Diagnosing Strongyloides — Stool Culture, Serology, and Screening
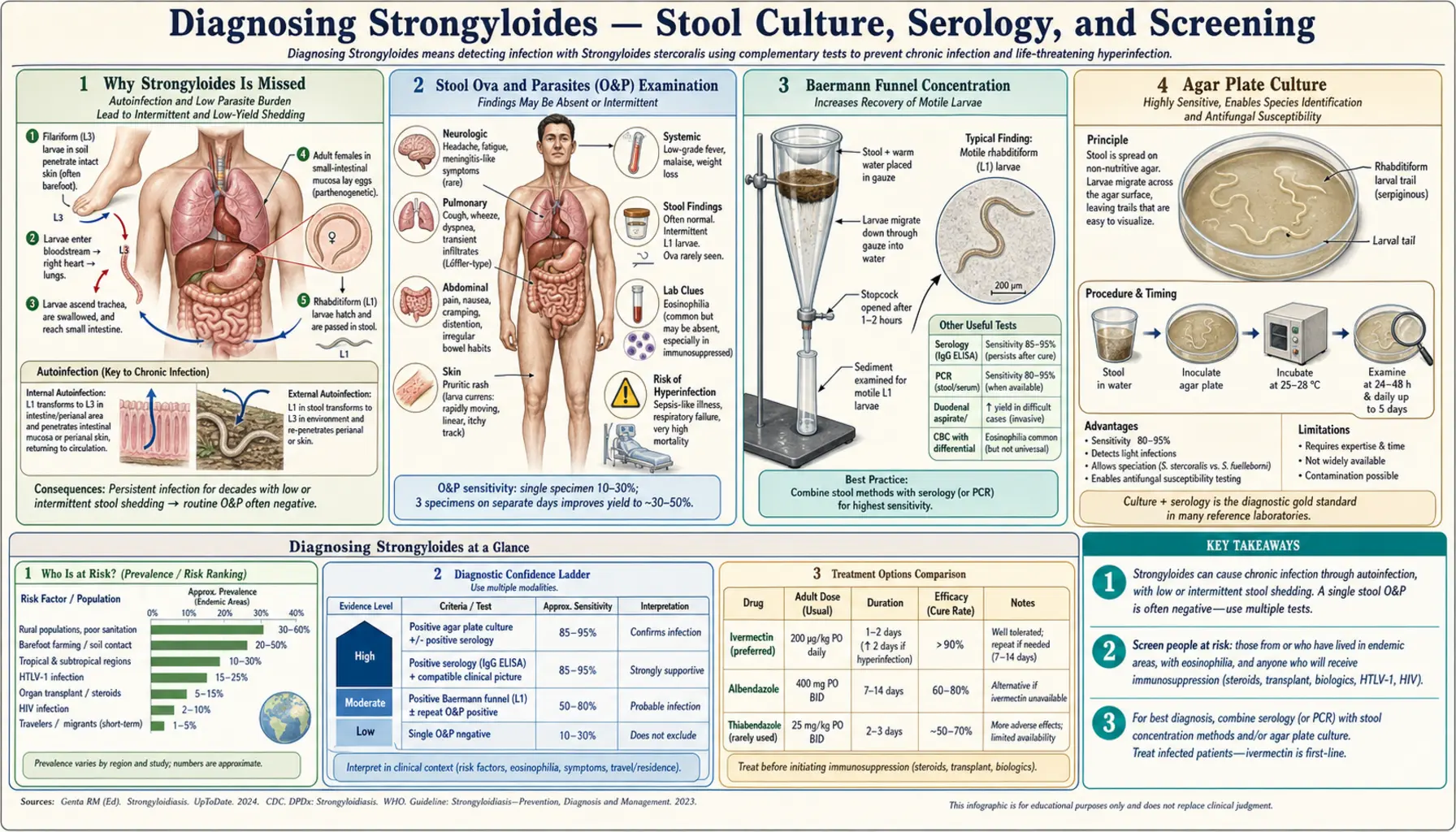
Table of Contents
- Why Strongyloides Is Missed
- Stool Ova and Parasites (O&P) Examination
- Baermann Funnel Concentration
- Agar Plate Culture
- Harada-Mori Filter Paper Culture
- Serology (IgG ELISA)
- Luciferase Immunoprecipitation System (LIPS)
- Duodenal Aspiration and Biopsy
- Eosinophilia as a Diagnostic Clue
- Pre-Immunosuppression Screening Algorithm
- Key Research Papers
- PubMed Searches
- Connections
- Featured Videos
Why Strongyloides Is Missed
Strongyloides is the most commonly missed soil-transmitted helminth in clinical practice. Three reasons dominate. First, larval output is intermittent: rhabditiform larvae appear in stool only when the lifecycle is in a shedding phase, which can vary day to day. A single stool exam catches only 25–30% of infections. Second, symptoms overlap with irritable bowel syndrome, peptic ulcer disease, and eosinophilic gastroenteritis — all common, all diagnosed before strongyloides is considered. Third, outside endemic-country hospitals, most clinicians in North America, Europe, and Australia have never seen a case and keep it off their differential.
The result: patients go years to decades with chronic infection, only presenting to medical attention when immunosuppression triggers hyperinfection. By then, the window for easy treatment has passed. The stakes could not be higher — hyperinfection carries a mortality rate exceeding 80% without rapid diagnosis and treatment. Every missed case of chronic strongyloidiasis is a potential future hyperinfection fatality waiting to happen.
