Strongyloides stercoralis: The Autoinfecting Threadworm That Can Kill Immunocompromised Patients
Symptoms Overview
The full spectrum of Strongyloides disease — from chronic larva currens rash to fatal hyperinfection syndrome.
Larva Currens & Skin Symptoms
The racing larva rash, perianal itch, urticaria, eosinophilia, and Löffler's syndrome during lung migration.
Hyperinfection & Dissemination
When corticosteroids or HTLV-1 unleash massive larval autoinfection — gram-negative sepsis, ARDS, and 70–90% mortality.
Diagnosis: Stool Culture & Serology
Agar plate culture, Baermann funnel, ELISA serology, LIPS assay, and pre-immunosuppression screening algorithms.
Treatments Overview
Ivermectin as drug of choice, cure criteria, and management principles for complicated disease.
Ivermectin Treatment
Dosing, mechanism, bioavailability tips, cure rates (97%+), and post-treatment serology follow-up.
Hyperinfection Management
ICU protocol: extended ivermectin, broad-spectrum antibiotics, stopping immunosuppressants, HTLV-1 co-management.
Prevention & Screening
Pre-immunosuppression screening, mass drug administration, barefoot avoidance, and refugee health protocols.
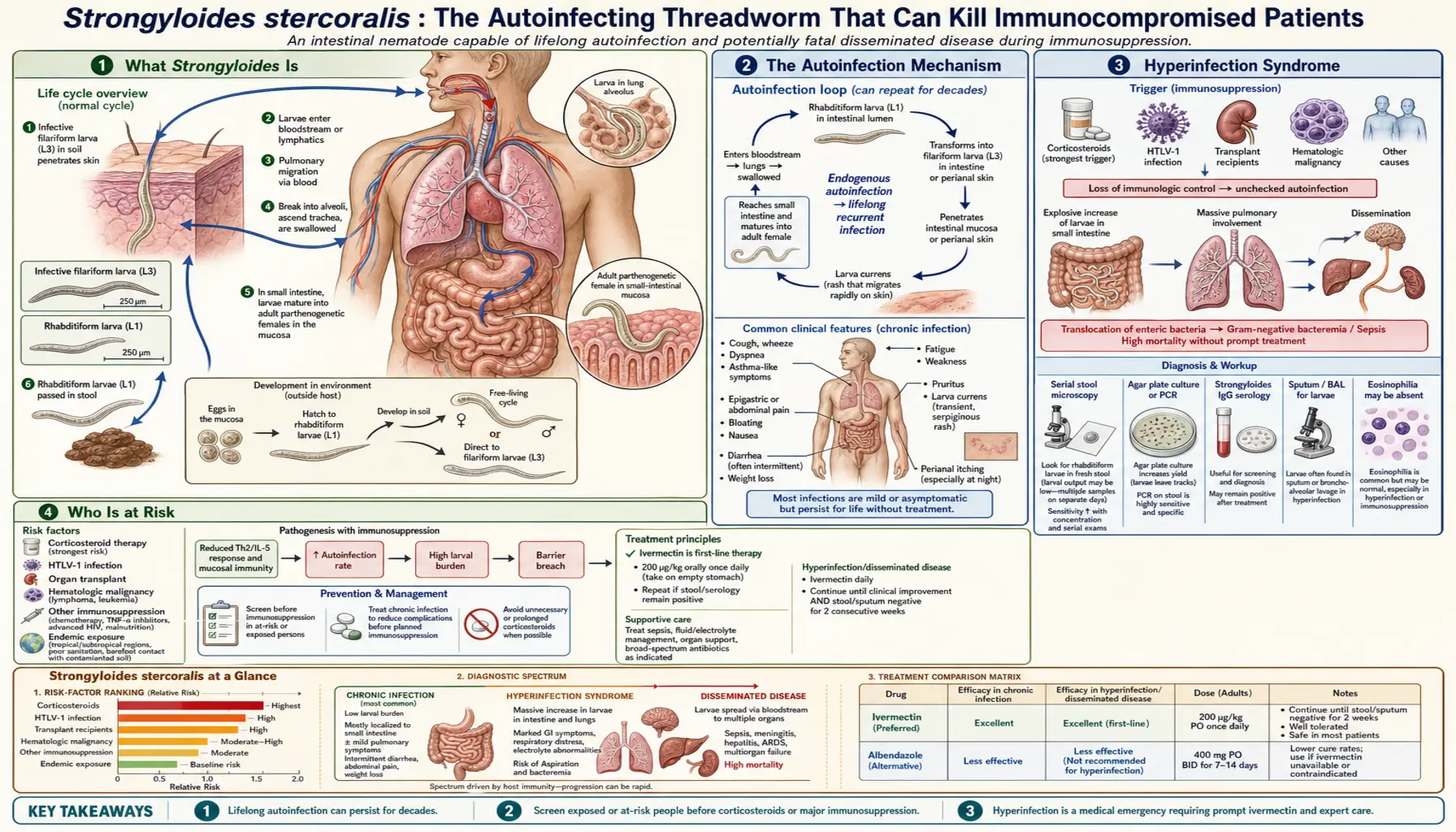
Strongyloides is unique among human parasites in its ability to autoinfect — completing its entire life cycle inside a single host indefinitely. In healthy people it causes mild GI symptoms; in people starting corticosteroids or with HTLV-1 infection, it can cause fatal hyperinfection syndrome with larvae disseminating to the brain, liver, and lungs. Globally, an estimated 100 million people harbor this threadworm, many without knowing it for decades.
Table of Contents
- What Strongyloides Is
- The Autoinfection Mechanism
- Hyperinfection Syndrome
- Who Is at Risk
- Symptoms
- Diagnosis
- Treatment (Ivermectin)
- Screening Before Immunosuppression
- Key Research Papers
- Featured Videos
1. What Strongyloides Is
