Sardines for Calcium & Bones from Whole Fish
Sardines are unique among commonly consumed animal foods because their soft, fully-edible vertebrae and ribs deliver hydroxyapatite calcium — the same biological mineral matrix as human bone — in a form the digestive tract recognizes and absorbs efficiently. A single 3.75-ounce tin provides 351 mg of calcium (27% of the adult RDA), more than a cup of milk, alongside the Vitamin D3, magnesium, phosphorus, and Vitamin K2 cofactors that determine whether dietary calcium ends up mineralizing bone or calcifying arteries. For postmenopausal women, men over 70, patients with lactose intolerance, and anyone who cannot tolerate dairy, sardines are arguably the most efficient single-food strategy for meeting calcium needs without the cardiovascular risk signal associated with high-dose isolated calcium carbonate supplements.
Table of Contents
- Why Edible Fish Bones Are an Exceptional Calcium Source
- Hydroxyapatite vs Calcium Carbonate Bioavailability
- The Calcium Cofactors Sardines Deliver Together
- Postmenopausal Bone Loss and Dietary Calcium
- A Dairy-Free Calcium Strategy
- The Calcium Supplement Cardiovascular Controversy
- The Sardinian Blue Zone Pattern
- Practical Intake — How Many Tins per Week
- Cautions (Kidney Stones, Hyperparathyroidism)
- Key Research Papers
- Connections
- Featured Videos
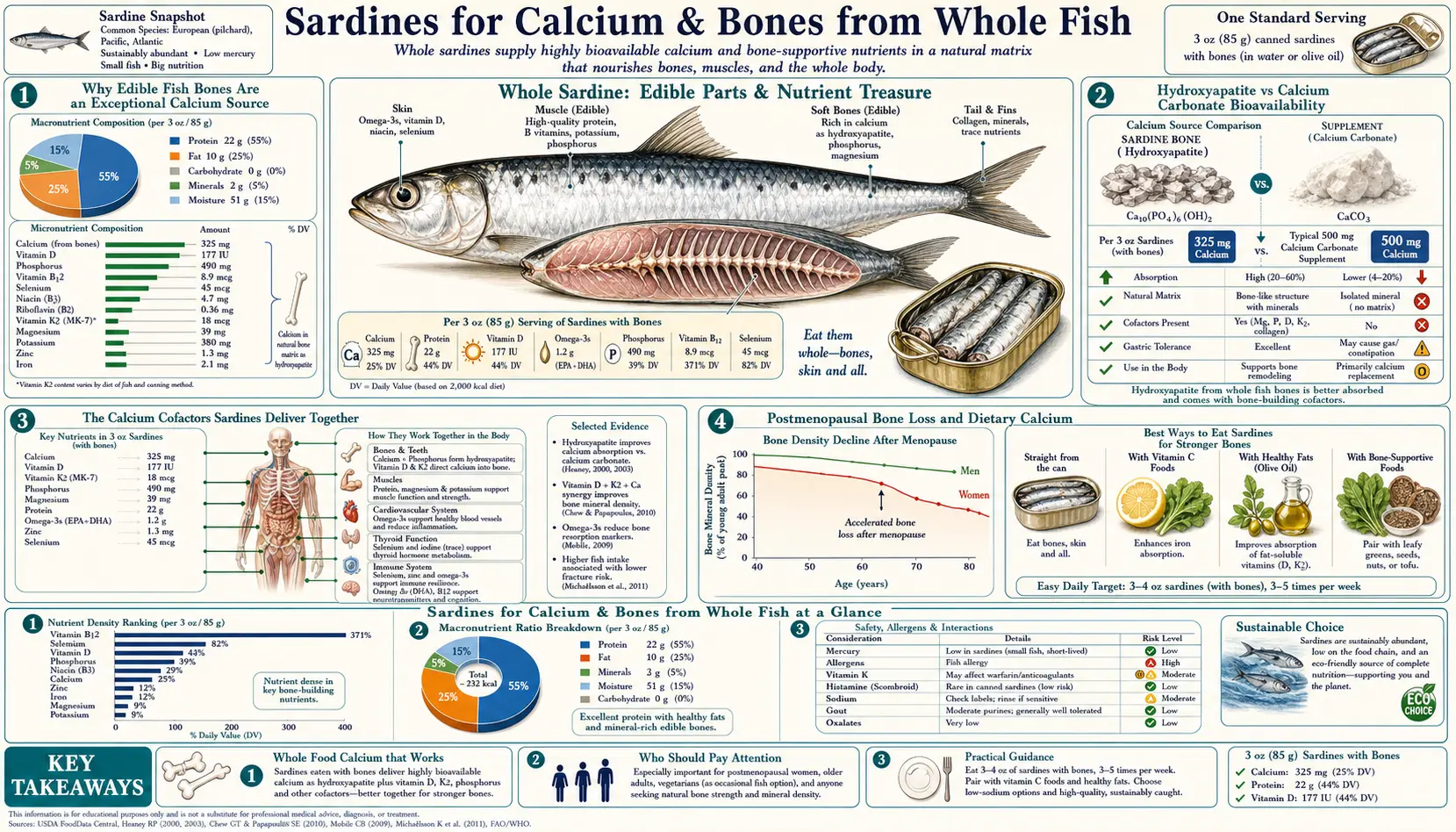
Why Edible Fish Bones Are an Exceptional Calcium Source
The canning process for sardines — typically pressure-cooked at 115-121 °C for 60-90 minutes in sealed cans — thoroughly softens the vertebrae and ribs of the fish to the point where they become indistinguishable in texture from the surrounding flesh. The bones do not need to be removed, and most consumers do not even notice them in the final product. What they are eating is biological hydroxyapatite — the same calcium-phosphate mineral lattice that constitutes their own skeleton.
Hydroxyapatite (chemical formula Ca10(PO4)6(OH)2) is the dominant inorganic component of vertebrate bone. It is laid down on a collagen scaffold during ossification, providing the compressive strength of bone while collagen provides the tensile strength. When sardine bone is dissolved in gastric acid, the released calcium and phosphate ions enter the duodenum together, in roughly the correct stoichiometric ratio for bone mineralization, alongside intact collagen-derived peptides and bone-matrix proteins.
