Black Cohosh for Hormonal Balance (Non-Estrogenic Mechanism)
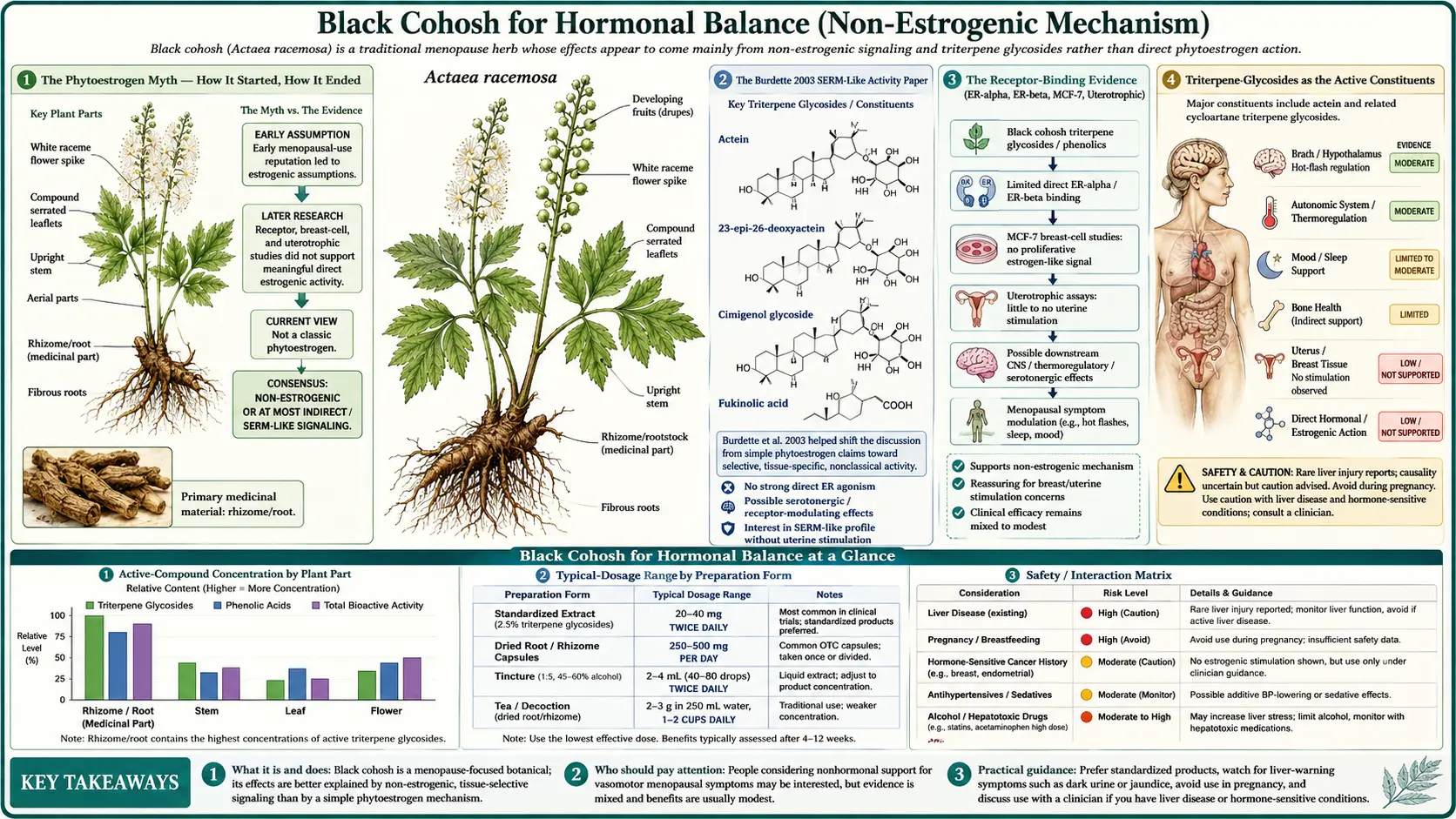
The single most important — and most commonly misunderstood — fact about Black Cohosh is that it is NOT a phytoestrogen. For most of the twentieth century, the herb was assumed to act like soy isoflavones or red clover — binding weakly to estrogen receptors, producing a partial-agonist effect that mimicked low-dose estrogen. That model was overturned by a series of rigorous receptor-binding, gene-expression, and animal-model studies between 2002 and 2008, most notably the Burdette 2003 demonstration that Black Cohosh extract acts as a mixed competitive ligand at the serotonin 5-HT7 receptor — not at estrogen receptors. The corrected mechanism is multi-target neurotransmitter modulation by the triterpene glycosides actein, 23-epi-26-deoxyactein, and cimicifugoside, with secondary contributions from cinnamic-acid esters. Clinically, this distinction matters enormously: women with estrogen-receptor-positive breast cancer history can use Black Cohosh under their oncologist's supervision in a way that they cannot use any true phytoestrogen.