Strongyloides stercoralis is a parasitic roundworm (nematode) belonging to the family Strongyloididae. Unlike most intestinal helminths, Strongyloides has a remarkable dual life cycle: it can exist as a free-living organism in soil or as an intestinal parasite in a human host. The adult parasitic female measures roughly 2–3 mm and lives embedded in the mucosa of the upper small intestine, producing eggs parthenogenetically (without fertilization). These hatch inside the gut into rhabditiform (L1) larvae, which are passed in feces.
Strongyloides is found in tropical and subtropical regions worldwide, with high prevalence in sub-Saharan Africa, Southeast Asia, and Latin America. It is also present in rural parts of Appalachia and the southeastern United States, and among immigrants and military veterans from endemic regions. An estimated 100 million people are currently infected globally, though precise numbers are uncertain because many cases are never diagnosed.
The critical distinguishing feature of Strongyloides compared with all other intestinal helminths is its capacity for autoinfection: larvae can reinvade the same host without leaving the body. This means that a person infected decades ago — perhaps as a child in an endemic region — can still carry the parasite today.
2. The Autoinfection Mechanism
In most intestinal worm infections, the worm must leave the host (via feces) to reach the environment and develop to an infective stage before reinfecting someone. Strongyloides breaks this rule. Some rhabditiform larvae, instead of passing out in stool, transform into infective filariform (L3) larvae while still inside the intestine or on the perianal skin. These filariform larvae can then penetrate the gut wall or the perianal skin directly, re-enter the circulation, migrate through the lungs, and return to the small intestine to restart the cycle — all without ever leaving the body.
This endogenous autoinfection allows the parasite to persist indefinitely in a single host. In immunocompetent individuals, the immune system (particularly IgE antibodies and eosinophils) limits the rate of autoinfection to a low, tolerated level. The worm burden stays roughly constant, and most people have chronic low-grade infection for years or decades. The danger emerges when immune control is disrupted.
