Astragalus for Cardiovascular Health
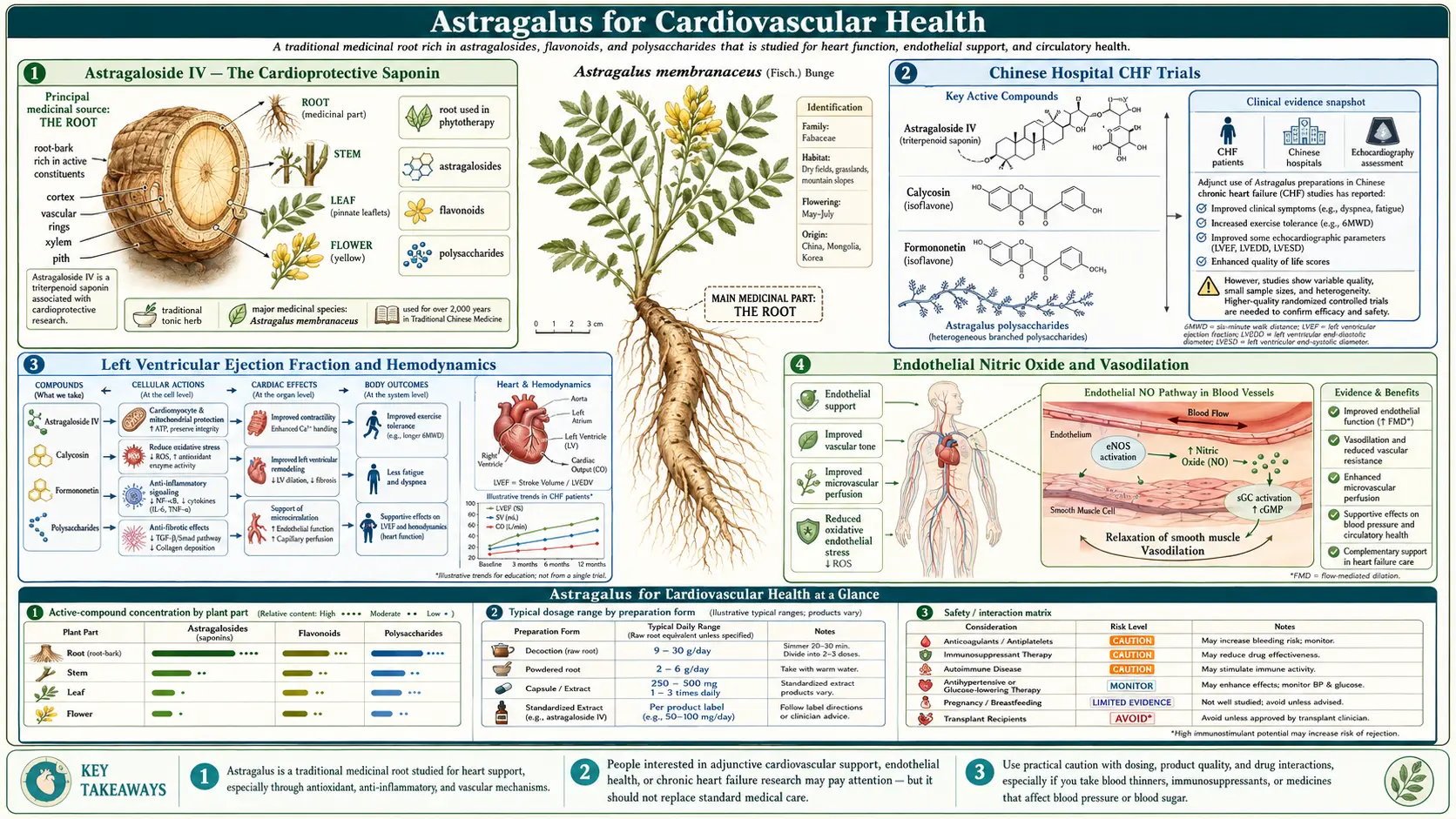
Astragaloside IV, the most thoroughly characterized triterpenoid saponin in Astragalus membranaceus, has produced one of the most coherent cardioprotective data packages of any single botanical compound. In Chinese hospital settings, intravenous astragalus injection added to standard congestive heart failure therapy improves left ventricular ejection fraction and exercise tolerance; oral preparations support endothelial nitric oxide production, reduce cardiac fibrosis after myocardial infarction, modulate cAMP signaling for a gentle positive inotropic effect, and protect vascular endothelium from oxidative damage. The pattern is consistent with the classical Chinese characterization of huang qi as a qi-tonifying herb for chronic deficiency — gradual restoration of cardiac function over weeks rather than acute hemodynamic intervention. This deep-dive traces the mechanism through endothelial biology, cardiomyocyte calcium handling, post-MI remodeling biology, and the integrative cardiology rationale for combining astragalus with optimal medical therapy in heart failure and ischemic heart disease.
