in head-to-head comparisons (Wuttke 2006 was an equivalence trial showing comparable effect at the doses used, but most non-equivalence studies have shown HRT outperforms Black Cohosh on hot-flash frequency by approximately 15–25%). HRT also produces additional benefits that Black Cohosh does not — reliable resolution of genitourinary syndrome of menopause (vaginal dryness, dyspareunia, urinary urgency), measurable preservation of bone density (Black Cohosh shows a smaller signal here, see the Bone Health deep-dive), and possible cardiovascular and cognitive benefits when initiated within the "window of opportunity" of approximately the first 10 years after menopause.
The case for Black Cohosh over HRT is built on situations where HRT is contraindicated, relatively contraindicated, or actively undesired by the patient:
- Personal history of estrogen-receptor-positive breast cancer — absolute contraindication to systemic estrogen. The non-estrogenic mechanism of Black Cohosh (see the Hormonal Balance deep-dive) makes it the most-studied herbal option for breast-cancer survivors with disabling vasomotor symptoms, though the evidence base in this specific population is still limited.
- Strong family history of breast or ovarian cancer — relative contraindication; many patients in this category prefer non-hormonal options regardless of formal guidelines.
- History of venous thromboembolism, pulmonary embolism, or stroke — oral conjugated estrogens carry a 2- to 3-fold elevated thrombotic risk. Transdermal estradiol is safer in this regard but still relatively contraindicated.
- Active liver disease — absolute contraindication to oral estrogens. Also a contraindication to Black Cohosh because of the rare idiosyncratic hepatotoxicity signal.
- Patient preference — many women have strong preferences for non-hormonal therapy for reasons that may include risk perception (often shaped by the 2002 Women's Health Initiative results, which were specific to oral conjugated estrogens plus medroxyprogesterone acetate in older women), religious or philosophical beliefs about pharmaceutical hormones, or prior negative experience with HRT.
- Mild-to-moderate vasomotor symptoms that don't require the full effect size of HRT — many women have symptoms that interfere with sleep and quality of life but don't rise to a level that demands the most effective therapy. Black Cohosh as a less-intensive option is reasonable.
Women with Breast-Cancer History
Breast-cancer survivors with disabling vasomotor symptoms (often induced or worsened by tamoxifen or aromatase-inhibitor therapy) face a specific clinical dilemma: systemic estrogen is absolutely contraindicated, and the antidepressants commonly used as alternatives can interact with tamoxifen metabolism (paroxetine and fluoxetine are strong CYP2D6 inhibitors and reduce conversion of tamoxifen to its active metabolite endoxifen — this interaction is clinically significant). Venlafaxine and gabapentin avoid the CYP2D6 issue but have their own side-effect burden.
The clinical-trial evidence for Black Cohosh in breast-cancer survivors is limited but encouraging. The Hernandez Munoz 2003 trial in 136 tamoxifen-treated breast-cancer patients found that 40 mg/day of standardized Black Cohosh extract reduced hot-flash severity significantly compared to placebo at 12 weeks, with no signal for adverse breast outcomes. The Pockaj 2006 NCCTG (North Central Cancer Treatment Group) randomized trial of 132 breast-cancer survivors using a non-iso-propanolic preparation showed no benefit over placebo — consistent with the broader observation that extract preparation matters.
The mechanistic case is strong (Black Cohosh does not bind estrogen receptors, does not stimulate MCF-7 breast-cancer cell proliferation, does not produce uterotrophic effects, and a 2011 Henneicke-von Zepelin analysis of German pharmacovigilance data found no signal for breast-cancer recurrence in long-term Black Cohosh users). The major North American Menopause Society (NAMS), German Commission E, and European Medicines Agency monographs all consider short-term Black Cohosh use acceptable in breast-cancer survivors after individual risk-benefit discussion with their oncologist.
The practical recommendation: for a breast-cancer survivor on tamoxifen with disabling hot flashes who is not getting relief from venlafaxine or gabapentin, a 12-week trial of 40 mg/day standardized iso-propanolic Black Cohosh extract is reasonable after baseline liver-function testing and with oncologist concurrence. The hepatotoxicity warnings apply with extra force in patients who may also be on hepatotoxic chemotherapy regimens.
