Black Cohosh — Benefits Deep Dive
Black Cohosh (Actaea racemosa, formerly Cimicifuga racemosa) is a North American woodland perennial whose dark, gnarled rhizome was used for centuries by Native American peoples — the Cherokee, Iroquois, Algonquian, and Penobscot — for "female complaints," rheumatism, and as a parturient. Nineteenth-century Eclectic physicians adopted it under the common name "squaw root" or "black snakeroot." Modern phytochemistry has identified the dominant active constituents as triterpene glycosides (actein, 23-epi-26-deoxyactein, cimiracemoside, cimicifugoside) along with cinnamic-acid esters and small amounts of formononetin. For nearly a century the herb was assumed to be a phytoestrogen, but rigorous receptor-binding and microarray studies after 2002 have established that it is NOT estrogenic — it does not bind ER-alpha or ER-beta, does not stimulate estrogen-responsive breast tissue, and does not induce uterine proliferation. The true mechanism is multi-target serotonergic, dopaminergic, GABAergic, and opioid-receptor modulation by the triterpene glycosides. Black Cohosh is one of the most-studied herbs in the world for menopausal symptoms, with the Wuttke 2006 BNO 1055 trial demonstrating equivalence to low-dose conjugated estrogens for hot flashes and a 50% reduction in Kupperman menopause-index scores at 12 weeks. Four benefit pages below cover the clinical evidence, the mechanism controversy, the bone-density signal, and the perimenopausal mood/sleep applications.
Deep-Dive Articles
Menopause & Hot Flashes
The Wuttke 2006 BNO 1055 trial comparing Remifemin to 0.6 mg conjugated estrogens, the Cochrane 2012 mixed-evidence review, the canonical 40 mg/day standardized iso-propanolic extract dose, the 8–12 week response timeline (most patients see benefit by week 4), comparison to HRT for women with breast-cancer history, and why the trial-to-trial heterogeneity exists (extract standardization, placebo response, study population).
Hormonal Balance (Non-Estrogenic Mechanism)
Why the long-assumed phytoestrogen label is wrong, the Burdette 2003 SERM-like activity paper that overturned the consensus, triterpene-glycoside binding to serotonin 5-HT7 and 5-HT1A receptors, dopamine D2 modulation, mu-opioid receptor engagement, the absence of effect on FSH/LH/estradiol/prolactin, and the practical implication for women with estrogen-sensitive breast cancer history.
Bone Health
Postmenopausal bone-density data from the Wuttke 2003 ovariectomized-rat model and the Garcia-Perez 2006 human trial, comparison to estradiol's osteoprotective effect, the proposed actein-mediated osteoblast stimulation and osteoclast suppression mechanism, RANKL/OPG modulation, and the clinical reality that Black Cohosh is supplementary — not a stand-alone osteoporosis therapy.
Mood & Sleep
Perimenopausal mood swings and anxiety, the Liske 2002 anxiety subscale data from the Hamilton Anxiety Scale, traditional Native American (Cherokee, Iroquois) use as a parturient and nervine, the serotonergic and GABAergic mechanism behind the mood effect, sleep-architecture improvements in vasomotor-symptom-driven insomnia, and combination protocols with St. John's Wort for moderate depression in perimenopause.