This is different from drinking milk (where calcium is bound to casein protein), eating dark leafy greens (where calcium is partially bound to oxalate and fiber), or taking a calcium carbonate or citrate supplement (where calcium is isolated and chemically defined). Each form has different absorption characteristics, and each interacts with different cofactor requirements. The fish-bone form is the closest dietary match to the body's actual bone-mineral chemistry.
Hydroxyapatite vs Calcium Carbonate Bioavailability
Calcium carbonate (the most common over-the-counter calcium supplement, found in Tums, Caltrate, Os-Cal, and Citracal-D) requires significant gastric acid to dissolve. In healthy young adults with normal stomach acid, calcium carbonate absorption is roughly 25-30% when taken with food. In adults over 65 with reduced gastric acid (atrophic gastritis affects 25-30% of this population), or in patients on chronic proton pump inhibitor therapy (omeprazole, esomeprazole, pantoprazole, lansoprazole), calcium carbonate absorption can drop to 5-10% — meaning most of the calcium passes through unabsorbed.
Calcium citrate (the second common supplement form) does not require gastric acid for dissolution and maintains 30-35% absorption regardless of stomach acid status. It is the supplement of choice for elderly patients and those on acid-suppression therapy.
Hydroxyapatite calcium from edible fish bone is absorbed at approximately 25-30% in studies of human subjects, comparable to calcium carbonate in young adults and superior in elderly subjects because the fish bone matrix appears to release calcium more gradually as it is digested. The Malde et al. studies and related work suggest that fish-bone calcium does not have the absorption falloff at low stomach acid that supplemental calcium carbonate does.
More importantly, the calcium from sardines comes embedded in a complete bone-mineralization toolkit, which the next section addresses.
The Calcium Cofactors Sardines Deliver Together
Calcium absorption is only the first step. The body needs additional micronutrients to direct absorbed calcium to bone tissue rather than to arterial walls, kidney stones, or soft-tissue calcification. The four key cofactors are Vitamin D3 (calcium absorption and transport), magnesium (bone matrix formation), phosphorus (the other half of hydroxyapatite), and Vitamin K2 menaquinone (activates osteocalcin, which deposits calcium into bone, and activates matrix Gla protein, which removes calcium from arteries).
