Sardines — Vitamin D and B12
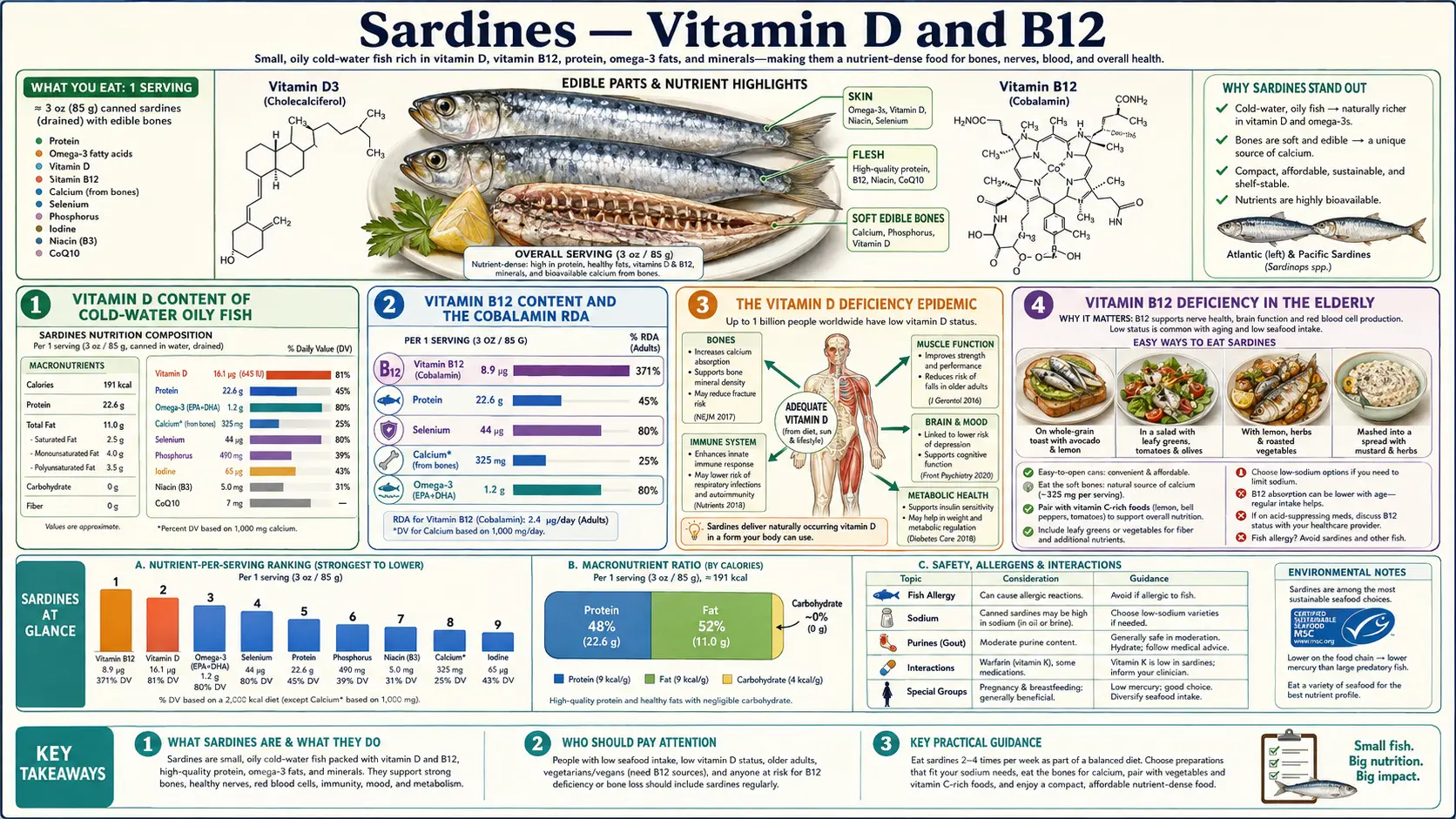
Vitamin D and Vitamin B12 are the two micronutrients most commonly inadequate in adult populations in the developed world. Roughly 25-40% of US adults have serum 25-hydroxyvitamin D below 20 ng/mL (frank insufficiency), and approximately 6% of adults under 60 and 20% of adults over 60 have biochemical Vitamin B12 deficiency — rising sharply with age, metformin use, proton-pump-inhibitor use, atrophic gastritis, and vegan diet. A single 3.75-ounce sardine tin provides roughly 175 IU Vitamin D3 (cholecalciferol) and 8.9 micrograms Vitamin B12 (cobalamin) — over 100% of the adult B12 RDA in one meal. Two to three tins per week is enough to address most cases of B12 marginal status and contribute meaningfully to Vitamin D adequacy alongside seasonal sun exposure and targeted supplementation. This page covers the populations at highest risk, the laboratory monitoring strategy, and why food-source D3 and B12 from sardines is particularly valuable for the elderly and for patients on chronic gastric-acid-suppression therapy.