Table of Contents
- Deep-Dive Articles
- Why Black Cohosh Produces Effects (Multi-Mechanism with Controversy)
- CRITICAL Hepatotoxicity Warning
- Key Research Papers
- External Authoritative Resources
- Connections
- Featured Videos
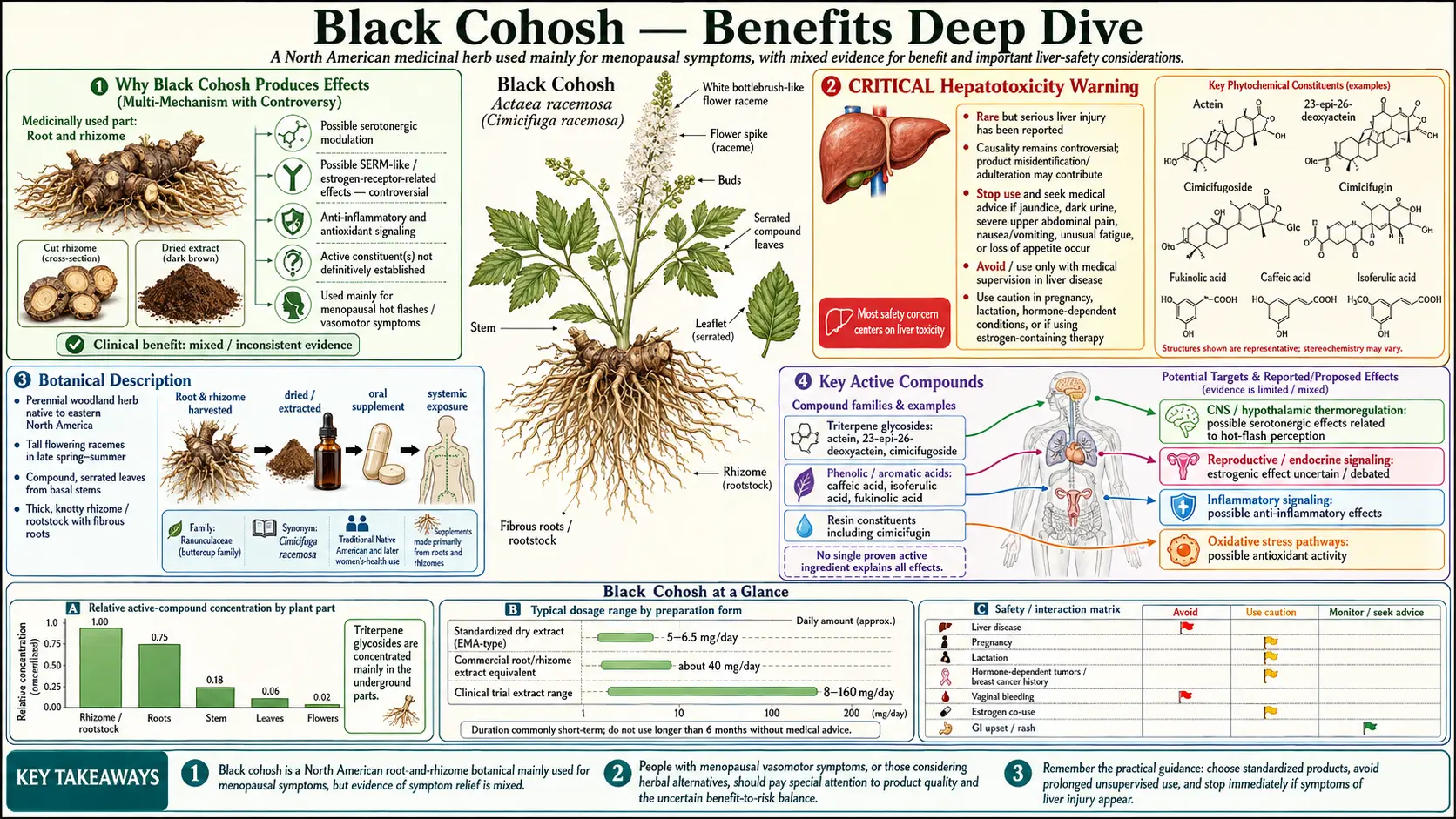
Why Black Cohosh Produces Effects (Multi-Mechanism with Controversy)
Most herbal therapies for menopausal symptoms (red clover, soy isoflavones, hops) are phytoestrogens — plant compounds that bind weakly to estrogen receptors and produce a partial-agonist effect. Black Cohosh is the conspicuous exception. For most of the 20th century it was assumed to belong to the same category, but a series of receptor-binding and gene-expression studies after 2002 systematically dismantled that assumption. The truth is more interesting: the active triterpene glycosides act through at least four distinct non-estrogenic pathways, each contributing to the clinical effect.
- Serotonergic activity — triterpene glycosides bind to serotonin 5-HT7 and 5-HT1A receptors. The 5-HT7 binding is the most-studied (Burdette 2003) and mechanistically explains the thermoregulatory effect on hot flashes, because the 5-HT7 receptor in the hypothalamic preoptic area is centrally involved in core-temperature setpoint regulation. The 5-HT1A binding contributes to anxiolytic and mood-stabilizing effects, similar in pathway (though weaker in magnitude) to buspirone. See the Mood & Sleep deep-dive for the clinical applications.