Table of Contents
- Astragaloside IV — The Cardioprotective Saponin
- Chinese Hospital CHF Trials
- Left Ventricular Ejection Fraction and Hemodynamics
- Endothelial Nitric Oxide and Vasodilation
- cAMP Signaling and Positive Inotropic Effect
- Post-Myocardial Infarction Remodeling
- Ischemia-Reperfusion Injury Protection
- LDL Oxidation and Atherosclerosis
- Antiplatelet Activity and Thrombosis Prevention
- Anthracycline Cardiotoxicity Mitigation
- Integrative Cardiology — Adding Astragalus to Standard Therapy
- Dosing for Cardiovascular Indications
- Cautions (Anticoagulants, Hypotension, Surgery)
- Key Research Papers
- Connections
- Featured Videos
Astragaloside IV — The Cardioprotective Saponin
Astragaloside IV (AS-IV) is the most abundant and most thoroughly studied of the triterpenoid saponins in Astragalus membranaceus root. Chemically it is a cycloartane-type tetracyclic triterpene glycoside — an aglycone (cycloastragenol) attached to two sugar units (xylose and glucose). Standardized astragalus extracts for cardiovascular indications are commonly assayed for AS-IV content, typically 0.3 to 1.0% by weight of the dried root extract.
AS-IV is sufficiently lipid-soluble to cross cell membranes (the aglycone portion enters the lipid bilayer) and engage intracellular signaling targets. The pharmacological profile spans:
- Inhibition of TGF-beta-driven fibroblast-to-myofibroblast transition (the cellular basis of cardiac fibrosis)
- Modulation of PI3K/Akt and AMPK signaling, both relevant to cardiomyocyte survival under stress
- Upregulation of endothelial nitric oxide synthase (eNOS) and increased nitric oxide bioavailability
- Reduction of mitochondrial dysfunction and apoptosis under ischemia-reperfusion conditions
- Mild positive inotropic effect via cAMP-dependent calcium handling enhancement
- Direct antioxidant activity and upregulation of endogenous antioxidant enzyme expression (SOD, catalase, glutathione peroxidase)
The same molecular mechanisms that make AS-IV cardioprotective also drive its renoprotective effects, discussed in the Kidney and Diabetic Nephropathy deep-dive — TGF-beta inhibition reduces fibrosis equally in cardiac and renal tissue, eNOS upregulation improves microcirculation in both vascular beds, and the antioxidant effects translate across organ systems. This is one of the reasons astragalus is well-suited to patients with combined cardiorenal disease, where the two organ systems are simultaneously failing.
Chinese Hospital CHF Trials
The clinical evidence base for astragalus in congestive heart failure (CHF) is largely Chinese in origin. Multiple randomized controlled trials have been conducted in Chinese university hospital cardiology departments, generally adding astragalus — most often as an injectable preparation (huang qi zhu she ye) administered intravenously alongside standard therapy — to a control arm receiving standard therapy alone.