Table of Contents
- Vitamin D Content of Cold-Water Oily Fish
- Vitamin B12 Content and the Cobalamin RDA
- The Vitamin D Deficiency Epidemic
- Vitamin B12 Deficiency in the Elderly
- Metformin and PPI as B12-Depleting Drugs
- Laboratory Monitoring (25-OH-D, MMA, Homocysteine)
- Supplement vs Food-Source Considerations
- The Vegan-to-Pescatarian Transition
- Cautions
- Key Research Papers
- Connections
- Featured Videos
Vitamin D Content of Cold-Water Oily Fish
Cold-water oily fish synthesize Vitamin D3 (cholecalciferol) in their tissues from 7-dehydrocholesterol precursors. The fish do not need UV-B exposure for this synthesis the way humans do — the conversion occurs in their liver and is concentrated in fatty tissues. The biological function appears to be calcium regulation analogous to human Vitamin D physiology.
USDA-listed Vitamin D content per 100 g for common fish:
- Wild salmon — 500-988 IU (the absolute leader; varies with species and season)
- Farmed salmon — 250-526 IU (lower due to feed composition; varies by producer)
- Mackerel — 360-643 IU
- Herring (kippered, pickled) — 200-450 IU
- Canned sardines (in oil) — 165-272 IU (varies by season and species)
- Canned tuna — 234 IU (albacore higher than skipjack)
- Cod — 36 IU (low; cod is a lean fish with most D in the liver, hence cod liver oil)
- Tilapia — 124 IU
- Cod liver oil (1 tsp) — 450-1,360 IU (and 2,500-5,000 IU Vitamin A, which is its own consideration)
A standard 3.75 oz sardine tin (106 g) provides approximately 175-285 IU Vitamin D3, depending on brand and season. This is 22-36% of the adult RDA (800 IU). Two tins per week averaged across the week is roughly 50-80 IU/day from sardines alone — meaningful but not sufficient as the sole strategy. For most US adults living north of 35°N latitude, fall and winter supplementation of 1,000-2,000 IU/day Vitamin D3 will still be needed to maintain serum 25-OH-D in the 30-50 ng/mL range. Sardines and salmon contribute the food-source baseline that reduces the supplementation requirement.
Vitamin B12 Content and the Cobalamin RDA
Vitamin B12 (cobalamin) is produced exclusively by bacteria. Animals acquire B12 either by consuming other animals (predators, carnivores), by consuming the bacteria themselves (ruminants harvesting B12 from fermentation in the rumen), or by consuming B12-rich animal tissues (organs, fish, eggs, dairy). Fish concentrate B12 in their liver, kidney, and muscle — sardines, being eaten whole with viscera in some preparations, are particularly B12 dense.