Table of Contents
- The Phytoestrogen Myth — How It Started, How It Ended
- The Burdette 2003 SERM-Like Activity Paper
- The Receptor-Binding Evidence (ER-alpha, ER-beta, MCF-7, Uterotrophic)
- Triterpene Glycosides as the Active Constituents
- Serotonergic Mechanism (5-HT7, 5-HT1A)
- Dopaminergic and Opioid-Receptor Mechanisms
- Effects on the HPO Axis (FSH, LH, Estradiol, Prolactin)
- The KNDy Neuron Model and Why It Fits Black Cohosh
- Implications for Breast-Cancer Survivors
- What Black Cohosh Does Not Do (Genitourinary Symptoms, Bone — Mostly)
- Key Research Papers
- Connections
- Featured Videos
The Phytoestrogen Myth — How It Started, How It Ended
The "Black Cohosh is a phytoestrogen" idea originated in the 1980s, when European laboratory work suggested that crude Black Cohosh extracts had estrogen-like activity in some in vitro and animal-model assays. The compound formononetin — an isoflavonoid found in trace amounts in some Black Cohosh preparations — was identified as a possible candidate for the estrogenic activity. The story was clean, mechanistically appealing, and quickly absorbed into the herbal-medicine literature: a North American herb whose traditional use for menopausal symptoms made sense because it was a mild plant estrogen, like soy.
The story began to unravel in the mid-1990s when more careful analyses found that formononetin content in authenticated Actaea racemosa is too low to account for any clinical estrogenic effect — and that several of the original "estrogenic" Black Cohosh samples had been adulterated with red clover (which is genuinely high in formononetin). Receptor-binding studies with purified triterpene glycosides showed no measurable affinity for ER-alpha or ER-beta. Gene-expression studies of estrogen-responsive cells exposed to Black Cohosh extract showed no induction of the expected estrogen-target genes. The Wuttke group's 2003 ovariectomized-rat model showed no uterotrophic effect (a sensitive in vivo assay for estrogen activity).
The capstone study was Burdette 2003 (Journal of Agricultural and Food Chemistry), which used a panel of 33 receptor-binding assays to identify what the active extract was actually binding. The strongest hit was serotonin receptor 5-HT7 — not any estrogen receptor. Subsequent work by the Bolton laboratory at the University of Illinois at Chicago, the Wuttke laboratory at Göttingen, and several other groups built out a much more textured mechanism map involving serotonergic, dopaminergic, GABAergic, and mu-opioid pathways. The current scientific consensus, codified in the 2018 NAMS position statement, the European Medicines Agency monograph, and the German Commission E review, is unambiguous: Black Cohosh is not estrogenic.
The myth persists in consumer-facing materials, on supplement labels, and in many older medical and herbal-medicine textbooks because the correction is not commercially convenient — "natural plant estrogen for menopause" is a simpler marketing message than "multi-target serotonergic modulator with bone-protective triterpene glycosides." Clinicians counseling patients about Black Cohosh should be prepared to actively correct the phytoestrogen assumption.
