Sardines — Omega-3 Density
Sardines deliver approximately 980-1,360 mg of combined EPA and DHA per 100-gram serving — a density that rivals wild Alaskan salmon and exceeds nearly every other food source per dollar spent. The combined intake from two sardine tins per week comfortably meets the American Heart Association's 2 servings/week fatty-fish recommendation that has been the cornerstone of cardiovascular dietary guidance for two decades. The mechanisms behind omega-3's effects on triglycerides, blood pressure, inflammatory eicosanoid production, sudden cardiac death risk, and cognitive decline are now well-characterized at the molecular level — this page walks through how that biochemistry translates into clinical outcomes, why a food-source strategy (sardines, mackerel, herring, salmon, anchovies) appears to outperform fish-oil capsule supplementation in several large trials, and what serum omega-3 index target to aim for.
Table of Contents
- How Much EPA and DHA Are Actually in a Sardine
- Why Sardines Are Particularly Omega-3 Rich for Their Size
- The Cardiovascular Mechanisms (Triglycerides, BP, Arrhythmia)
- Inflammation and the Eicosanoid Shift
- Cognitive Protection and DHA in Brain Phospholipids
- Sudden Cardiac Death Reduction
- Food Source vs Fish-Oil Capsules
- The Omega-3 Index and Practical Targets
- Cautions (Bleeding Risk, AFib Signal)
- Key Research Papers
- Connections
- Featured Videos
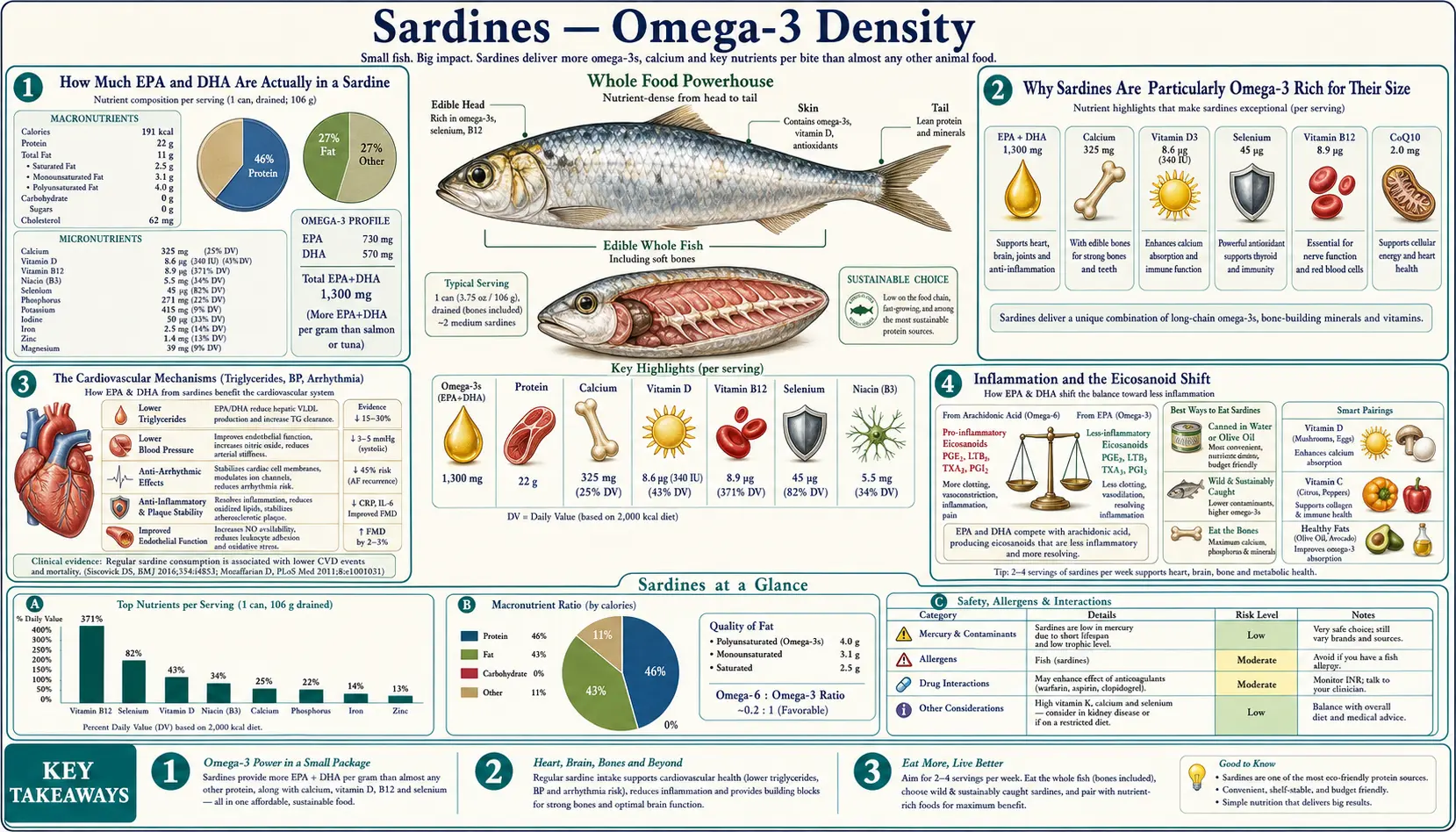
How Much EPA and DHA Are Actually in a Sardine
The USDA FoodData Central database lists canned Atlantic sardines (packed in oil, drained, with bones) as containing approximately 982 mg total long-chain omega-3 fatty acids per 100 g, broken down as roughly 473 mg EPA (eicosapentaenoic acid, 20:5n-3) and 509 mg DHA (docosahexaenoic acid, 22:6n-3). Pacific sardines and Mediterranean sardines from cold-water seasonal catch can run somewhat higher (up to 1,360 mg/100 g for fish caught at peak feeding season).