A single sardine tin delivers all four together:
- Vitamin D3 (cholecalciferol) — approximately 175 IU per tin, roughly 22% of the adult RDA
- Magnesium — 39 mg per tin, approximately 10% of adult RDA
- Phosphorus — 451 mg per tin, approximately 36% of adult RDA, in the correct biological ratio with the calcium
- Vitamin K2 menaquinone — small but non-zero amounts (K2 is produced by gut bacteria in the fish and concentrated in fatty tissues)
For Vitamin K2 specifically, fermented foods (natto, hard cheeses) and pasture-raised dairy and eggs are the dietary leaders, but oily fish does contribute. The combination of calcium, phosphorus, magnesium, and Vitamin D3 in sardines (alongside high-quality protein for the bone collagen matrix) is essentially a complete bone-formation package in a single shelf-stable food.
Contrast this with a calcium carbonate supplement: it provides calcium alone, with none of the cofactors. The 2006 Auckland Calcium Study and the 2010 Bolland et al. meta-analysis raised concerns that high-dose isolated calcium supplementation (1,000+ mg/day from supplements) was associated with increased risk of myocardial infarction — possibly because the calcium pulse without K2 activation of matrix Gla protein contributed to arterial calcification rather than bone deposition. This concern, addressed in detail below, does not apply to food-source calcium because food sources deliver the calcium with its cofactors.
Postmenopausal Bone Loss and Dietary Calcium
Postmenopausal women lose approximately 1-2% of bone mineral density per year for the first 5-10 years after menopause, driven by the loss of estrogen's protective effect on osteoclast activity. Over a lifetime, this translates to a hip fracture risk of approximately 17-20% for a 50-year-old white woman.
Adequate dietary calcium does not stop this loss but slows it. The IOM recommends 1,200 mg/day of calcium for women over 50 and men over 70. The average American adult consumes 800-1,000 mg/day, leaving a 200-400 mg gap that needs to be closed through food or supplementation.
Two sardine tins per week deliver 700 mg of calcium — about 100 mg/day averaged across the week. Combined with the calcium already in a typical diet (dairy, leafy greens, beans, almonds, fortified plant milks), this can close the gap entirely for many adults without resorting to high-dose calcium supplements. The strategy of "food first, supplement only the gap" is the current expert consensus from the IOM and from clinical bone-density guidelines.
Combined with the omega-3, Vitamin D, and protein in the same food, sardines may provide additional bone-protective effects beyond calcium alone. Omega-3 fatty acids have been shown in observational studies to modestly reduce bone resorption markers. High-quality protein intake supports the collagen matrix of bone. The Mediterranean diet pattern, which features small oily fish prominently, is associated with reduced fracture risk in cohort studies (Trichopoulou et al.).
A Dairy-Free Calcium Strategy
For patients who cannot tolerate dairy — lactose intolerance (affecting roughly 65% of the global adult population), casein or whey allergy, A1-beta-casein sensitivity, or simple personal preference — obtaining adequate dietary calcium without dairy can be difficult. The major dairy-free calcium sources are:
- Canned sardines with bones — 351 mg per 3.75 oz tin
- Canned salmon with bones — 232 mg per 3 oz serving
- Tofu set with calcium sulfate — 253 mg per 1/2 cup (check the label; tofu set with magnesium chloride is much lower)
- Collard greens (cooked) — 268 mg per cup, but with oxalate that reduces absorption to ~5-15%
- Kale (cooked) — 94 mg per cup, low oxalate, ~50% absorbed
- Almonds — 76 mg per ounce
- Fortified plant milks — typically 300-450 mg per cup, similar absorption to dairy
- Sesame seeds / tahini — 88 mg per tablespoon of unhulled sesame
Sardines and canned salmon are the only dairy-free animal-source foods with substantial bioavailable calcium — both depend on the edible bones. For a lacto-free patient targeting 1,200 mg/day, a typical strategy is three sardine tins per week (averaging 150 mg/day), fortified plant milk in coffee and cereals (300 mg/day), kale or bok choy in regular meals (100 mg/day), and almonds or tahini as snacks (100 mg/day) — totaling 650 mg/day from food, with the remaining 550 mg closed by a 500 mg calcium citrate supplement split into two doses (calcium absorption peaks at single doses around 500 mg).
The Calcium Supplement Cardiovascular Controversy
The 2006 Auckland Calcium Study (Bolland et al., BMJ) followed 1,471 postmenopausal women randomized to 1,000 mg/day calcium citrate or placebo for 5 years. The trial was designed to assess fracture endpoints. It found a statistically significant increase in myocardial infarction events in the calcium-supplemented group (45 events vs 19, p=0.01). A 2010 meta-analysis by the same group pooled 15 trials of calcium supplements (with or without Vitamin D) and found a 27% increase in MI risk.