A representative meta-analysis pooled 62 randomized trials (more than 5,000 patients) evaluating astragalus injection added to standard CHF therapy (ACE inhibitor or ARB, beta-blocker, diuretic, digoxin where indicated). The pooled effect:
- Improvement in left ventricular ejection fraction (LVEF) by approximately 5-10 percentage points beyond standard therapy
- Reduction in N-terminal pro-B-type natriuretic peptide (NT-proBNP) levels
- Improvement in NYHA functional class
- Improvement in 6-minute walk distance
- Reduction in re-hospitalization rates for decompensated CHF
- Quality-of-life score improvements on Minnesota Living with Heart Failure Questionnaire
The methodological quality of individual trials varies substantially — many trials are single-center, open-label or single-blind, with relatively short follow-up — and the reliance on injectable astragalus rather than oral preparations limits direct translation to outpatient Western practice. Major Western cardiology guidelines do not yet incorporate astragalus, and rigorous multi-center placebo-controlled trials are needed before formal incorporation. However, the consistency of the directional effect across many trials and the mechanistic plausibility justify cautious clinical interest, particularly for patients seeking adjunctive options to optimize their standard regimen.
Left Ventricular Ejection Fraction and Hemodynamics
Left ventricular ejection fraction (LVEF) is the fraction of blood pumped from the left ventricle with each contraction. Normal LVEF is 55-70%; reduced LVEF (typically defined as <40%) is the diagnostic threshold for "heart failure with reduced ejection fraction" (HFrEF), the systolic heart failure pattern that benefits from neurohormonal blockade with ACE inhibitors, beta-blockers, mineralocorticoid receptor antagonists, and SGLT2 inhibitors.
The astragalus effect on LVEF appears to operate through three mechanisms:
- Direct positive inotropic effect — astragaloside IV mildly enhances cardiomyocyte calcium handling and contractility through cAMP-dependent and calcium-channel modulating mechanisms (discussed below)
- Afterload reduction via endothelial nitric oxide enhancement — improved peripheral vasodilation reduces the resistance the failing left ventricle must pump against, increasing ejection fraction at the same level of myocardial contractility
- Reverse remodeling effect — chronic astragalus use reduces TGF-beta-driven cardiac fibrosis and may allow gradual recovery of viable but stunned or hibernating myocardium
The combination of inotropic support, afterload reduction, and reverse remodeling closely parallels the effect profile of the optimal medical therapy regimen for HFrEF — which is why astragalus produces an additive rather than overlapping effect when added to standard therapy. The clinical implication is that astragalus is best understood as a complement to, not a replacement for, evidence-based guideline-directed medical therapy.
Endothelial Nitric Oxide and Vasodilation
The vascular endothelium — the single layer of cells lining all blood vessels — produces nitric oxide (NO) via the enzyme endothelial nitric oxide synthase (eNOS). Endothelium-derived NO diffuses to adjacent vascular smooth muscle, triggering relaxation, vasodilation, and reduced peripheral vascular resistance. Endothelial dysfunction — impaired NO production due to age, hypertension, diabetes, dyslipidemia, smoking, or chronic inflammation — is among the earliest detectable abnormalities in cardiovascular disease and a major contributor to hypertension, ischemic disease, and heart failure with preserved ejection fraction.
Astragaloside IV restores endothelial function through several pathways:
- Direct upregulation of eNOS gene expression and protein abundance in endothelial cells
- Increased eNOS enzymatic activity through PI3K/Akt-mediated phosphorylation of the eNOS Ser1177 activation site
- Reduction of inducible NOS (iNOS) overactivity in chronic inflammation (which produces pathological NO levels that scavenge oxygen)
- Antioxidant effects that preserve NO bioavailability by reducing the reaction of NO with superoxide to form peroxynitrite
- Reduced endothelial cell apoptosis under oxidative stress
The clinical translation is improved flow-mediated dilation (a standard non-invasive measure of endothelial function), reduced peripheral vascular resistance, modest blood pressure lowering (typically 5-10 mmHg systolic in mildly hypertensive patients), and improved exercise tolerance in patients with both stable angina and heart failure. The blood-pressure-lowering effect is generally too mild to substitute for first-line antihypertensives but additive when combined with them.