The Burdette 2003 SERM-Like Activity Paper
Joanna Burdette and colleagues at the Bolton laboratory at the University of Illinois at Chicago published the paper that fundamentally changed the Black Cohosh mechanism story in Journal of Agricultural and Food Chemistry in 2003. The study took a methylene-chloride extract of authenticated Actaea racemosa rhizome and screened it against a panel of 33 receptors covering the major neurotransmitter systems (serotonin, dopamine, GABA, glutamate, opioid, adrenergic, histamine, acetylcholine).
The strongest binding was at the serotonin 5-HT7 receptor, with the extract acting as a mixed competitive ligand and partial agonist. The extract also bound the 5-HT1A and 5-HT1D receptors with somewhat lower affinity. Notably absent from the binding panel was any meaningful affinity for estrogen receptors (which were included in the assay set). The 5-HT7 receptor is particularly relevant because it is expressed in the hypothalamic preoptic area — the brain region that regulates core body temperature setpoint and that is centrally involved in the generation of hot flashes.
The therapeutic-equivalence comparison Burdette drew was to selective serotonin reuptake inhibitors (SSRIs). Paroxetine, venlafaxine, and other SSRIs/SNRIs reduce hot-flash frequency by approximately 30–50% in clinical trials — and these drugs work by increasing synaptic serotonin, which then engages serotonin receptors including 5-HT7. If Black Cohosh triterpene glycosides directly bind and partially agonize 5-HT7, the therapeutic effect should be analogous to that of an SSRI — which is exactly what the clinical trials show, both in magnitude and in time-course. The term "SERM-like" in Burdette's title was used in the broader sense of "selective effects mediated through receptor-level interaction" rather than the narrower "selective estrogen receptor modulator" sense; the receptor in question is 5-HT7, not the estrogen receptor.
The Receptor-Binding Evidence (ER-alpha, ER-beta, MCF-7, Uterotrophic)
A complete absence-of-effect case requires multiple independent lines of evidence. For the "Black Cohosh is not estrogenic" claim, the supporting evidence is:
- Direct ER-alpha and ER-beta radioligand-binding assays — Black Cohosh extract does not displace tritiated estradiol from either receptor isoform at any concentration tested (Liu 2001; Burdette 2003; Wuttke 2003). The IC50 is at or above the upper limit of solubility — effectively no binding.
- Estrogen-response-element (ERE) luciferase reporter assays — transfected cell lines expressing ER and an ERE-luciferase reporter construct produce a strong luminescent signal when exposed to estradiol or true phytoestrogens (genistein, daidzein). Black Cohosh extract produces no signal above background. Co-incubation with estradiol does not block the estradiol response (no antagonism).
- MCF-7 breast-cancer cell proliferation — the MCF-7 line is the standard in vitro screening tool for estrogenic activity. ER-alpha expression in MCF-7 drives proliferation in response to estrogens. Black Cohosh extract does not stimulate MCF-7 proliferation; some preparations actually suppress it. Critically, Black Cohosh does not block tamoxifen-induced growth inhibition (Bodinet 2002; Hostanska 2004) — if it were an estrogen agonist, it would partially reverse tamoxifen's effect, which it does not.
- Uterotrophic assay in ovariectomized rats — the classic in vivo sensitive assay for estrogen activity. An ovariectomized rat has minimal endogenous estrogen and a thin uterine epithelium. A true estrogen, given for 3 days, induces measurable uterine weight increase and epithelial thickening. Black Cohosh extract at therapeutic equivalent doses produces no uterotrophic response (Wuttke 2003; Bolle 2007). In contrast, conjugated estrogens produce a robust response in the same model.
- Endometrial thickness in clinical trials — the human equivalent of the uterotrophic assay. The Wuttke 2006 trial directly compared Black Cohosh BNO 1055 to conjugated estrogens for 12 weeks with transvaginal ultrasound monitoring. The estrogen arm produced measurable endometrial thickening; the Black Cohosh arm did not. This is arguably the strongest single piece of in vivo human evidence for the non-estrogenic claim.
- Vaginal cytology (Frank/Papanicolaou) maturation index — estrogen causes vaginal-epithelial maturation toward squamous cells with cornified nuclei; the Frank/Papanicolaou maturation index is sensitive to estrogen exposure. Liske 2002 included this endpoint and found no estrogen-like maturation effect from Black Cohosh.