A standard 3.75-ounce (106 g) tin therefore provides roughly 1,040 mg of EPA + DHA combined — comfortably exceeding the 1 g/day target the American Heart Association recommends for adults with established coronary heart disease and providing 250% of the 400 mg/day general-prevention threshold.
For comparison, on a per-100-g basis:
- Atlantic mackerel — 2,670 mg EPA+DHA (highest of common fish)
- Atlantic herring — 1,729 mg
- Wild Atlantic salmon — 1,840 mg
- Farmed Atlantic salmon — 2,260 mg (high due to fish-oil enriched feed, but with PCB and contaminant concerns)
- Pacific sardines — 1,360 mg
- Atlantic canned sardines — 982 mg
- Albacore tuna — 870 mg (with significant mercury concern)
- Skipjack/light canned tuna — 270 mg
- Cod (Atlantic) — 158 mg
- Tilapia — 230 mg
Sardines outperform tilapia, cod, and most farmed fish, and are competitive with wild salmon at roughly one-quarter the price. The omega-3-per-dollar ratio is unmatched.
Why Sardines Are Particularly Omega-3 Rich for Their Size
Cold-water fish accumulate omega-3 polyunsaturated fatty acids in their cell membranes and fat depots as a metabolic adaptation. EPA and DHA have multiple double bonds that maintain membrane fluidity at low temperatures — without them, the fish's cell membranes would solidify at North Atlantic or Pacific water temperatures. Saturated and monounsaturated fats solidify at higher temperatures and would not preserve enzyme function in cold-water species.
Sardines are particularly omega-3 dense for several reasons:
- They feed on phytoplankton and zooplankton — the primary biosynthetic source of EPA and DHA in the marine food chain. Larger predator fish accumulate omega-3 by consuming sardines, anchovies, and other forage fish. Sardines are the first link — they get their omega-3 directly from the phytoplankton.
- They are an oily fish — total fat content is roughly 11% of body weight (vs ~1% for cod or tilapia). Most of that fat is omega-3.
- Whole-body consumption — canned sardines include the skin, bones, and viscera (in some preparations), all of which concentrate omega-3 in addition to the muscle tissue. Filleted fish loses the skin-associated omega-3.