cAMP Signaling and Positive Inotropic Effect
The classical positive inotropic pharmacology (drugs that enhance cardiac contractility) operates primarily through one of two mechanisms: beta-adrenergic agonism (epinephrine, dobutamine) that activates G-protein coupled receptors and increases intracellular cAMP, or phosphodiesterase-3 inhibition (milrinone, inamrinone) that prevents cAMP degradation. Either way, the downstream effect is increased cAMP, which activates protein kinase A, which phosphorylates and enhances the activity of voltage-gated calcium channels and the sarcoplasmic reticulum calcium handling machinery.
Astragaloside IV exerts a mild positive inotropic effect through a similar cAMP-related mechanism, though with a more modest magnitude and a much more favorable safety profile than dobutamine or milrinone. The conventional pharmaceutical inotropes increase cardiac contractility powerfully but at the cost of increased oxygen consumption, arrhythmogenicity, and worse long-term mortality (the classical PROMISE and OPTIME-CHF trials showed long-term harm from chronic milrinone in advanced heart failure). Astragalus appears to provide modest inotropic support without these adverse long-term consequences — though the evidence base for very long-term outcomes is less mature than the evidence base for established Western inotropes.
The complementary effect to inotropy is the reverse-remodeling effect described above: while the cAMP-mediated boost provides modest immediate contractility enhancement, the TGF-beta antifibrotic effect and the eNOS-mediated afterload reduction produce slower, more durable structural improvement that persists after each individual dose. The net long-term clinical pattern is gradual improvement in cardiac function over weeks to months of consistent use, rather than the immediate but short-lived hemodynamic boost of acute inotropic infusion.
Post-Myocardial Infarction Remodeling
After acute myocardial infarction, the injured myocardium undergoes a process called "ventricular remodeling" — the chamber dilates, the wall thins, scar tissue replaces dead cardiomyocytes, and the remaining viable myocardium hypertrophies to compensate. Adverse remodeling progresses over months to years and is a major mechanism of post-MI heart failure. Pharmacologic reverse-remodeling (with ACE inhibitors, ARBs, mineralocorticoid receptor antagonists, and beta-blockers) is the central goal of standard post-MI care.
Astragaloside IV has been studied in animal MI models and in clinical trials as an adjunct to standard post-MI care:
- In rat coronary ligation models, AS-IV reduces infarct expansion, improves post-MI LVEF, and reduces fibrosis in remote (non-infarcted) myocardium
- The TGF-beta inhibition mechanism is particularly relevant — TGF-beta-driven myofibroblast transformation is the primary cellular driver of post-MI fibrosis
- Animal studies show reduced matrix metalloproteinase activity, suggesting reduced infarct-zone expansion
- Clinical trials adding astragalus to standard post-MI therapy show modest improvements in LVEF and reductions in NT-proBNP at 3-6 month follow-up
The translation to clinical practice is that astragalus may serve as an adjunctive therapy in the post-MI recovery period — alongside, not instead of, the guideline-directed combination of ACE-inhibitor/ARB, beta-blocker, statin, and antiplatelet therapy. For more on the broader cardiovascular context, see our Cardiovascular Disease page.
Ischemia-Reperfusion Injury Protection
Ischemia-reperfusion (I-R) injury is the paradoxical cellular damage that occurs when blood flow is restored to ischemic tissue. The reperfusion itself — through generation of reactive oxygen species, intracellular calcium overload, mitochondrial dysfunction, and inflammatory cell infiltration — can produce a substantial fraction of the final tissue damage. In clinical practice this matters for primary PCI after acute MI, for cardiac surgery requiring cardiopulmonary bypass, and for stroke management with thrombolysis or thrombectomy.
