Nausea and Vomiting
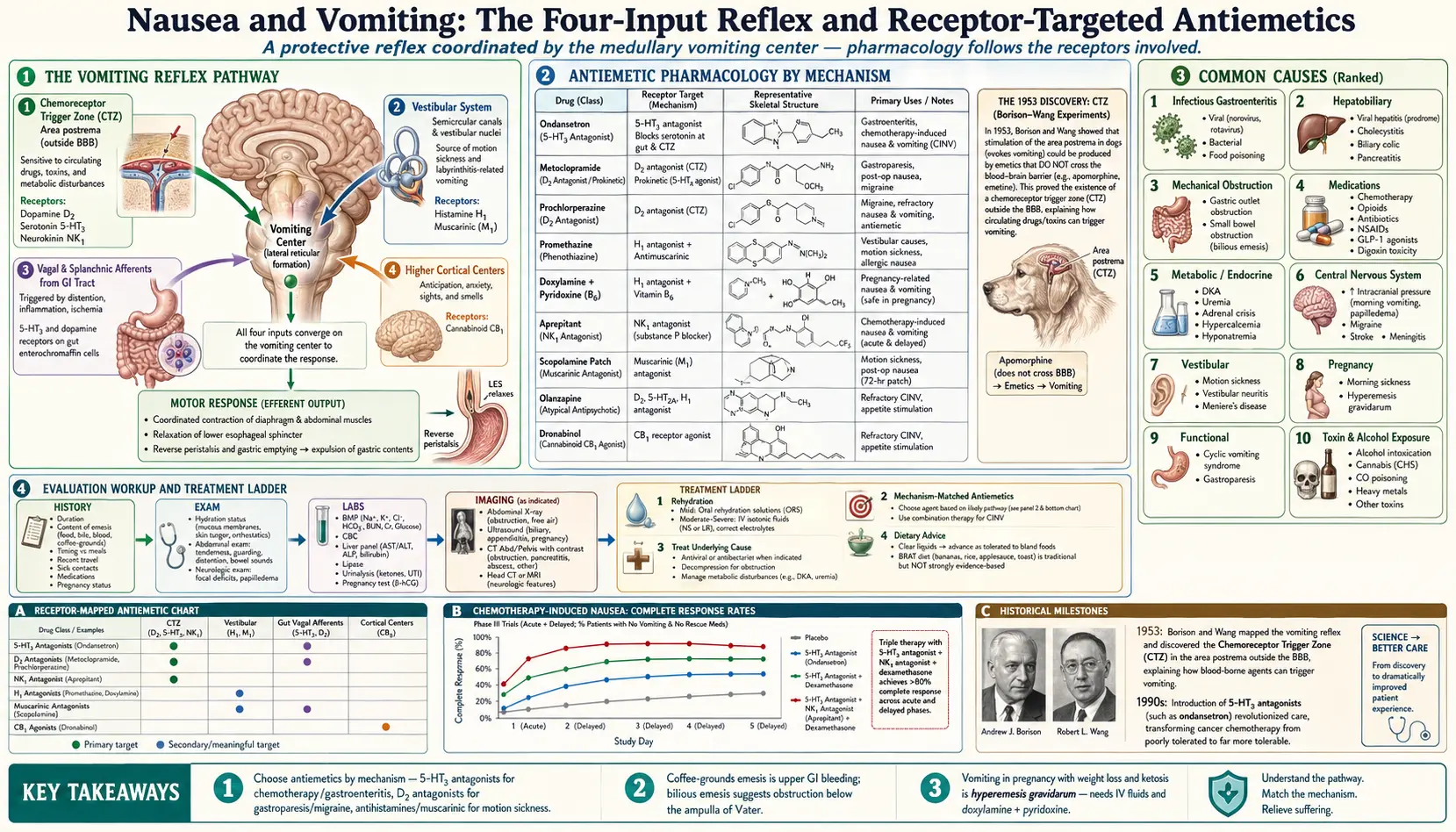

Table of Contents
- Overview
- The Vomiting Reflex
- Common Causes
- Evaluation
- Management
- When to Seek Medical Care
- Connections
- References & Research
- Featured Videos
Overview
Nausea is the unpleasant feeling that vomiting may be imminent. Vomiting is the forceful expulsion of stomach contents through the mouth. Both are protective reflexes — evolved to expel toxins and irritants — but they accompany an enormous range of conditions, from gastroenteritis and migraine to viral hepatitis, pregnancy, and serious abdominal emergencies. Persistent vomiting can rapidly cause dehydration and electrolyte disturbances.
The Vomiting Reflex
Vomiting is coordinated by the vomiting center in the medulla, which receives inputs from four major sources:
- Chemoreceptor trigger zone (CTZ) in the area postrema — sensitive to circulating drugs, toxins, and metabolic disturbances. Receptors include dopamine D2, serotonin 5-HT3, and neurokinin NK1.