Combination Protocols (Black Cohosh + St. John's Wort, SERMs)
Several combination products and protocols have been studied:
- Black Cohosh + St. John's Wort — the Uebelhack 2006 trial in 301 women with menopausal symptoms and significant mood symptoms tested a fixed combination (BNO 1055 + St. John's Wort 250 mg) against placebo for 16 weeks. The combination outperformed both placebo and the historical control of Black Cohosh alone, particularly on Hamilton Depression Rating Scale scores. The combination is marketed in Germany as Remifemin Plus. The interaction concern is that St. John's Wort is a potent CYP3A4 inducer — check for drug interactions before combining (tamoxifen, warfarin, oral contraceptives, immunosuppressants, anti-HIV drugs, and many anticonvulsants are all affected). See the Mood & Sleep deep-dive for more on the perimenopausal-mood applications.
- Black Cohosh + soy isoflavones — a logical combination since the two would act through different mechanisms (Black Cohosh non-estrogenic, soy mildly phytoestrogenic). Limited trial evidence; the few studies have not shown a clearly additive effect, and soy carries its own complexity for breast-cancer survivors.
- Black Cohosh + venlafaxine or paroxetine — not formally studied in randomized trials but commonly used clinically in patients who respond partially to either alone. No known pharmacokinetic interaction; reasonable empirical combination.
- Black Cohosh as bridge to or off HRT — some clinicians use Black Cohosh during HRT tapering to soften the rebound vasomotor symptoms that commonly occur. Limited evidence base but mechanistically reasonable.
Non-Responders — What to Try Next
If a patient has completed a 12-week trial of 40 mg/day standardized iso-propanolic Black Cohosh extract with no meaningful reduction in hot-flash frequency or intensity, the options in escalating order are:
- Confirm extract quality and adherence. A surprising fraction of "non-responders" turn out to have been taking a non-iso-propanolic preparation or have been inconsistent with dosing. Switch to authenticated BNO 1055 / Remifemin and confirm consistent twice-daily dosing for another 8 weeks before declaring non-response.
- Try higher dose (80 mg/day). Evidence for added benefit is weak but the safety profile at this dose is well-established. 8–12 week trial.
- Switch to or add a non-hormonal pharmaceutical. Paroxetine 7.5 mg/day (FDA-approved for vasomotor symptoms), venlafaxine 75 mg/day, gabapentin 300–900 mg/day at bedtime. Avoid paroxetine in tamoxifen-treated patients.
- Reconsider hormone therapy. For women without contraindications, low-dose transdermal estradiol (0.025–0.05 mg/day patch) is by far the most effective option and has the most favorable safety profile of all HRT formulations.
- Cognitive behavioral therapy for hot flashes (CBT-HF). A structured psychological intervention developed by Myra Hunter and colleagues that has shown 25–40% reduction in hot-flash bother (not necessarily frequency) in randomized trials. Especially useful for women who continue to have residual symptom impact despite partial response to other therapies.
- Lifestyle interventions: weight loss in overweight women (each 5 kg loss reduces hot-flash frequency measurably), reduction of alcohol and spicy foods (common individual triggers), bedroom temperature optimization, paced breathing.
Safety, Monitoring, and Discontinuation
The dominant safety concern is the rare idiosyncratic hepatotoxicity discussed in detail on the Benefits hub Hepatotoxicity section. The practical monitoring protocol:
- Baseline ALT, AST, alkaline phosphatase, total bilirubin before starting if any risk factor for liver disease is present (alcohol, statins, methotrexate, prior hepatitis, NASH).
- Repeat LFTs at 6 months for any user continuing beyond that timepoint.
- Annual LFTs for any user continuing >1 year.
- Immediate discontinuation at the first sign of jaundice, dark urine, RUQ pain, unusual fatigue, anorexia, or nausea. Get LFTs the same day.
Other safety considerations:
- Pregnancy and lactation: Contraindicated. Black Cohosh has uterotonic effects in vitro and has been used historically as a parturient to induce labor.
- Active liver disease: Absolute contraindication.