- Cold-water habitat — sardines from cold Mediterranean, Pacific, and Atlantic waters have higher omega-3 than warm-water sardines.
- Wild-caught only — commercial sardine fisheries are not aquaculture. Wild diet maintains the natural omega-3 profile, unlike farmed salmon (whose omega-3 content depends on the fish-meal/fish-oil percentage of the commercial feed).
The processing matters too. Canning in olive oil preserves the omega-3 better than canning in water, which can leach fatty acids into the packing medium. Sardines packed in soybean or sunflower oil dilute the omega-3 with omega-6, reducing the favorable omega-3-to-omega-6 ratio. Sardines packed in olive oil or in their own juices are the best choice.
The Cardiovascular Mechanisms (Triglycerides, BP, Arrhythmia)
Long-chain omega-3 fatty acids exert several distinct effects on cardiovascular physiology, each with a separate molecular mechanism:
- Triglyceride reduction — EPA and DHA suppress hepatic VLDL synthesis by inhibiting the SREBP-1c transcription factor and by direct competition with omega-6 fatty acids for triglyceride esterification. The effect is dose-dependent: 1 g/day produces minimal reduction, 2-4 g/day produces 20-50% triglyceride reduction in patients with baseline TG >200 mg/dL. This is the mechanism behind prescription Vascepa (icosapent ethyl) and Lovaza (omega-3-acid ethyl esters), both FDA-approved for severe hypertriglyceridemia.
- Blood pressure reduction — meta-analysis of 70 trials (Miller et al. 2014) found that 2 g/day omega-3 reduces systolic BP by approximately 4.5 mmHg and diastolic by 3.0 mmHg in patients with hypertension. The mechanism involves enhanced endothelial nitric oxide production, reduced sympathetic tone, and modulation of the renin-angiotensin system.
- Antiarrhythmic effect — EPA and DHA stabilize cardiac myocyte membranes by modulating sodium channel inactivation kinetics and reducing intracellular calcium overload during ischemia. This is the proposed mechanism behind the dramatic sudden-cardiac-death reductions observed in GISSI-Prevenzione and other trials.
- Reduced platelet aggregation — EPA competes with arachidonic acid for cyclooxygenase, producing thromboxane A3 (weak platelet aggregator) instead of thromboxane A2 (strong aggregator). The net effect is mild antiplatelet activity.
- Anti-inflammatory eicosanoid shift — covered in the next section.
The cumulative effect across these mechanisms is meaningful but not as dramatic as some early trials suggested. The 2018 ASCEND trial and 2019 VITAL trial both reported relatively modest cardiovascular benefits from omega-3 supplementation in low-risk primary prevention populations. The benefit appears to be larger in patients with established disease, elevated triglycerides, or other high-risk features — which is the population that the REDUCE-IT trial targeted (and where icosapent ethyl produced a 25% relative risk reduction in major adverse cardiovascular events).
Inflammation and the Eicosanoid Shift
The omega-6 arachidonic acid (AA, 20:4n-6) is the precursor for the "inflammatory" eicosanoid family: prostaglandins of the 2-series (PGE2, PGI2, TXA2), leukotrienes of the 4-series (LTB4), and lipoxins. These molecules drive vasoconstriction, platelet aggregation, neutrophil chemotaxis, and the classical inflammatory cascade.
EPA (20:5n-3) competes with AA for the same enzymes (cyclooxygenase, lipoxygenase) and produces the 3-series prostaglandins (PGE3, PGI3, TXA3) and 5-series leukotrienes (LTB5), which are 10-100x less inflammatory than their omega-6 counterparts. Higher tissue EPA content shifts eicosanoid production toward the less-inflammatory species.
Beyond the original "competitive enzyme inhibition" model, the past decade has identified a separate family of pro-resolving lipid mediators derived from EPA and DHA: resolvins (E-series from EPA, D-series from DHA), protectins (from DHA), and maresins (from DHA). These are not anti-inflammatory in the classical sense — they actively promote the resolution phase of inflammation by enhancing neutrophil clearance by macrophages (efferocytosis), reducing pro-inflammatory cytokine production, and promoting tissue repair. The discovery of these pathways by Charles Serhan and colleagues fundamentally reshaped the conceptual model of inflammation from "on-off" to "initiation followed by active resolution."