3. Hyperinfection Syndrome
When cellular immunity is impaired — most dangerously by corticosteroids — the brake on autoinfection is released. Larvae complete the endogenous cycle at a massively accelerated rate, producing hyperinfection syndrome: an explosive amplification of worm burden throughout the gut and lungs. Patients develop severe diarrhea, abdominal pain, vomiting, and pulmonary symptoms (cough, wheeze, hemoptysis) as larvae stream through the lungs.
In the most severe form, disseminated strongyloidiasis, larvae carry gut bacteria through the bowel wall into the bloodstream, seeding the liver, heart, kidneys, brain, and meninges with both worms and enteric organisms. Gram-negative bacteremia and bacterial meningitis often complicate disseminated infection. Mortality in disseminated strongyloidiasis exceeds 70% even with treatment. This devastating outcome can be triggered by a single course of corticosteroids in a patient who was never tested for Strongyloides.
4. Who Is at Risk
Healthy immunocompetent individuals carry Strongyloides with minimal symptoms, and the infection remains well-controlled by the immune system indefinitely. Risk of hyperinfection or dissemination is concentrated in specific groups:
- Corticosteroid users: Even a short course of prednisone can trigger hyperinfection in someone with undiagnosed chronic strongyloidiasis. Corticosteroids both suppress eosinophil activity (removing the anti-larval defense) and directly stimulate larval development through glucocorticoid receptor activation on the parasites themselves. This is the most important risk group in clinical practice.
- HTLV-1 infection: Human T-lymphotropic virus type 1 (HTLV-1) specifically depletes Th2 immunity — the arm of the immune response that controls Strongyloides. HTLV-1-positive individuals have markedly elevated rates of hyperinfection and dissemination. The combination of HTLV-1 and Strongyloides co-endemicity in parts of Japan, the Caribbean, and South America is clinically significant.
- Organ transplant recipients on immunosuppressive regimens, patients with hematologic malignancies, and those receiving biological agents that deplete T cells.
- Malnutrition and achlorhydria (low stomach acid) may also impair normal barriers to infection.
5. Symptoms
Chronic uncomplicated strongyloidiasis in immunocompetent individuals is often asymptomatic or produces only nonspecific complaints. When symptoms occur, the most characteristic is larva currens: a rapidly migrating, itching, urticarial rash on the trunk and buttocks that tracks the path of migrating larvae just under the skin. It can appear and disappear within hours and recur episodically over years.
Gastrointestinal symptoms include intermittent diarrhea, constipation, nausea, abdominal bloating, and epigastric pain. These are nonspecific and easily attributed to other causes, contributing to delayed diagnosis. Eosinophilia on a blood count (elevated eosinophil percentage) is an important clue — often the only laboratory abnormality — and should trigger Strongyloides testing in anyone from an endemic area or with relevant risk factors.
Pulmonary symptoms (cough, wheeze, transient infiltrates on chest X-ray) can occur during the pulmonary migration phase of larval development — a presentation similar to Löffler syndrome. In hyperinfection, pulmonary symptoms become severe and may include massive pulmonary hemorrhage.
6. Diagnosis
Diagnosis of strongyloidiasis requires a high index of suspicion, particularly in returned travelers, immigrants from endemic regions, and anyone about to start immunosuppressive therapy.
- Serology (IgG ELISA): The most sensitive test for chronic infection. Sensitivity ranges from 80–90% in immunocompetent individuals; sensitivity is paradoxically lower in immunocompromised patients because their antibody responses are impaired. Serology is the preferred initial test for screening.
- Stool examination (ova and parasites, O&P): Finding larvae in stool confirms active infection but requires multiple samples and experienced examination, since larval shedding is intermittent. A single stool O&P examination has sensitivity of only about 25%; sensitivity improves with multiple samples or the Baermann concentration technique.