The convergence across six independent assay systems — three in vitro, two animal-model, one human clinical — is what gives the non-estrogenic conclusion its weight.
Triterpene Glycosides as the Active Constituents
Phytochemical fractionation studies have identified the triterpene glycosides as the dominant pharmacologically active class in Actaea racemosa rhizome. The principal compounds are:
- Actein — the most abundant; used as a quantitative marker for extract standardization. Has been studied for anti-cancer effects in breast and pancreatic cell lines and for bone-stimulatory effects.
- 23-epi-26-deoxyactein (formerly called 27-deoxyactein) — chemically related to actein; the second most abundant. Shows similar serotonergic and bone-stimulatory activity in in-vitro assays.
- Cimicifugoside — structurally distinct triterpene glycoside.
- Cimiracemoside A–F — a family of related triterpene glycosides specific to A. racemosa, used as chemotaxonomic markers to distinguish authentic North American Black Cohosh from the adulterating Asian Cimicifuga species.
The triterpene glycosides are not water-soluble; they extract preferentially into iso-propanol, ethanol, or methylene chloride. This explains why the iso-propanolic extract Remifemin BNO 1055 has the most-studied pharmacological profile — the extraction solvent matches the solubility profile of the active compounds. Aqueous teas and water-extracted preparations contain a different and probably less active phytochemical profile.
The cinnamic-acid esters (fukinolic acid, cimicifugic acids A–F) are secondary contributors. Some in vitro work suggests these compounds have antioxidant and anti-inflammatory activity that may contribute to the overall clinical effect, but they are not the primary mediators of the serotonergic and hormonal effects.
Serotonergic Mechanism (5-HT7, 5-HT1A)
The serotonergic mechanism is the most-studied and most-likely-relevant for the clinical effect on hot flashes. The relevant pharmacology:
- 5-HT7 receptor — Gs-coupled receptor expressed in the hypothalamic preoptic area, the suprachiasmatic nucleus, the cortex, and several limbic structures. Centrally involved in thermoregulatory setpoint, circadian rhythm, and mood. 5-HT7 antagonism produces antidepressant-like and pro-thermoregulatory effects in animal models. Black Cohosh extract acts as a mixed-competitive partial agonist (Burdette 2003; Powell 2008) — meaning it both displaces serotonin from the receptor and partially activates the receptor itself, producing a net effect that resembles low-level chronic 5-HT7 stimulation.
- 5-HT1A receptor — Gi-coupled receptor expressed on serotonergic neurons (autoreceptor) and on hippocampal and cortical pyramidal neurons (heteroreceptor). 5-HT1A is the principal target of the anxiolytic drug buspirone. Black Cohosh extract has weaker but measurable 5-HT1A binding (Burdette 2003), which is the mechanistic basis for the modest anxiolytic effect documented in the Mood & Sleep deep-dive.
- 5-HT1D receptor — weaker binding; clinical significance unclear.
The 5-HT7 binding maps cleanly to the clinical effect: the hypothalamic preoptic area integrates serotonergic, noradrenergic, and KNDy-neuron signals to set the core temperature setpoint. The narrowed thermoneutral zone characteristic of menopause — where small upward shifts in core temperature trigger a vasodilation-and-sweating heat-dissipation cascade that the patient experiences as a hot flash — is partly serotonin-mediated. Drugs that increase serotonergic tone (SSRIs, SNRIs) widen the thermoneutral zone and reduce hot flashes. Black Cohosh, by partially agonizing 5-HT7 in the preoptic area, produces a similar widening with a different molecular mechanism.
Dopaminergic and Opioid-Receptor Mechanisms
Dopaminergic activity: In vitro studies (Jarry 2003; Powell 2008) have documented Black Cohosh extract binding to dopamine D2 receptors with moderate affinity. The D2 receptor is the primary target of prolactin-suppressing drugs like bromocriptine and cabergoline (D2 agonism on lactotrophs in the anterior pituitary suppresses prolactin secretion). Some clinical studies have documented mild prolactin reduction in women on Black Cohosh, consistent with weak D2 agonism. The dopaminergic effect may also contribute to mood modulation through mesolimbic and tuberoinfundibular pathways. The clinical magnitude is modest — Black Cohosh is not a substitute for cabergoline in true hyperprolactinemia and is not a clinically significant antipsychotic-effect modifier.