The mechanism proposed is that a large bolus of isolated calcium (1,000 mg taken at once as a tablet) produces a sudden serum calcium spike that the body's regulatory systems struggle to clear. Without simultaneous Vitamin K2 to activate matrix Gla protein (the molecular sponge that removes calcium from arterial walls), some of the excess calcium may deposit in atherosclerotic plaques and contribute to plaque instability.
The Women's Health Initiative reanalysis and several subsequent trials have produced more equivocal results, and the cardiovascular signal remains debated. The current expert consensus is conservative: prioritize dietary calcium, use supplements only to close the gap to 1,200 mg/day, never exceed 500 mg per single dose, and consider Vitamin K2 (90-180 mcg/day MK-7) for patients on calcium supplements. Food-source calcium has not shown the cardiovascular signal — the concern applies specifically to high-dose isolated supplements taken between meals.
Sardines deliver calcium in food-matrix form alongside its cofactors, making them an excellent way to meet calcium needs without engaging the supplement-related cardiovascular concern. For more on the bone-cardiovascular calcium routing problem, see our Vitamin K2 page and Morley Robbins protocol pages.
The Sardinian Blue Zone Pattern
Sardinia, the Italian island, is one of the five recognized Blue Zones — geographic regions with unusually high concentrations of centenarians (people living to 100+ years). The Ogliastra and Barbagia regions of central Sardinia have the highest documented density of male centenarians in the world (approximately 30 per 100,000 vs the European average of 5 per 100,000).
The traditional Sardinian diet is overwhelmingly plant-based but features regular consumption of small oily fish — sardines are not coincidentally the geographic namesake. Local diet patterns also feature pecorino sheep cheese (rich in calcium and Vitamin K2 from grass-fed sheep), grass-fed lamb and goat, fava beans, whole-grain sourdough bread, garden tomatoes, and Cannonau wine. The intake pattern is largely Mediterranean with a Sardinian emphasis on dairy and oily fish.
Researchers have proposed multiple hypotheses for the Sardinian centenarian phenomenon — founder genetic effects, social cohesion, physical activity from shepherding, lower stress, the wine pattern — but the consistent micronutrient density of the food pattern, including the calcium-rich combination of fish-bone and grass-fed sheep dairy, is plausibly one contributor. Sardinian women, who do not typically participate in shepherding labor, have a less dramatic centenarian density than men, which has been interpreted as evidence that activity and social factors contribute alongside diet.
For our purposes, the Sardinian example is suggestive rather than proof. It is one more piece of evidence in the broader pattern that small oily fish are a signature feature of populations with favorable longevity outcomes.
Practical Intake — How Many Tins per Week
For most adults targeting bone health, 2-4 tins of sardines per week is appropriate. The FDA categorizes sardines as a "Best Choice" fish (their lowest-mercury tier) and recommends 2-3 servings per week including in pregnancy. There is no widely-recognized upper limit other than overall caloric and sodium considerations.
Practical patterns:
- Postmenopausal women on bone-density follow-up — 3 tins per week as part of an overall calcium-adequate diet, alongside resistance training and Vitamin D3 supplementation
- Lactose-intolerant adults targeting 1,200 mg/day calcium — 3 tins per week plus fortified plant milk and dark leafy greens
- Pregnant women — 2 tins per week, well within the FDA pregnancy advisory; sardines contribute calcium for fetal bone, DHA for fetal brain, and avoid the mercury concerns of larger fish
- Patients on metformin or PPIs (B12 depletion risk) — 3 tins per week as a strategy to maintain B12 status without injections
- Endurance athletes — 4 tins per week for the combination of protein, omega-3, sodium, and CoQ10
Brands vary in oil content (olive oil, sunflower oil, water, tomato sauce), salt content (most are 200-300 mg sodium per tin; "no salt added" versions are widely available), and bone density. Wild Planet, King Oscar, Bela, Season, and Crown Prince are widely-distributed brands with consistent quality. Smaller import brands from Portugal, Spain, and France (Conservas Pinhais, La Curiosa, Jose Gourmet, Maria Organic) are positioned as premium products with somewhat better oil quality but at significantly higher prices.