Astragaloside IV has been one of the more thoroughly studied botanical cardioprotectants against I-R injury. In rodent and isolated-heart models:
- Pretreatment with AS-IV before coronary occlusion reduces infarct size by 20-40%
- Treatment given at the time of reperfusion (clinically more relevant) also reduces infarct size, suggesting protection against the reperfusion phase specifically
- Mitochondrial integrity is preserved — reduced opening of the mitochondrial permeability transition pore, the proximate trigger of cardiomyocyte death
- Endogenous antioxidant defenses (SOD, catalase, glutathione) are upregulated
- Apoptosis markers (caspase-3 activation, Bax/Bcl-2 ratio) are favorably shifted
The clinical translation to humans is preliminary — a small number of trials have given oral or IV astragalus to patients undergoing elective PCI or cardiac surgery and shown reduced post-procedure troponin elevation, suggesting reduced myocardial injury. The evidence is not yet sufficient to justify routine integration into peri-procedural protocols, but the mechanistic case is strong enough that this is an active area of research interest.
LDL Oxidation and Atherosclerosis
Atherosclerosis — the inflammatory accumulation of cholesterol-rich plaque in arterial walls — is initiated and propagated in large part by oxidized LDL particles. Native LDL is poorly atherogenic; oxidized LDL is highly atherogenic, taken up by macrophage scavenger receptors to form lipid-laden foam cells, the cellular foundation of atherosclerotic plaque. Reducing LDL oxidation is one of the mechanisms by which antioxidant interventions theoretically slow atherogenesis.
Astragalus has been studied in animal atherosclerosis models (particularly the apolipoprotein-E knockout mouse and the cholesterol-fed rabbit) with consistent findings of:
- Reduced oxidized LDL formation in plasma
- Reduced atherosclerotic plaque area in aortic specimens
- Reduced macrophage infiltration in plaque lesions
- Reduced inflammatory cytokine expression in plaque (TNF-alpha, IL-6, monocyte chemoattractant protein-1)
- Modest improvements in lipid profile (small reductions in total cholesterol and LDL, small increases in HDL)
The lipid effects are too small to substitute for statin therapy or other proven lipid-lowering interventions, but the antioxidant and anti-inflammatory effects on the vascular wall may complement statin therapy by addressing components of atherogenesis that lipid lowering alone does not fully control. The relationship is similar to the role of Vitamin E and other dietary antioxidants in cardiovascular prevention — supplementary, not primary.
Antiplatelet Activity and Thrombosis Prevention
Astragalus exerts mild antiplatelet activity, inhibiting both ADP-induced and collagen-induced platelet aggregation in laboratory assays. The mechanism appears to involve modulation of cyclooxygenase pathways, calcium signaling within platelets, and increased endothelial prostacyclin production that counters platelet activation.
The clinical significance of this antiplatelet effect cuts both ways:
- Potential benefit — modest reduction in pathologic thrombosis risk, complementary to the platelet effects of omega-3 fatty acids, garlic, ginkgo, and other dietary antiplatelet interventions
- Potential risk — additive bleeding risk when combined with antiplatelet medications (aspirin, clopidogrel, ticagrelor) or anticoagulants (warfarin, rivaroxaban, apixaban, dabigatran)
- Surgical context — astragalus should be discontinued at least 2 weeks before scheduled surgery to minimize peri-operative bleeding risk
For patients on combined antiplatelet and anticoagulant therapy (dual antiplatelet therapy for recent stent placement, anticoagulant plus aspirin for atrial fibrillation plus coronary disease), the additive bleeding risk should be discussed with the cardiologist and hematologist before adding astragalus. The mild magnitude of astragalus's antiplatelet effect means the absolute bleeding risk increase is small, but in high-bleeding-risk patients the combination requires careful review.
Anthracycline Cardiotoxicity Mitigation
Anthracycline chemotherapy (doxorubicin, epirubicin, daunorubicin, idarubicin) is one of the most effective classes of cancer chemotherapy — central to the management of breast cancer, lymphoma, leukemia, and sarcoma — but it is dose-limited by cumulative cardiotoxicity. The dose-response is essentially linear with cumulative dose, with approximately 5% of patients developing clinical heart failure at 400 mg/m² doxorubicin equivalent and approximately 26% at 550 mg/m². The mechanism is thought to involve oxidative stress from iron-anthracycline complexes, mitochondrial dysfunction, and direct DNA damage in cardiomyocytes.