USDA-listed Vitamin B12 content per 100 g:
- Beef liver — 70 µg (the absolute leader, 2,900% RDA)
- Clams — 84 µg
- Oysters — 16-28 µg
- Wild salmon — 3.2 µg
- Canned sardines — 8.9 µg (370% RDA in one 100 g serving)
- Canned tuna — 2.5 µg
- Beef (chuck roast) — 5.8 µg
- Eggs (one large) — 0.45 µg
- Milk (1 cup) — 1.1 µg
- Cheddar cheese (1 oz) — 0.2 µg
- Plant foods (any) — 0 µg (the strict zero is the key distinguishing feature)
A single 3.75 oz sardine tin therefore provides roughly 9.4 µg of B12 — more than four times the adult RDA of 2.4 µg in one meal. The body absorbs roughly 50% of the B12 in food (limited by intrinsic factor binding capacity), so the absorbed amount per tin is approximately 4-5 µg, still more than double the daily requirement.
For frequent sardine consumers, B12 deficiency from dietary inadequacy is essentially impossible — the limiting factor becomes absorption capacity, not intake. This is clinically meaningful because the populations at highest B12 risk (elderly, atrophic gastritis, PPI/metformin users) suffer primarily from absorption failure rather than intake inadequacy, which is addressed in the next sections.
The Vitamin D Deficiency Epidemic
National Health and Nutrition Examination Survey (NHANES) data consistently show that 25-40% of US adults have serum 25-hydroxyvitamin D below 20 ng/mL (the IOM threshold for frank insufficiency), and 60-80% have levels below the 30 ng/mL threshold many endocrinologists consider optimal. The deficit is greater in:
- Black and Hispanic populations (skin melanin reduces cutaneous synthesis)
- Northern latitude residents (insufficient UV-B during winter months)
- Indoor workers and sunscreen users
- Adults over 65 (cutaneous 7-dehydrocholesterol concentration declines with age, halving synthesis capacity)
- Obesity (Vitamin D sequesters in adipose tissue, reducing serum availability)
- Malabsorption (celiac, Crohn's, cystic fibrosis, post-bariatric surgery)
- Chronic kidney disease (reduced 1-alpha-hydroxylase activity)
- Veiled populations (limited skin exposure to UV-B)
The clinical consequences of long-term Vitamin D insufficiency include impaired calcium absorption (leading to secondary hyperparathyroidism and bone resorption), increased fall and fracture risk, increased susceptibility to upper respiratory infections, and (in observational but not all randomized data) increased risk of cardiovascular events, autoimmune disease, and certain cancers.
The practical strategy for most adults is a three-pronged approach: dietary intake from oily fish (sardines, salmon, herring), seasonal sun exposure when possible (10-30 minutes midday spring/summer/fall on arms and legs without sunscreen), and targeted supplementation (1,000-2,000 IU/day Vitamin D3 for most adults; 4,000-5,000 IU/day for adults with documented severe deficiency, monitored by serum 25-OH-D every 3-6 months). Sardines contribute approximately 50-80 IU/day averaged across the week with 2-3 tins — not enough alone but a meaningful contribution to the food-source baseline.
For more on Vitamin D testing, dosing, and the optimal range debate, see our Vitamin D3 page.
Vitamin B12 Deficiency in the Elderly
B12 deficiency prevalence rises sharply with age. NHANES and Framingham Offspring Study data indicate:
- ~6% of adults under age 60 have serum B12 below 200 pg/mL (frank deficiency)
- ~20% of adults over 60 have serum B12 below 200 pg/mL
- ~40% of adults over 60 have biochemical evidence of B12 deficiency (elevated methylmalonic acid or homocysteine) even with apparently normal serum B12
The mechanism is not dietary inadequacy — elderly adults typically consume adequate dietary B12. The issue is absorption failure. B12 absorption requires:
- Adequate gastric acid to liberate B12 from food-protein binding
- Intrinsic factor produced by gastric parietal cells
- Intact ileum with cubilin-amnionless receptor complex for IF-B12 complex uptake
Atrophic gastritis (loss of parietal cells, common in the elderly) reduces both gastric acid and intrinsic factor. Pernicious anemia (autoimmune destruction of parietal cells) eliminates intrinsic factor entirely. Ileal resection (Crohn's surgery, bariatric surgery with intestinal bypass) eliminates the absorption site.