- Dopaminergic modulation — in vitro studies show triterpene-glycoside affinity for dopamine D2 receptors. The D2 effect may explain the observation that Black Cohosh occasionally lowers prolactin in women with mild hyperprolactinemia, and may contribute to mood and vasomotor effects via the tubero-infundibular pathway.
- Opioid-receptor engagement — in 2008, a German group (Reame et al.) demonstrated mu-opioid receptor binding by Black Cohosh extract fractions. Opioid signaling in the hypothalamus modulates the LH/FSH pulse generator and is implicated in hot-flash generation through the KNDy (kisspeptin/neurokinin B/dynorphin) neuron system that has emerged as the central thermoregulatory player in menopause.
- Bone-protective effects — actein and related triterpenes appear to stimulate osteoblast activity and suppress osteoclast differentiation in vitro and in ovariectomized rat models. The mechanism is independent of estrogen receptors and may involve RANKL/OPG modulation. The clinical magnitude is smaller than estradiol but measurable. See the Bone Health deep-dive.
The controversy — and there is genuine controversy — arises from two facts. First, the older literature (pre-2002) is full of papers describing Black Cohosh as estrogenic, and these claims are repeated uncritically in textbooks and consumer-facing materials decades after they have been overturned by careful receptor-binding and microarray studies. The Wuttke group's 2003 demonstration that Black Cohosh extract did not bind ER-alpha or ER-beta in radioligand-binding assays, did not stimulate estrogen-response-element-luciferase reporter constructs, did not stimulate MCF-7 breast-cancer cell proliferation, and did not produce uterotrophic effects in ovariectomized rats was definitive. The Borrelli 2008 Cochrane review and the 2018 NAMS position statement both classify Black Cohosh as non-estrogenic. Second, the clinical-trial evidence for symptom relief is genuinely mixed — some large trials (HALT, Newton 2006) showed no benefit over placebo, while others (Wuttke 2003, Wuttke 2006, Frei-Kleiner 2005) showed clinically meaningful improvements. The plausible explanation is extract heterogeneity — the iso-propanolic extract Remifemin BNO 1055 (used in most positive trials) is not pharmaceutically equivalent to the various ethanolic, methanolic, and CO2 extracts marketed in North America. See the Menopause & Hot Flashes deep-dive for the trial-by-trial breakdown.
CRITICAL Hepatotoxicity Warning
REGULATORY WARNING: The U.S. Food and Drug Administration, the European Medicines Agency (EMA), and the Australian Therapeutic Goods Administration have all issued warnings since 2006 about rare cases of idiosyncratic liver injury associated with Black Cohosh use. EMA-required labeling on all Black Cohosh products in the European Union states: "Black cohosh may cause liver damage. Take medical advice if signs and symptoms suggestive of liver injury (tiredness, loss of appetite, yellowing of the skin and eyes or severe upper stomach pain with nausea and vomiting or dark urine) develop. Stop taking Black cohosh immediately and consult a doctor."
The hepatotoxicity question has been studied extensively in the two decades since the first case reports emerged. Several points are well-established:
- The events are real but very rare. The Naser 2011 systematic review (United States Pharmacopeia review committee) catalogued 83 published case reports of suspected Black Cohosh hepatotoxicity globally between 2002 and 2010, against an estimated population exposure of tens of millions of women-years of use. The Teschke 2011 expert RUCAM (Roussel Uclaf Causality Assessment Method) analysis of those cases found that only a minority met the threshold for "probable" causation; many had confounders (concomitant hepatotoxic drugs, pre-existing liver disease, contaminated or adulterated product).
- The mechanism is idiosyncratic, not dose-related. Unlike acetaminophen hepatotoxicity, the Black Cohosh signal does not correlate with dose or duration. This is the hallmark of an idiosyncratic immune-mediated drug-induced liver injury (DILI), typically involving a genetic-susceptibility component. The estimated incidence is on the order of one to a few per million users per year — rare in absolute terms, comparable to the idiosyncratic DILI rate for many prescription drugs that remain on the market.
- Product quality matters. A significant fraction of "Black Cohosh" products marketed in North America have been shown by HPLC and DNA-barcoding analysis to be adulterated with related but distinct Asian Cimicifuga species (C. dahurica, C. foetida, C. heracleifolia) which have different triterpene profiles and may carry different hepatotoxicity risk. Authenticated Actaea racemosa from the standardized iso-propanolic Remifemin extract has the longest safety record.