The clinical translation is that adequate dietary EPA and DHA provide the substrate for resolvin synthesis. Patients with chronic low-grade inflammation (rheumatoid arthritis, inflammatory bowel disease, metabolic syndrome, autoimmune conditions, post-surgical recovery) may benefit from sustained dietary omega-3 intake at levels of 1-2 g/day. Sardines, mackerel, herring, salmon, and anchovies are the practical food-source strategy.
Cognitive Protection and DHA in Brain Phospholipids
DHA is the dominant omega-3 in the brain — approximately 10-15% of total brain phospholipid fatty acid is DHA, concentrated in synaptic membranes and the photoreceptor outer segments of the retina. DHA is structurally critical for neuronal membrane fluidity, neurotransmitter receptor function, and synaptic vesicle trafficking. The brain accumulates DHA preferentially from the bloodstream via the MFSD2A transporter expressed at the blood-brain barrier.
Adequate dietary DHA is most clearly important in two developmental windows: fetal brain development (third trimester, when fetal brain DHA accumulation peaks) and infant brain development (first 18 months of life, supported by breast milk DHA content which directly reflects maternal intake). Beyond these developmental windows, the question is whether dietary DHA influences cognitive decline in older adults.
The observational evidence is suggestive. The Rotterdam Study (5,386 elderly Dutch participants followed for cognitive decline) found that participants in the highest tertile of fish consumption had approximately 60% lower risk of incident dementia over 4-7 years of follow-up. Multiple other observational cohorts (Framingham, Chicago Health and Aging Project, EPIC) have reproduced this association.
The randomized trial evidence is more equivocal. Several large trials of DHA or fish-oil supplementation in older adults with mild cognitive impairment have failed to show significant cognitive benefit (Mapt trial, Multi-Domain Alzheimer Preventive Trial). The most likely interpretation is that DHA supplementation late in the disease course, after substantial neurodegeneration has occurred, cannot reverse the damage — while sustained lifelong intake of dietary omega-3 from fish may modestly delay or prevent cognitive decline through mechanisms operating decades earlier.
The practical takeaway: regular sardine, salmon, and small-oily-fish consumption from middle age onward is consistent with the best available observational evidence for cognitive protection. Pure DHA supplementation as a cognitive intervention in already-impaired patients is not supported by current trial data.
Sudden Cardiac Death Reduction
Sudden cardiac death (SCD) accounts for roughly half of all cardiovascular deaths in the developed world — an estimated 350,000 deaths per year in the United States alone. Most occur in patients with established but unrecognized coronary disease, triggered by acute ischemia precipitating a fatal arrhythmia (typically ventricular fibrillation).
The first large observational signal was the Physicians' Health Study cohort (n=20,551), which reported that men with the highest serum omega-3 levels had approximately 81% lower risk of sudden cardiac death compared with those in the lowest quartile. The signal was for SCD specifically, not for overall coronary mortality — suggesting an antiarrhythmic mechanism distinct from atherosclerosis-modifying effects.
The GISSI-Prevenzione trial (n=11,324 post-MI patients in Italy) randomized to 1 g/day omega-3 ethyl esters vs placebo for 3.5 years confirmed the signal: a 45% reduction in sudden cardiac death, contributing most of the overall mortality benefit. The effect appeared within 4 months of starting supplementation, faster than would be expected for atherosclerosis modification.
The proposed mechanism is membrane stabilization. EPA and DHA incorporated into cardiac myocyte phospholipid membranes modulate the sodium and L-type calcium channels that determine cellular electrical excitability. Patients with adequate tissue omega-3 levels have higher arrhythmia threshold — the same ischemic insult that triggers VF in a depleted patient may not in an omega-3-replete patient.