The clinical consequences of unrecognized B12 deficiency are serious and partially irreversible: peripheral neuropathy (paresthesia, loss of vibratory sense, gait instability), megaloblastic anemia, cognitive impairment ranging from subtle to frank dementia, and subacute combined degeneration of the spinal cord. The cognitive impairment in particular is often misdiagnosed as Alzheimer's disease in elderly patients — one of the most rewarding diagnoses to make because it is reversible with B12 repletion if caught early.
The 2024 American Geriatrics Society Beers Criteria and consensus expert opinion recommend screening serum B12 (and ideally methylmalonic acid) in all adults over 65, with the threshold for repletion set higher than the IOM laboratory cutoffs. The conservative threshold for considering B12 supplementation or sublingual B12 is serum B12 below 400 pg/mL or any elevation of MMA above 0.27 µmol/L.
Regular sardine consumption (2-3 tins per week) provides approximately 4-6 µg/day of B12 averaged across the week, which is well above the RDA but does not bypass the absorption problem for patients with severe atrophic gastritis or pernicious anemia. Those patients require sublingual B12 (1,000-2,000 µg/day), intranasal cyanocobalamin spray, or intramuscular methylcobalamin injections (1,000 µg monthly).
Metformin and PPI as B12-Depleting Drugs
Two extremely common medications reliably produce B12 depletion over time:
- Metformin — the first-line oral diabetes medication, taken by approximately 90 million Americans. Metformin interferes with calcium-dependent B12-intrinsic factor uptake in the ileum. Approximately 30% of patients on metformin for >5 years develop biochemical B12 deficiency; the FDA added a warning to the metformin label in 2017. Annual serum B12 monitoring is recommended for all metformin users; supplementation should be initiated when serum B12 falls below 400 pg/mL.
- Proton pump inhibitors (PPIs) — omeprazole, esomeprazole, pantoprazole, lansoprazole, dexlansoprazole, rabeprazole. PPIs suppress gastric acid production, reducing the gastric-acid-dependent release of B12 from food protein. Long-term use (>2 years) is associated with B12 deficiency in observational studies. The deficiency risk increases with both dose and duration.
Other B12-depleting medications include H2-blockers (ranitidine, famotidine, cimetidine — same mechanism as PPIs but less potent), colchicine, neomycin, chloramphenicol, and nitrous oxide (a one-time exposure during anesthesia can precipitate frank B12 deficiency in patients with marginal status).
For patients on metformin or chronic PPI therapy, dietary sardine consumption provides high-dose B12 in a form that may partially bypass the absorption block (the high concentration in a single meal saturates intrinsic factor capacity and allows some passive diffusion in the ileum). Three sardine tins per week (~9 µg/day averaged) plus 1,000 µg sublingual cyanocobalamin daily is a reasonable strategy for high-risk patients. Serum B12 and methylmalonic acid should be monitored annually.
Laboratory Monitoring (25-OH-D, MMA, Homocysteine)
The relevant blood tests for monitoring sardines-as-a-strategy for D and B12 adequacy:
- Serum 25-hydroxyvitamin D (25-OH-D) — the standard Vitamin D status test. Insurance coverage is variable but the cash price is $30-60. Target range debated:
- <20 ng/mL: frank deficiency (IOM)
- 20-30 ng/mL: insufficiency (Endocrine Society)
- 30-50 ng/mL: optimal (most expert consensus)
- 50-80 ng/mL: high-normal, well-tolerated
- >100 ng/mL: potential toxicity
- Serum Vitamin B12 (cobalamin) — the standard screening test, with substantial limitations:
- <200 pg/mL: frank deficiency
- 200-400 pg/mL: marginal status, suggesting MMA and homocysteine assessment
- >400 pg/mL: generally adequate
- The test does not distinguish between active methylcobalamin and inactive analogs; up to 30% of patients with biochemical deficiency have apparently normal serum B12
- Methylmalonic acid (MMA) — the most sensitive marker of functional B12 deficiency. B12 is required for the methylmalonyl-CoA mutase reaction; deficiency causes MMA accumulation. Elevation above 0.27 µmol/L (or 270 nmol/L) is suspicious; above 0.40 µmol/L is highly specific for B12 deficiency.