Astragaloside IV has been studied as a cardioprotectant during anthracycline chemotherapy, with animal studies showing:
- Reduced doxorubicin-induced cardiomyocyte apoptosis
- Preserved cardiac function on echocardiogram after equivalent cumulative doxorubicin doses
- Reduced cardiac troponin elevation during treatment cycles
- Preserved mitochondrial function in cardiac tissue
- Reduced lipid peroxidation in cardiac tissue
Small clinical trials in patients receiving anthracycline-containing regimens for breast cancer and lymphoma have shown reduced subclinical cardiac injury markers (NT-proBNP, troponin) and preserved LVEF on serial echocardiography. The evidence is not yet sufficient to recommend astragalus as a routine cardioprotective adjunct on the same evidence basis as dexrazoxane (the FDA-approved pharmaceutical cardioprotectant), but the mechanistic case is strong and the safety profile is favorable. For patients receiving anthracyclines who are particularly anxious about cardiotoxicity (those with pre-existing reduced LVEF, very high planned cumulative dose, or prior chest radiation), this is reasonable to discuss with the treating oncologist.
Integrative Cardiology — Adding Astragalus to Standard Therapy
The integrative cardiology rationale for adding astragalus to a standard cardiology regimen rests on several considerations:
- Mechanistic complementarity — the effects of astragalus (endothelial NO enhancement, mild inotropy, antifibrotic, antioxidant) complement rather than overlap with the effects of standard pharmaceuticals (RAAS inhibition, beta-blockade, mineralocorticoid receptor antagonism, SGLT2 inhibition)
- Safety profile — favorable, with no major end-organ toxicity at recommended doses, well-characterized drug interaction profile
- Patient-experienced benefits — many patients report improved exercise tolerance and energy on astragalus, which may improve adherence to the broader cardiac-rehabilitation regimen
- Cardiorenal patients — particularly attractive in patients with combined heart failure and chronic kidney disease, where both organ systems benefit from the same molecular mechanism
The caveats are equally important. Astragalus is an adjunct, not a substitute, for evidence-based guideline-directed therapy. Patients should never discontinue or reduce their standard cardiac regimen to substitute astragalus or any other herbal therapy. Cardiology follow-up should continue on the standard schedule, with monitoring of NT-proBNP, LVEF on serial echocardiograms, and functional status. Astragalus should be added under the awareness of the treating cardiologist, particularly for the antiplatelet interaction discussed above.
Dosing for Cardiovascular Indications
- Standardized capsule extract (cardiovascular indication) — 250-500 mg of an extract standardized to 0.3-1.0% astragaloside IV, two to three times daily with meals. AS-IV-standardized products are preferred over APS-standardized products for cardiovascular indications.
- Sliced root decoction — 15-30 g of dried root simmered in water for 20-30 minutes daily; appropriate for patients who prefer traditional preparations
- Tincture (1:3) — 3-5 mL three times daily
- Astragalus injection (huang qi zhu she ye) — the form used in Chinese hospital CHF trials, administered IV by qualified TCM-trained physicians, not available in the United States outside research settings
- Course duration — cardiovascular effects build slowly over 8-12 weeks; the patient and clinician should plan a minimum 12-week trial before assessing response
- Monitoring — LVEF, NT-proBNP, functional class, 6-minute walk distance at baseline and at 12 weeks; blood pressure and heart rate at standard cardiology visits; INR if combined with warfarin
Cautions (Anticoagulants, Hypotension, Surgery)
- Anticoagulant interaction — the antiplatelet activity discussed above can add to the bleeding risk of warfarin, DOACs (rivaroxaban, apixaban, edoxaban, dabigatran), aspirin, clopidogrel, ticagrelor, prasugrel. Discuss with cardiologist before combining; consider INR monitoring with warfarin combinations.