Mu-opioid receptor activity: Reame and colleagues (2008) documented binding of Black Cohosh triterpene-glycoside fractions to mu-opioid receptors in rat brain homogenates and in cultured neuronal cells. The clinical significance is debated. The opioid-receptor hypothesis is mechanistically interesting because the hypothalamic KNDy-neuron system (kisspeptin/neurokinin B/dynorphin) that is now understood as the central regulator of vasomotor symptoms is itself opioid-modulated — dynorphin is a kappa-opioid agonist and is a key inhibitory signal in the KNDy negative-feedback loop. A drug that engages opioid receptors in this circuit could plausibly modulate the entire vasomotor-symptom-generating system. This remains an active research area without clear clinical-evidence translation yet.
The opioid hypothesis also raises a safety question: is there any risk of opioid-receptor desensitization, tolerance, or withdrawal with chronic Black Cohosh use? The clinical-trial data through 12 months of use show no withdrawal syndrome on discontinuation and no progressive tolerance, but the data do not address all the questions that the opioid mechanism raises. This is one reason that clinically the recommendation is to limit Black Cohosh courses to 6–12 months with monitoring rather than indefinite use.
Effects on the HPO Axis (FSH, LH, Estradiol, Prolactin)
If Black Cohosh were genuinely estrogenic, you would expect to see negative-feedback suppression of FSH (which is elevated in postmenopausal women due to loss of ovarian estrogen feedback). You would expect to see suppression of LH for the same reason. You would expect to see measurable serum estradiol elevation if the herb itself or its metabolites were binding circulating sex-hormone-binding globulin or being measured in the estradiol immunoassay. None of these are observed.
- FSH: Multiple clinical trials (Liske 2002; Bai 2007; Wuttke 2006) have measured serum FSH before and after Black Cohosh treatment for 12–52 weeks. No statistically significant change. This is a strong piece of evidence that the hypothalamic-pituitary system does not perceive the herb as estrogen.
- LH: Same pattern — no change in serum LH on Black Cohosh therapy.
- Estradiol: No change in serum estradiol measured by immunoassay or LC-MS/MS. Black Cohosh metabolites do not cross-react with the standard estradiol assays.
- SHBG: No change in sex-hormone-binding globulin (which is upregulated by oral estrogen exposure via first-pass hepatic effect).
- Prolactin: Slight reduction documented in some studies; consistent with the weak D2-agonist activity described above.
- Inhibin B, AMH, kisspeptin: Not systematically studied. Would be interesting follow-up given the KNDy hypothesis.
The clinical implication for hormone monitoring: women on Black Cohosh do not need ongoing hormone-level monitoring to assess efficacy or safety from a hormonal-axis standpoint. Symptom response and liver-function monitoring are the relevant clinical parameters. See the Hormone Panel page for the relevant baseline-assessment context.
The KNDy Neuron Model and Why It Fits Black Cohosh
The current best model of hot-flash generation centers on the KNDy neurons — arcuate-nucleus neurons that co-express kisspeptin, neurokinin B, and dynorphin. In premenopausal women, these neurons receive negative-feedback signals from circulating estrogen, which keeps their tonic firing rate suppressed. After menopause, estrogen drops, the KNDy neurons hypertrophy (documented in human autopsy studies), and their now-disinhibited firing produces a heightened input to the hypothalamic thermoregulatory center.
The KNDy neurons release neurokinin B (an NK3 receptor agonist) onto the preoptic-area thermoregulatory neurons, which narrows the thermoneutral zone and triggers a heat-dissipation cascade (cutaneous vasodilation, sweating) at lower-than-normal core-temperature triggers. The clinical proof of this mechanism came in 2019–2020 with the demonstration that NK3-receptor antagonists (fezolinetant, elinzanetant) reduce hot-flash frequency by 60–75% in randomized trials — an effect size approaching that of systemic estrogen. Fezolinetant was approved by the FDA in 2023 for moderate-to-severe vasomotor symptoms; elinzanetant followed in 2024.