- Homocysteine — elevated in both B12 deficiency and folate deficiency. Useful as a secondary marker but not specific to B12.
- Holotranscobalamin (active B12) — the fraction of serum B12 bound to transcobalamin II that is bioavailable to tissues. Newer test, not widely available; may eventually replace serum B12 as the screening test.
For a patient instituting a sardine-based dietary strategy, the recommended baseline workup is 25-OH-D, serum B12, MMA, and homocysteine. Repeat at 3-6 months to document response. Adjust supplementation as needed.
Supplement vs Food-Source Considerations
For Vitamin D, food-source intake from sardines, salmon, and other oily fish is meaningful but typically insufficient alone for most adults living north of 35°N latitude. The realistic strategy combines food-source D3 (50-150 IU/day averaged) with seasonal sun exposure when possible and 1,000-2,000 IU/day supplemental D3 in fall/winter or year-round for indoor workers. Vitamin D3 (cholecalciferol) supplements are inexpensive ($5-10 for a year's supply), shelf-stable, and well-tolerated. There is no clear advantage of food-source over supplemental D3 from a biochemistry standpoint — both are converted to 25-OH-D in the liver and 1,25-(OH)2-D in the kidney through identical pathways.
For B12, the food-source vs supplement distinction is more nuanced. The intrinsic-factor-mediated absorption pathway has limited capacity (approximately 1.5-2 µg per meal). High-dose supplements (1,000-2,000 µg/day) saturate this pathway but also produce some passive diffusion across the intestinal wall (estimated 1% of the dose). For patients with intact GI function, dietary B12 from fish, meat, eggs, and dairy is more than adequate. For patients with absorption failure (atrophic gastritis, pernicious anemia, PPI/metformin users, post-bariatric), high-dose oral or sublingual supplementation is necessary, and dietary B12 alone is not sufficient.
The form of supplemental B12 matters. Cyanocobalamin is the cheapest and most stable form but requires conversion to methylcobalamin or adenosylcobalamin in the body. Methylcobalamin and adenosylcobalamin (or "methyl-B12") are the active coenzyme forms and bypass the conversion step. Hydroxocobalamin (used clinically as an antidote for cyanide poisoning) is also effective. For most patients, generic cyanocobalamin is fine; patients with MTHFR polymorphisms or those who prefer the active form can use methylcobalamin at modestly higher cost.
The Vegan-to-Pescatarian Transition
Long-term strict vegans (vegetable matter only, no dairy, eggs, or fish) reliably develop B12 deficiency if they do not supplement — usually within 3-5 years for adults, faster for children. The Adventist Health Study-2 documented 52% B12 deficiency among vegans who did not supplement, with significant elevations in homocysteine and MMA.
Many vegans choose to remain vegan and supplement reliably with fortified plant milks (B12-fortified), nutritional yeast (B12-fortified), and explicit B12 supplements. This strategy works when followed consistently; the failure mode is intermittent supplementation that allows depletion of liver B12 stores over years.
Some long-term vegans choose to transition to a "pescatarian" pattern — including fish (and often eggs and dairy) while continuing to avoid land animals. The motivations vary (resolving B12 or omega-3 deficiency, addressing low-energy or cognitive symptoms, ethical evolution). For these patients, sardines are an ideal entry point:
- The smallest, least sentient marine organism in the human food chain
- Sustainable harvest with minimal environmental impact
- The most ethical-acceptable option for many people transitioning from strict veganism
- The highest single-food density of the two micronutrients (D and B12) most likely to be depleted
- The lowest toxin and contaminant burden
- Calcium-replete (addressing the calcium gap if dairy is also being avoided)
- Omega-3-replete (addressing the EPA/DHA gap that ALA from flax and walnut does not adequately fill)
A typical transition protocol is to begin with 1 tin per week and assess tolerance, taste, and any psychological or ethical considerations, then escalate to 2-3 tins per week over 4-8 weeks. Lab monitoring of serum B12, MMA, and 25-OH-D before and 3-6 months after the transition will document the response. Most patients see normalization of MMA and meaningful elevation of 25-OH-D within 3 months.