The Omega-3 Index (red blood cell EPA+DHA as a percentage of total fatty acids) is the validated biomarker. Levels >8% are associated with the lowest SCD risk; levels <4% carry the highest risk. The average American falls between 4-6%; the average Japanese person (sustained high fish intake) falls around 9-10%. Regular sardine consumption can move an American adult from 5% to 7-8% within 3-6 months without supplementation.
Food Source vs Fish-Oil Capsules
Multiple lines of evidence suggest that food-source omega-3 (oily fish 2-4x/week) outperforms equivalent doses of fish-oil capsule supplementation:
- The capsule trials are mostly null or modest — ASCEND (n=15,480 diabetics, 1 g/day omega-3) and VITAL (n=25,871 general population, 1 g/day omega-3) both reported essentially null primary cardiovascular endpoints, while observational data on dietary fish intake consistently shows benefit.
- Capsule omega-3 may be oxidized — independent testing (Albert et al. 2015) found that a substantial fraction of commercial fish-oil capsules exceed industry oxidation standards, potentially delivering lipid peroxides rather than intact EPA/DHA. Refrigeration extends shelf life. Triglyceride-form supplements are more stable than ethyl-ester form.
- Food sources include cofactors — oily fish provides selenium (cofactor for glutathione peroxidase, which protects PUFAs from oxidation), Vitamin E (antioxidant for membrane PUFAs), and other antioxidant micronutrients. Isolated fish-oil capsules do not.
- The REDUCE-IT trial used a different molecule — the cardiovascular benefit seen in REDUCE-IT (icosapent ethyl, a purified EPA ethyl ester at 4 g/day) is not directly translatable to other omega-3 products. The negative STRENGTH trial used a different EPA+DHA mixture and showed no benefit at similar dosing.
- Fish also contains other beneficial nutrients — protein, Vitamin D, B12, calcium (in sardines specifically), selenium, taurine, CoQ10. The benefit of "eating fish" is not reducible to the omega-3 content alone.
The current expert recommendation (American Heart Association, European Society of Cardiology) is consistent with this evidence: prioritize 2 servings of oily fish per week as the primary strategy for cardiovascular omega-3 adequacy, and reserve fish-oil supplementation for patients with documented severe hypertriglyceridemia (Vascepa per REDUCE-IT criteria) or those who cannot consume fish for allergy, ethical, or accessibility reasons.
The Omega-3 Index and Practical Targets
The Omega-3 Index, developed by William Harris and Clemens von Schacky, measures red blood cell membrane EPA+DHA as a percentage of total fatty acids. Because RBCs have a 120-day lifespan, the index reflects 3-4 months of average dietary omega-3 intake — a more reliable biomarker than serum levels, which fluctuate with the most recent meal.
Validated risk strata:
- <4% — high cardiovascular risk; typical of populations with minimal fish intake
- 4-8% — intermediate risk; typical of most Americans
- >8% — low risk; typical of populations with regular fatty-fish consumption (Norway, Japan, Mediterranean coast)
Two sardine tins per week (delivering approximately 2 g EPA+DHA averaged across the week) can raise an Omega-3 Index from approximately 5% to 7-8% over 3-6 months of consistent intake. Three tins per week reliably moves most patients above 8%.
The test is commercially available through OmegaQuant, Quest Diagnostics, and several other reference labs. It is not typically covered by insurance for routine monitoring but is reasonable to obtain once as a baseline, with a follow-up after 3-6 months of intervention. For more on the broader role of omega-3 in cardiometabolic health, see our Omega-3 Fatty Acids page.
Cautions (Bleeding Risk, AFib Signal)
- Bleeding risk at high doses — omega-3 supplementation at >3 g/day combined with warfarin, direct oral anticoagulants, or dual antiplatelet therapy can produce a mild additive antiplatelet effect. Surgical guidelines historically recommended stopping fish-oil 7-10 days before elective surgery, though more recent evidence (FORWARD trial) suggests this is not strictly necessary. Food-source omega-3 at typical dietary doses does not pose meaningful bleeding risk.