The KNDy model is relevant to Black Cohosh because the proposed serotonergic, dopaminergic, and opioid mechanisms of Black Cohosh all converge on the KNDy neurons and their downstream targets. 5-HT7 stimulation in the preoptic area widens the thermoneutral zone. D2 agonism in the arcuate nucleus modulates KNDy firing. Mu-opioid engagement parallels endogenous dynorphin's inhibitory role within the KNDy cell itself. The molecular targets are different from NK3 antagonism but the system-level effect is similar — restoration of a wider thermoneutral zone — which is consistent with the observation that the clinical effect size of Black Cohosh (40–50% hot-flash reduction in responders) is intermediate between placebo (~20%) and systemic estrogen or NK3 antagonists (~75%).
This converging-pathway model also helps explain why Black Cohosh and SSRIs/SNRIs produce roughly similar clinical effect sizes — both modulate the serotonergic input to the same hypothalamic circuit, by different molecular mechanisms.
Implications for Breast-Cancer Survivors
The non-estrogenic mechanism is the single most clinically consequential fact about Black Cohosh because it opens up a use case that is unavailable for any true phytoestrogen: management of vasomotor symptoms in women with personal history of estrogen-receptor-positive breast cancer.
The supporting evidence is substantial:
- In vitro: Black Cohosh extract does not stimulate MCF-7 proliferation; some preparations suppress it; it does not block tamoxifen's growth-inhibitory effect.
- Animal models: Black Cohosh in mammary-tumor-bearing rodents does not accelerate tumor growth; some models show modest tumor-growth suppression.
- Clinical trials in breast-cancer survivors: The Hernandez Munoz 2003 trial in 136 tamoxifen-treated patients showed Black Cohosh reduced hot-flash severity with no adverse breast outcomes. The Rostock 2011 observational cohort followed 50,000 patient-years of Black Cohosh use in breast-cancer survivors via German pharmacovigilance and found no signal for recurrence.
- 2018 NAMS position statement: Includes Black Cohosh as one of the acceptable non-hormonal options for vasomotor symptoms in breast-cancer survivors after individualized risk-benefit discussion with the oncologist.
The practical recommendation: for a postmenopausal breast-cancer survivor on tamoxifen or an aromatase inhibitor with disabling vasomotor symptoms, after consultation with the oncologist, a 12-week trial of 40 mg/day standardized iso-propanolic Black Cohosh extract is reasonable. The principal monitoring requirement is liver function (the hepatotoxicity warning applies with extra force in patients who may be on hepatotoxic chemotherapy). Drug-interaction screening is needed for any concomitant pharmaceutical regimen. See the Menopause & Hot Flashes deep-dive for the trial-specific evidence.
What Black Cohosh Does Not Do (Genitourinary Symptoms, Bone — Mostly)
Honest counseling about Black Cohosh requires being clear about what it does not address well:
- Genitourinary syndrome of menopause (GSM) — vaginal dryness, vulvar atrophy, dyspareunia, urinary urgency and recurrent UTI. These symptoms are driven by direct loss of estrogen action on the vaginal and vulvar epithelium and urinary tract. They respond well to local vaginal estrogen (which has minimal systemic absorption and is safe in most breast-cancer survivors after oncologist consultation), to ospemifene (an oral SERM), to DHEA prasterone (vaginal), and to vaginal moisturizers. Black Cohosh, lacking estrogenic action, does not address GSM. Patients with vasomotor symptoms plus GSM may need combination therapy.
- Bone protection (mostly) — Black Cohosh shows a measurable but small positive effect on bone-resorption markers in clinical trials. It is not a substitute for bisphosphonates, denosumab, teriparatide, or systemic estrogen for established osteoporosis. See the Bone Health deep-dive for the detail.
- Cardiovascular and cognitive benefits associated with HRT — not demonstrated for Black Cohosh.