Cautions
- Vitamin D toxicity — cannot occur from food-source D from sardines alone. Toxicity (serum 25-OH-D >100 ng/mL with hypercalcemia) requires sustained intake of approximately 50,000 IU/day or more — achievable only with high-dose supplementation, never with diet alone. Sardine consumption at any practical level is safe.
- Vitamin B12 toxicity — B12 has no established upper limit; the body excretes excess B12 in urine. The pink color of high-dose B12 supplement urine is harmless. Sardine consumption at any practical level is safe.
- Hidden Vitamin A in sardines — sardines do contain some Vitamin A (32 mcg RAE per tin), much less than beef liver or cod liver oil. Not a teratogenicity concern at any reasonable intake level.
- B12-folate masking — high folate intake (often from folic-acid-fortified grains) can correct the megaloblastic anemia of B12 deficiency while allowing the neurological damage to progress unrecognized. Patients should be screened with MMA or holotranscobalamin if there is any clinical suspicion of B12 deficiency, regardless of folate or hemoglobin status.
- Drug interactions with sardine fortification of B12 — none. Sardine B12 follows the same absorption pathway as any food-source B12.
- The Vitamin D supplementation controversy — the VITAL trial and other large RCTs have not shown clear cardiovascular or cancer prevention benefit from Vitamin D supplementation in already-replete adults. The benefit appears confined to patients with documented insufficiency. The argument for sardine consumption is not "as much as possible" — it is to maintain the food-source baseline alongside testing and targeted supplementation.
Key Research Papers
- Holick MF (2007). Vitamin D deficiency. NEJM. — PubMed
- Allen LH (2009). How common is vitamin B-12 deficiency? American Journal of Clinical Nutrition. — PubMed
- Stabler SP (2013). Vitamin B12 deficiency. NEJM. — PubMed
- de Jager J et al. (2010). Long term treatment with metformin in patients with type 2 diabetes and risk of vitamin B-12 deficiency: randomised placebo controlled trial. BMJ. — PubMed
- Lam JR et al. (2013). Proton pump inhibitor and histamine 2 receptor antagonist use and vitamin B12 deficiency. JAMA. — PubMed
- Manson JE et al. (2019). Vitamin D Supplements and Prevention of Cancer and Cardiovascular Disease (VITAL). NEJM. — PubMed
- Lips P (2007). Vitamin D physiology. Progress in Biophysics and Molecular Biology. — PubMed
- Pawlak R et al. (2013). How prevalent is vitamin B12 deficiency among vegetarians? Nutrition Reviews. — PubMed
- Wang H et al. (2013). Efficacy of vitamin B supplementation on cognition in elderly patients with cognitive-related diseases: meta-analysis. Journal of Geriatric Psychiatry and Neurology. — PubMed
- Carmel R (2011). Biomarkers of cobalamin (vitamin B-12) status in the epidemiologic setting. American Journal of Clinical Nutrition. — PubMed
- Smith AD et al. (2010). Homocysteine-lowering by B vitamins slows the rate of accelerated brain atrophy in mild cognitive impairment. PLoS ONE. — PubMed
- Pittas AG et al. (2019). Vitamin D Supplementation and Prevention of Type 2 Diabetes (D2d). NEJM. — PubMed
PubMed Topic Searches
- PubMed: Vitamin D in oily fish
- PubMed: B12 elderly / atrophic gastritis
- PubMed: Metformin / PPI B12 depletion
- PubMed: MMA functional B12
- PubMed: Vegan B12 / homocysteine
Connections
- Sardines Overview
- Sardines Benefits Hub
- Sardines — Calcium & Bones
- Sardines — Omega-3 Density
- Sardines — Low Mercury
- Vitamin D3
- Vitamin B12
- Folate (Vitamin B9)
- 25-Hydroxyvitamin D Test
- Vitamin B12 Test
- Methylmalonic Acid Test
- Homocysteine Test
- Anemia
- Peripheral Neuropathy
- Type 2 Diabetes (Metformin)
- GERD (PPI Use)