- Hypotension — the endothelial NO-mediated vasodilation can produce additive hypotension in patients on multiple antihypertensives. Watch for orthostasis, particularly in elderly patients and those on alpha-blockers, ACE inhibitors, ARBs, or calcium-channel blockers.
- Pre-surgical period — discontinue astragalus at least 2 weeks before scheduled surgery (cardiac or otherwise) to minimize bleeding risk and avoid unclear interactions with anesthesia.
- Severe aortic stenosis — theoretical concern about vasodilation in a patient with fixed cardiac output; discuss with cardiologist before use.
- Lithium therapy — astragalus has mild diuretic effects and could affect lithium clearance; monitor lithium levels if combining.
- Pregnancy and breastfeeding — insufficient safety data; avoid in the absence of specific clinical guidance.
- Heart transplant recipients — astragalus is contraindicated due to immunosuppression interaction risk and potential rejection.
- Combined with checkpoint-inhibitor immunotherapy — if astragalus is used for cardiac protection during anthracycline therapy in a cancer patient also receiving checkpoint inhibitors, discuss with the oncology team because of the theoretical immune-stimulation interaction with the immunotherapy.
Key Research Papers
- Ren S et al. (2013). Pharmacological effects of astragaloside IV: a literature review. Journal of Traditional Chinese Medicine. — PubMed
- Zhang WD et al. (2006). Astragaloside IV from Astragalus membranaceus shows cardioprotection during myocardial ischemia in vivo and in vitro. Planta Medica. — PubMed
- Fu S et al. (2014). Astragalus polysaccharide injection added to conventional treatment for chronic heart failure: meta-analysis of randomized controlled trials. Evidence-Based Complementary and Alternative Medicine. — PubMed
- Liu T et al. (2017). Astragaloside IV alleviates heart failure via activating PPAR-alpha to switch glycolysis to fatty acid beta-oxidation. Scientific Reports. — PubMed
- Wang D et al. (2009). Effect of Astragalus membranaceus on viral myocarditis: clinical and experimental study. Chinese Medical Journal. — PubMed
- Xu XL et al. (2007). Endothelium-dependent and -independent effects of astragaloside IV on isolated rat aorta. European Journal of Pharmacology. — PubMed
- Cheng XD et al. (2018). Astragaloside IV protects against ischemia reperfusion injury by activating Akt and reducing apoptosis: a meta-analysis of preclinical studies. Journal of Cellular Physiology. — PubMed
- Wei Y et al. (2018). Astragaloside IV and doxorubicin-induced cardiotoxicity. Phytotherapy Research. — PubMed
- Li M et al. (2017). Astragaloside IV improves diabetic cardiomyopathy by inhibiting myocardial autophagy via mTOR signaling. Frontiers in Pharmacology. — PubMed
- Zhang JG et al. (2007). Astragaloside IV derived from Astragalus membranaceus: a research review on the pharmaceutical effects. Advances in Pharmacological Sciences. — PubMed
- Gui J et al. (2013). Astragaloside IV improves heart function in chronic heart failure rats. American Journal of Translational Research. — PubMed
- Zhao M et al. (2008). Astragaloside IV attenuates cardiac dysfunction by suppressing NF-kappaB-driven inflammation in heart failure. Cardiovascular Drugs and Therapy. — PubMed
PubMed Topic Searches
- PubMed: AS-IV in heart failure
- PubMed: Endothelial NO
- PubMed: Ischemia-reperfusion protection
- PubMed: Anthracycline cardiotoxicity
- PubMed: LDL oxidation and atherosclerosis
Connections
- Astragalus Overview
- Astragalus Benefits Hub
- Astragalus for Immune Function
- Astragalus for Anti-Aging
- Astragalus for Kidney Disease
- Cardiovascular Disease
- Hawthorn
- Garlic
- Turmeric
- Omega-3 Fatty Acids
- Magnesium
- Potassium
- Vitamin K2
- Vitamin E
- Oxidative Stress
- Lipid Panel
- Blood Pressure
- Cancer (Anthracycline Context)
- All Herbs
- Heart Failure — the condition the Chinese astragalus-injection trials were built around.