Practical safety protocol:
- Baseline LFTs before starting if the patient has any prior history of hepatic disease, current alcohol use, statin use, or other potentially hepatotoxic medications.
- Repeat LFTs at 6 months and every 6–12 months thereafter for any user continuing beyond 6 months. The 6-month checkpoint is recommended by the German Commission E monograph and adopted by most quality clinicians.
- Absolutely contraindicated in pre-existing liver disease — hepatitis B or C, autoimmune hepatitis, non-alcoholic steatohepatitis (NASH), alcoholic liver disease, primary biliary cholangitis, cirrhosis of any etiology. The risk-benefit calculation does not favor use.
- Avoid concomitant hepatotoxic drugs — high-dose acetaminophen, methotrexate, isoniazid, ketoconazole, kava kava.
- Discontinue immediately at the first sign of dark urine, jaundice, right-upper-quadrant pain, unusual fatigue, anorexia, or nausea. Get LFTs the same day.
- Use authenticated standardized product — the Remifemin iso-propanolic extract has been the most-studied and has the cleanest safety record. Avoid no-name bulk-powder products and any product whose label does not specify Actaea racemosa from North American sourcing.
The bottom line: the hepatotoxicity risk is real but small, the regulatory warnings are appropriate, and informed patients with normal baseline liver function can use Black Cohosh safely with periodic monitoring. The media coverage in 2006–2010 substantially overstated the population risk — estimates from that era suggested the per-user risk is comparable to or lower than the hepatotoxicity risk from common prescription medications that are not subject to the same warnings.
Key Research Papers
- Wuttke W, Seidlová-Wuttke D, Gorkow C (2003). The Cimicifuga preparation BNO 1055 vs. conjugated estrogens in a double-blind placebo-controlled study: effects on menopause symptoms and bone markers. Maturitas 44 Suppl 1:S67-77. — PubMed: Wuttke 2003 BNO 1055
- Burdette JE, Liu J, Chen SN et al. (2003). Black cohosh acts as a mixed competitive ligand and partial agonist of the serotonin receptor. Journal of Agricultural and Food Chemistry 51(19):5661-70. — PubMed: Burdette 2003 serotonin receptor
- Liske E, Hanggi W, Henneicke-von Zepelin HH et al. (2002). Physiological investigation of a unique extract of black cohosh (Cimicifugae racemosae rhizoma): a 6-month clinical study demonstrates no systemic estrogenic effect. Journal of Women's Health and Gender-Based Medicine 11(2):163-74. — PubMed: Liske 2002 anxiety subscale
- Leach MJ, Moore V (2012). Black cohosh (Cimicifuga spp.) for menopausal symptoms. Cochrane Database of Systematic Reviews 9:CD007244. — PubMed: Cochrane 2012
- Naser B, Schnitker J, Minkin MJ et al. (2011). Suspected black cohosh hepatotoxicity: no evidence by meta-analysis of randomized controlled clinical trials for isopropanolic black cohosh extract. Menopause 18(4):366-75. — PubMed: Naser 2011 hepatotoxicity meta-analysis
External Authoritative Resources
- NIH National Center for Complementary and Integrative Health — Black Cohosh — the U.S. government's primary patient-facing summary; covers efficacy, safety, and the hepatotoxicity warnings
- NIH Office of Dietary Supplements — Black Cohosh Fact Sheet (Health Professionals) — comprehensive scientific summary with full reference list
- European Medicines Agency — Cimicifugae racemosae rhizoma (Black Cohosh) — the EMA herbal monograph including the mandatory hepatotoxicity labeling
- North American Menopause Society (NAMS) — position statements on non-hormonal menopausal therapies including Black Cohosh
- MedlinePlus — Black Cohosh
- PubMed — All research on Black Cohosh / Actaea racemosa (~1,500+ papers)
Connections
- Black Cohosh (Main Page)
- Black Cohosh for Menopause & Hot Flashes
- Black Cohosh for Hormonal Balance
- Black Cohosh for Bone Health
- Black Cohosh for Mood & Sleep
- All Herbs
- Maca
- Ashwagandha
- Chamomile
- Lemon Balm
- Perimenopause
- Perimenopause Symptom Tracker
- Polycystic Ovary Syndrome
- Anxiety
- Depression
- Hormone Panel
- Stress Management