- Drug interactions: Limited evidence for clinically significant CYP-mediated interactions with Black Cohosh alone. Combination products with St. John's Wort carry the full set of St. John's Wort interactions (CYP3A4 induction).
- Common minor side effects: Mild GI upset (5–10% of users), headache (3–5%), rash (rare).
- Stopping after long-term use: No withdrawal syndrome. Vasomotor symptoms may return over 2–4 weeks after discontinuation if the underlying menopause physiology is still active.
Key Research Papers
- Wuttke W, Seidlová-Wuttke D, Gorkow C (2003). The Cimicifuga preparation BNO 1055 vs. conjugated estrogens in a double-blind placebo-controlled study: effects on menopause symptoms and bone markers. Maturitas 44 Suppl 1:S67-77. — PubMed
- Wuttke W, Raus K, Gorkow C (2006). Efficacy and tolerability of the Black cohosh (Actaea racemosa) ethanolic extract BNO 1055 on climacteric complaints: a double-blind, placebo- and conjugated estrogens-controlled study. Maturitas 55 Suppl 1:S83-91. — PubMed
- Leach MJ, Moore V (2012). Black cohosh (Cimicifuga spp.) for menopausal symptoms. Cochrane Database of Systematic Reviews 9:CD007244. — PubMed
- Newton KM et al. (2006). Treatment of vasomotor symptoms of menopause with black cohosh, multibotanicals, soy, hormone therapy, or placebo: a randomized trial (HALT). Annals of Internal Medicine 145(12):869-79. — PubMed
- Frei-Kleiner S, Schaffner W, Rahlfs VW et al. (2005). Cimicifuga racemosa dried ethanolic extract in menopausal disorders: a double-blind placebo-controlled clinical trial. Maturitas 51(4):397-404. — PubMed
- Pockaj BA et al. (2006). Phase III double-blind, randomized, placebo-controlled crossover trial of black cohosh in the management of hot flashes: NCCTG Trial N01CC. Journal of Clinical Oncology 24(18):2836-41. — PubMed
- Hernandez Munoz G, Pluchino S (2003). Cimicifuga racemosa for the treatment of hot flushes in women surviving breast cancer. Maturitas 44 Suppl 1:S59-65. — PubMed
- Uebelhack R et al. (2006). Black cohosh and St. John's wort for climacteric complaints: a randomized trial. Obstetrics & Gynecology 107(2 Pt 1):247-55. — PubMed
- Reed SD et al. (2008). Vaginal, endometrial, and reproductive hormone findings: randomized, placebo-controlled trial of black cohosh, multibotanical herbs, and dietary soy for vasomotor symptoms (HALT). Menopause 15(1):51-8. — PubMed
- Henneicke-von Zepelin HH (2017). 60 years of Cimicifuga racemosa medicinal products: clinical research milestones, current study findings and current development. Wiener Medizinische Wochenschrift 167(7-8):147-159. — PubMed
- Drewe J, Boonen G, Culmsee C (2015). Treatment of climacteric complaints with Cimicifuga racemosa: a series of in vitro experiments. Phytomedicine 22(13):1182-6. — PubMed
- Beer AM, Osmers R, Schnitker J et al. (2013). Efficacy of black cohosh (Cimicifuga racemosa) medicines for treatment of menopausal symptoms — comments on major statements of the Cochrane Collaboration report 2012. Gynecological Endocrinology 29(12):1022-5. — PubMed
PubMed Topic Searches
- PubMed: Black cohosh hot flashes RCTs
- PubMed: Cimicifuga menopause vasomotor
- PubMed: BNO 1055 Remifemin menopause
- PubMed: Black cohosh in breast cancer / tamoxifen
- PubMed: Actaea racemosa menopausal symptoms trials
Connections
- Menopause: Why the Hormones Fall and What Changes — interactive animation
- Black Cohosh Overview
- Black Cohosh Benefits Hub
- Black Cohosh for Hormonal Balance
- Black Cohosh for Bone Health
- Black Cohosh for Mood & Sleep
- Menopause
- Perimenopause
- Perimenopause Symptom Tracker
- Maca
- Ashwagandha
- Chamomile
- Hormone Panel
- Anxiety
- Depression
- Stress Management
- All Herbs