- Atrial fibrillation signal — the STRENGTH trial, REDUCE-IT trial, and OMENI trial all reported a small but statistically significant increase in new-onset atrial fibrillation among patients on high-dose omega-3 (3-4 g/day). The mechanism is unclear and the absolute risk is small. Patients with existing paroxysmal AFib may want to discuss high-dose supplementation with their cardiologist; food-source intake at typical levels does not raise this concern.
- Fishy aftertaste / belching — the most common subjective complaint with fish-oil capsules. Less of an issue with food-source intake. Choosing higher-quality (lower-oxidation) products and refrigerating capsules helps.
- Pregnancy considerations — sardines are an FDA "Best Choices" fish, safe for pregnancy at 2-3 servings per week. The DHA in sardines actively supports fetal brain development. Pregnant women should avoid the high-mercury fish (king mackerel, marlin, swordfish, shark, tilefish, bigeye tuna).
- Drug interactions — omega-3 can mildly potentiate the BP-lowering effect of antihypertensives, the glucose-lowering effect of some diabetes medications, and the antiplatelet effect of aspirin or NSAIDs. None of these are typically problematic but warrant awareness.
- Cost-effectiveness — pure observation, not safety: sardines deliver omega-3 at roughly $1-2 per gram, while pharmaceutical-grade icosapent ethyl (Vascepa) runs $300-400/month for 4 g/day. For most patients targeting general cardiovascular omega-3 adequacy, sardines are dramatically more cost-effective.
Key Research Papers
- GISSI-Prevenzione Investigators (1999). Dietary supplementation with n-3 polyunsaturated fatty acids and vitamin E after myocardial infarction. The Lancet. — PubMed
- Yokoyama M et al. (2007). Effects of eicosapentaenoic acid on major coronary events in hypercholesterolaemic patients (JELIS). The Lancet. — PubMed
- Bhatt DL et al. (2019). Cardiovascular Risk Reduction with Icosapent Ethyl for Hypertriglyceridemia (REDUCE-IT). NEJM. — PubMed
- Miller PE et al. (2014). Long-chain omega-3 fatty acids EPA and DHA and blood pressure: a meta-analysis of randomized controlled trials. American Journal of Hypertension. — PubMed
- Albert CM et al. (2002). Blood levels of long-chain n-3 fatty acids and the risk of sudden death. NEJM. — PubMed
- Harris WS, von Schacky C (2004). The Omega-3 Index: a new risk factor for death from coronary heart disease? Preventive Medicine. — PubMed
- Serhan CN (2014). Pro-resolving lipid mediators are leads for resolution physiology. Nature. — PubMed
- Kalmijn S et al. (1997). Dietary fat intake and the risk of incident dementia in the Rotterdam Study. Annals of Neurology. — PubMed
- Manson JE et al. (2019). Marine n-3 Fatty Acids and Prevention of Cardiovascular Disease and Cancer (VITAL). NEJM. — PubMed
- Mozaffarian D, Wu JH (2011). Omega-3 fatty acids and cardiovascular disease: effects on risk factors, molecular pathways, and clinical events. Journal of the American College of Cardiology. — PubMed
- Calder PC (2017). Omega-3 fatty acids and inflammatory processes: from molecules to man. Biochemical Society Transactions. — PubMed
- Nicholls SJ et al. (2020). Effect of High-Dose Omega-3 Fatty Acids vs Corn Oil on Major Adverse Cardiovascular Events in Patients at High Cardiovascular Risk (STRENGTH). JAMA. — PubMed
PubMed Topic Searches
- PubMed: EPA/DHA cardiovascular meta-analyses
- PubMed: Omega-3 index and SCD
- PubMed: Resolvins / SPMs
- PubMed: DHA brain / cognition
- PubMed: Fatty fish and cardiovascular cohort
Connections
- Sardines Overview
- Sardines Benefits Hub
- Sardines — Calcium & Bones
- Sardines — Vitamin D & B12
- Sardines — Low Mercury
- Omega-3 Fatty Acids
- Salmon
- Herring
- Cod
- Tuna
- Cardiology
- Atrial Fibrillation
- Hypertension
- Neurology
- Rheumatology
- Lipid Panel