- Stool culture (agar plate culture): Detects larvae by observing their migration tracks on an agar plate; more sensitive than direct stool O&P but requires laboratory expertise.
- PCR on stool: Available at reference laboratories; higher sensitivity than microscopy but not yet widely standardized.
- Duodenal aspirate or biopsy: Can directly demonstrate adult worms or larvae in the small intestine; reserved for cases where non-invasive testing is negative but suspicion remains high.
7. Treatment (Ivermectin)
Ivermectin is the treatment of choice for Strongyloides infection. Given orally at 200 μg/kg/day for two days (standard uncomplicated infection), it achieves cure rates of over 95%, substantially superior to the previously standard drug albendazole. For hyperinfection or disseminated disease, treatment is continued until larvae are undetectable in stool, which may require weeks of therapy because the drug does not penetrate the gut wall where larvae reenter during autoinfection.
Ivermectin works by opening glutamate-gated chloride channels in nematode neurons and muscle, causing paralysis and death of the parasite. It is well-tolerated with few significant side effects in standard doses, which is why it is preferred. In patients with disseminated strongyloidiasis, treatment must also address the bacterial superinfections that commonly accompany larval migration through the gut wall.
Albendazole (400 mg twice daily for 7 days) is an alternative when ivermectin is unavailable, but cure rates are lower (approximately 60–70%). Thiabendazole, the original treatment, is rarely used today due to its poorer tolerability.
8. Screening Before Immunosuppression
The most important practical message about Strongyloides is one of prevention through screening. Any patient who may have been exposed to Strongyloides — through birth or residence in an endemic region, rural tropical travel, or known risk factors — should be tested before starting corticosteroids, transplant immunosuppression, or anti-T cell biologics.
The test of choice for pre-immunosuppression screening is serology (IgG ELISA). A positive result should prompt treatment with ivermectin before immunosuppression begins. This simple intervention prevents hyperinfection syndrome entirely. Many cases of fatal disseminated strongyloidiasis occur in patients who received no such screening, underscoring the importance of a careful travel and exposure history in clinical practice.
In patients with established HTLV-1 infection, screening for Strongyloides is standard of care in most guidelines, given the particularly high risk of co-infection and hyperinfection in this group.
Key Research Papers
Landmark studies and reviews on Strongyloides stercoralis biology, hyperinfection, and treatment.
- Siddiqui AA, Berk SL. Diagnosis of Strongyloides stercoralis Infection. Clinical Infectious Diseases. — Search PubMed [PubMed PMID 11340529]
- Lim S, Katz K, Krajden S, Fuksa M, Keystone JS, Kain KC. Complicated and Fatal Strongyloides Infection in Canadians. Canadian Medical Association Journal. — Search PubMed [PubMed PMID 15337727]
- Nutman TB. Human Infection with Strongyloides stercoralis and Other Related Strongyloides Species. Parasitology. 2017;144(3):263–273. [PubMed PMID 27181117]
- Bisoffi Z, Buonfrate D, Montresor A, et al. Strongyloides stercoralis: A Plea for Action. PLOS Neglected Tropical Diseases. — Search PubMed [PubMed PMID 23285307]
- Mejia R, Nutman TB. Screening, Prevention, and Treatment for Hyperinfection Syndrome and Disseminated Infections Caused by Strongyloides stercoralis. Current Opinion in Infectious Diseases. — Search PubMed [PubMed PMID 22130345]
Live PubMed Searches
- Strongyloides hyperinfection
- Strongyloides ivermectin treatment
- Strongyloides HTLV-1
- Strongyloides screening before immunosuppression
- Strongyloides + corticosteroids
- Strongyloidiasis autoinfection eosinophilia
Connections
- Strongyloides Symptoms
- Strongyloides Treatments
- All Parasites
- Hookworm
- Ascaris
- Pinworm
- Toxocara
- Gastroenterology
- Infectious Disease
- All Conditions
- Strongyloidiasis