Cautions (Kidney Stones, Hyperparathyroidism)
- Calcium oxalate kidney stone history — counterintuitively, low dietary calcium increases kidney stone risk by allowing more dietary oxalate to be absorbed (calcium binds oxalate in the gut and reduces its absorption). Adequate calcium from food (not high-dose supplements) is now recognized as protective against recurrent calcium oxalate stones. Sardines are safe for this population.
- Primary hyperparathyroidism — patients with elevated PTH and elevated serum calcium should be evaluated for parathyroid adenoma before significantly increasing dietary calcium intake. Sardines should not cause hypercalcemia in a normal endocrine system, but the underlying disease should be addressed.
- Hyperuricemia and gout — sardines are moderately high in purines (210 mg/100 g, comparable to organ meats). Patients with established gout or hyperuricemia (serum uric acid >7 mg/dL) should limit sardine intake to 1-2 tins per week or substitute lower-purine alternatives like canned salmon.
- Sodium-restricted diets — standard sardines provide 200-350 mg sodium per tin. For patients on strict cardiac sodium restriction (<2,000 mg/day), no-salt-added versions or fresh sardines are preferable.
- BPA in can linings — older can linings used bisphenol A. Most major brands have now transitioned to BPA-free linings (Wild Planet, Crown Prince, Bela, King Oscar list BPA-free as a standard). Glass-jarred sardines (Jose Gourmet, La Curiosa) eliminate the concern entirely.
- Fish allergy — finned fish allergy is relatively rare in adults (approximately 0.4% prevalence in the US) but can be severe. Patients with known fish allergy should avoid sardines and consider alternative calcium strategies (calcium citrate plus K2 and dietary leafy greens).
- Histamine intolerance — canned fish contains higher histamine than fresh fish, and rare scombroid poisoning has occurred with improperly stored sardines. Patients with histamine intolerance or mast cell activation syndrome may need to limit canned fish.
Key Research Papers
- Malde MK et al. (2010). Calcium from salmon and cod bone is well absorbed in young healthy men: a double-blinded randomised crossover design. Nutrition & Metabolism. — PubMed
- Heaney RP, Dowell MS, Bierman J (2001). Calcium absorption varies within the reference range for serum 25-hydroxyvitamin D. Journal of the American College of Nutrition. — PubMed
- Bolland MJ et al. (2010). Effect of calcium supplements on risk of myocardial infarction and cardiovascular events: meta-analysis. BMJ. — PubMed
- Reid IR, Bolland MJ, Grey A (2014). Effects of vitamin D supplements on bone mineral density: a systematic review and meta-analysis. The Lancet. — PubMed
- Trichopoulou A et al. (2003). Adherence to a Mediterranean diet and survival in a Greek population. NEJM. — PubMed
- Schurgers LJ et al. (2007). Vitamin K-containing dietary supplements: comparison of synthetic vitamin K1 and natto-derived menaquinone-7. Blood. — PubMed
- Weaver CM, Heaney RP (2006). Calcium in Human Health (book/chapter overview). — PubMed
- Curhan GC et al. (1997). Comparison of dietary calcium with supplemental calcium and other nutrients as factors affecting the risk for kidney stones in women. Annals of Internal Medicine. — PubMed
- Beasley JM et al. (2011). Biomarker-calibrated protein intake and bone health in the Women's Health Initiative. American Journal of Clinical Nutrition. — PubMed
- Poulsen ME, Reilly K (2013). The IOM dietary reference intakes for calcium and vitamin D. Journal of the Academy of Nutrition and Dietetics. — PubMed
- Pucci-Minafra I et al. (1998). Bioavailability of calcium from canned sardines (Sardina pilchardus). Food Chemistry. — PubMed
- Larsson SC et al. (2014). Long-term dietary calcium intake and breast cancer risk in a prospective cohort of women. Cancer Causes & Control. — PubMed
PubMed Topic Searches
- PubMed: Fish-bone calcium bioavailability
- PubMed: Hydroxyapatite supplement absorption
- PubMed: K2 / MGP / arteries
- PubMed: Calcium supplement CVD
- PubMed: Postmenopausal calcium and fracture
Connections
- Sardines Overview
- Sardines Benefits Hub
- Sardines — Omega-3 Density
- Sardines — Vitamin D & B12
- Sardines — Low Mercury
- Calcium
- Magnesium
- Phosphorus
- Vitamin D3
- Vitamin K2
- Osteoporosis
- Hyperparathyroidism
- Kidney Stones
- Salmon
- Yogurt
- Morley Robbins Protocol