- Vestibular system — the source of motion sickness and labyrinthitis-related vomiting.
- Vagal and splanchnic afferents from the GI tract — triggered by distention, inflammation, or ischemia.
- Higher cortical centers — anticipation, anxiety, sights, and smells.
Common Causes
- Infectious gastroenteritis — viral (norovirus, rotavirus), bacterial, food poisoning.
- Hepatobiliary — viral hepatitis, cholecystitis, biliary colic, pancreatitis.
- Mechanical obstruction — gastric outlet obstruction, small bowel obstruction.
- Medications — chemotherapy, opioids, antibiotics, NSAIDs, GLP-1 agonists, digoxin toxicity.
- Metabolic and endocrine — diabetic ketoacidosis, uremia, adrenal crisis, hypercalcemia, hyponatremia.
- Central nervous system — increased intracranial pressure, migraine, stroke, meningitis.
- Vestibular — motion sickness, vestibular neuritis, Ménière's disease.
- Pregnancy — morning sickness, hyperemesis gravidarum.
- Functional — cyclic vomiting syndrome, gastroparesis.
- Toxin and alcohol exposure.
Evaluation
- History — duration, content (food, bile, blood, coffee-grounds), timing relative to meals, recent travel, sick contacts, medications, pregnancy status.
- Physical exam — hydration status, abdominal exam for tenderness or distention, neurologic exam.
- Labs — basic metabolic panel (electrolytes, BUN, creatinine, glucose), CBC, lipase, liver panel, urinalysis, pregnancy test.
- Imaging — abdominal X-ray for obstruction; CT or ultrasound based on suspected cause; head CT/MRI for neurologic features.
Management
- Rehydration — oral rehydration solutions for mild cases, IV fluids for severe dehydration.
- Antiemetics chosen by mechanism:
- Ondansetron (5-HT3 antagonist) — first-line for gastroenteritis and chemotherapy.
- Metoclopramide and prochlorperazine (D2 antagonists) — gastroparesis, migraine.
- Promethazine — vestibular and motion sickness.
- Doxylamine + pyridoxine (B6) — pregnancy.
- Aprepitant (NK1 antagonist) — chemotherapy-induced.
- Treat the underlying cause — antiviral or antibacterial therapy when indicated, decompression for obstruction, management of metabolic disturbances.
- Dietary advice — clear liquids advancing to bland foods (the BRAT diet — bananas, rice, applesauce, toast — is traditional but not strongly evidence-based).
When to Seek Medical Care
- Vomiting blood or material that looks like coffee grounds.
- Severe abdominal pain, rigid abdomen, or fever.
- Signs of dehydration — dizziness, dry mouth, decreased urination, confusion.
- Severe headache, neck stiffness, focal weakness, or recent head injury.
- Unable to keep down fluids for more than 24 hours.
- Vomiting in pregnancy with weight loss or ketosis.
Connections
- Hepatitis
- Abdominal Pain
- Pancreatitis
- Migraine
- Diabetes
- Gallbladder Disease
- Loss of Appetite
- Ginger
- Migraine (Pain & Allergy)
- Anxiety
- Dizziness
- Headache
- Meningitis
- Stroke
- Urinalysis
- Bloating
- Hepatitis B
- Malaria
References & Research
Historical Background
The neuroanatomy of vomiting was mapped in the 1950s by Borison and Wang, who identified the chemoreceptor trigger zone in the area postrema and distinguished it from the vomiting center in the lateral reticular formation of the medulla. Their work explained why agents that do not cross the blood-brain barrier could still trigger vomiting, and laid the foundation for the development of targeted antiemetics — most notably the 5-HT3 antagonists in the 1990s, which transformed cancer chemotherapy.
Key Research Papers
- Quigley EM, Hasler WL, Parkman HP. AGA technical review on nausea and vomiting. Gastroenterology. 2001;120(1):263-286.
- Hesketh PJ. Chemotherapy-induced nausea and vomiting. New England Journal of Medicine. 2008;358(23):2482-2494.
- Niebyl JR. Nausea and vomiting in pregnancy. New England Journal of Medicine. 2010;363(16):1544-1550.
- Borison HL, Wang SC. Physiology and pharmacology of vomiting. Pharmacological Reviews. 1953;5(2):193-230.
- Camilleri M, Parkman HP, Shafi MA, Abell TL, Gerson L. Clinical guideline: management of gastroparesis. American Journal of Gastroenterology. 2013;108(1):18-37.
- Cubeddu LX, Hoffmann IS, Fuenmayor NT, Finn AL. Efficacy of ondansetron and the role of serotonin in cisplatin-induced nausea and vomiting. New England Journal of Medicine. 1990;322(12):810-816.
- Singh P, Yoon SS, Kuo B. Nausea: a review of pathophysiology and therapeutics. Therapeutic Advances in Gastroenterology. 2016;9(1):98-112.