- Severe depressive episodes — Black Cohosh has mild anxiolytic and mood-stabilizing activity but does not substitute for SSRI/SNRI therapy in moderate-to-severe major depression. The combination with St. John's Wort (Remifemin Plus) addresses milder mood symptoms; see the Mood & Sleep deep-dive.
- Severe vasomotor symptoms unresponsive to first-line therapy — for the most severe cases, the new NK3 antagonists (fezolinetant, elinzanetant) and systemic estrogen produce the largest effect size; Black Cohosh effect size is intermediate.
Key Research Papers
- Burdette JE, Liu J, Chen SN et al. (2003). Black cohosh acts as a mixed competitive ligand and partial agonist of the serotonin receptor. Journal of Agricultural and Food Chemistry 51(19):5661-70. — PubMed
- Liu J, Burdette JE, Xu H et al. (2001). Evaluation of estrogenic activity of plant extracts for the potential treatment of menopausal symptoms. Journal of Agricultural and Food Chemistry 49(5):2472-9. — PubMed
- Wuttke W, Jarry H, Becker T et al. (2003). Phytoestrogens: endocrine disrupters or replacement for hormone replacement therapy? Maturitas 44 Suppl 1:S9-20. — PubMed
- Bodinet C, Freudenstein J (2002). Influence of Cimicifuga racemosa on the proliferation of estrogen receptor-positive human breast cancer cells. Breast Cancer Research and Treatment 76(1):1-10. — PubMed
- Hostanska K, Nisslein T, Freudenstein J et al. (2004). Cimicifuga racemosa extract inhibits proliferation of estrogen receptor-positive and negative human breast carcinoma cell lines by induction of apoptosis. Breast Cancer Research and Treatment 84(2):151-60. — PubMed
- Powell SL et al. (2008). In vitro serotonergic activity of black cohosh and identification of N(omega)-methylserotonin as a potential active constituent. Journal of Agricultural and Food Chemistry 56(24):11718-26. — PubMed
- Reame NE et al. (2008). Black cohosh has central opioid activity in postmenopausal women: evidence from naloxone blockade and positron emission tomography neuroimaging. Menopause 15(5):832-40. — PubMed
- Jarry H, Metten M, Spengler B et al. (2003). In vitro effects of the Cimicifuga racemosa extract BNO 1055. Maturitas 44 Suppl 1:S31-8. — PubMed
- Bolle P, Mastrangelo S, Perrone F et al. (2007). Estrogen-like effect of a Cimicifuga racemosa extract sub-fraction as assessed by in vivo, ex vivo and in vitro assays. Journal of Steroid Biochemistry and Molecular Biology 107(3-5):262-9. — PubMed
- Ruhlen RL et al. (2007). Black cohosh: insights into its mechanism(s) of action. Integrative Medicine Insights 2:21-32. — PubMed
- Rostock M, Fischer J, Mumm A et al. (2011). Black cohosh (Cimicifuga racemosa) in tamoxifen-treated breast cancer patients with climacteric complaints — a prospective observational study. Gynecological Endocrinology 27(10):844-8. — PubMed
- Henneicke-von Zepelin HH, Meden H, Kostev K et al. (2007). Isopropanolic black cohosh extract and recurrence-free survival after breast cancer. International Journal of Clinical Pharmacology and Therapeutics 45(3):143-54. — PubMed
PubMed Topic Searches
- PubMed: Black cohosh receptor binding
- PubMed: Cimicifuga 5-HT7 mechanism
- PubMed: Actein triterpene glycoside
- PubMed: Black cohosh breast cancer safety
- PubMed: KNDy / NK3 menopause
Connections
- Black Cohosh Overview
- Black Cohosh Benefits Hub
- Black Cohosh for Menopause & Hot Flashes
- Black Cohosh for Bone Health
- Black Cohosh for Mood & Sleep
- Perimenopause
- Perimenopause Symptom Tracker
- Polycystic Ovary Syndrome
- Hormone Panel
- Maca
- Ashwagandha
- Chamomile
- Lemon Balm
- Stress Management
- All Herbs