A further complication: the parasite is geographically underestimated. Classic teaching places Strongyloides in the tropics and subtropics, but autochthonous transmission occurs in Appalachia, the rural US South, and parts of eastern Europe. Veterans returning from Vietnam, Korea, and the Pacific theater who were never treated still carry active infections decades later. Immigrants from endemic regions may be seronegative on routine screening panels that don't include Strongyloides. Clinicians must maintain a high index of suspicion in any patient with unexplained gastrointestinal symptoms plus one or more of: travel to or residence in endemic regions, eosinophilia, immunosuppression, or HTLV-1 infection.
Stool Ova and Parasites (O&P) Examination
The standard stool O&P exam, while inexpensive and widely available, has poor sensitivity for Strongyloides. A single stool exam detects larvae in only 25–30% of infected individuals. The reason is the intermittent pattern of larval output — on days when larvae aren't shedding, the exam is negative regardless of infection burden. Examining three separate stool specimens on different days raises sensitivity to approximately 60–70%, still unacceptably low for a potentially fatal condition.
The exam must be processed quickly: larvae are motile and can be missed if the sample sits. Fresh warm stool directly plated is preferable to formalin-fixed specimens, which kill larvae and make identification harder. When ordering a stool O&P, explicitly write "evaluate for Strongyloides larvae" on the requisition — this alerts the laboratory to use techniques appropriate for larval detection rather than relying solely on concentration methods designed for eggs and cysts, which are inadequate for Strongyloides.
Even expert parasitologists miss infections on direct exam. Rhabditiform larvae are approximately 250 μm long, transparent, and can be confused with free-living nematodes or cellular debris if the microscopist is not specifically looking for them. The characteristic feature is a short buccal cavity and a prominent genital primordium visible under 100x magnification. Filariform (infective) larvae, which are longer (approximately 500 μm) with a notched tail, may also be present if stool has sat for more than a few hours and larval development has progressed.
Given the poor sensitivity of a single O&P, it should never be used as the sole diagnostic test when clinical suspicion is present. Combine it with serology and, ideally, agar plate culture for the highest diagnostic yield.
Baermann Funnel Concentration
The Baermann method exploits larval thermotropism — Strongyloides larvae migrate toward warmth. Fresh stool is placed in a funnel lined with gauze or cheesecloth over warm water (37–40°C); larvae migrate through the gauze, settle at the bottom of the water column, and are collected by opening the valve at the base of the funnel. The sediment is then examined microscopically for motile rhabditiform larvae.
Sensitivity is approximately 40–50% for a single sample, modestly better than direct exam but still imperfect. The major advantage is its simplicity: no specialized equipment or reagents are required beyond a standard laboratory funnel, gauze, and a warm water source. It works well in resource-limited settings where agar plate culture is not available. Multiple-day samples can be pooled to improve yield — running three consecutive day samples through Baermann concentration raises sensitivity to approximately 65–75%.
The method works only with fresh stool (not formalin-fixed) and requires larvae to be alive and actively migrating. Samples more than 2 hours old give poor results because larvae lose motility and thermotropic behavior as they die. The technique is temperature-sensitive: water that is too cool (below 35°C) won't stimulate migration effectively; water that is too hot (above 42°C) kills larvae. The optimal temperature window is narrow, requiring attention to water temperature throughout the procedure. Despite these limitations, Baermann remains a valuable tool in tropical field surveys and in laboratories where agar plate culture is not available.
Agar Plate Culture
Agar plate culture (APC) is the gold standard for stool-based Strongyloides diagnosis, with sensitivity exceeding 90% for single samples in multiple validation studies. The technique was developed in the 1990s and has significantly improved the laboratory diagnosis of strongyloidiasis in institutions that have adopted it. Fresh stool (approximately 1 gram) is placed in the center of a nutrient agar plate and incubated at room temperature (25–28°C) for 48–72 hours. Strongyloides larvae migrate outward from the stool across the agar surface, carrying bacterial colonies from the gut flora as they travel. These bacteria grow in the trails left by larvae, creating visible sinuous tracks radiating from the stool inoculum.
The plate is then examined under low-power microscopy (4x or 10x objective). Larvae can be found at the ends of the tracks, still motile. The visible bacterial tracks are the key diagnostic feature — they make larval tracks apparent even to laboratory staff who have not seen many Strongyloides cases. The plate should be sealed with Parafilm after inoculation to prevent environmental contamination and to keep larvae from escaping the plate.
APC requires fresh stool (not fixed), 48–72 hours of incubation, and laboratory staff trained to recognize larval tracks, which can be subtle when larval density is low. The technique is not universally available — many clinical laboratories in North America and Europe have never set it up. When a patient with suspected strongyloidiasis presents, it is worth calling the laboratory director directly to confirm that APC is available or to arrange referral to a reference parasitology laboratory that performs it. The combination of three APC samples on consecutive days approaches 100% sensitivity and should be considered the diagnostic endpoint before concluding that stool-based testing is negative.
Harada-Mori Filter Paper Culture
The Harada-Mori technique was developed in Japan in the 1950s as a low-cost, low-technology method for larval culture of soil-transmitted helminths. A thin smear of fresh stool is applied to a strip of filter paper. The strip is then placed vertically in a test tube containing a small amount of water (enough to keep the lower end of the strip moist without touching the stool smear). The tube is incubated at 25–28°C for 7–10 days. Strongyloides larvae hatch from eggs or continue developing from rhabditiform to filariform stage and migrate into the water at the bottom of the tube, where they can be seen with the naked eye as small wriggling threads or examined under low-power microscopy.
Sensitivity is roughly comparable to Baermann (40–50%) for a single sample. The long incubation period (7–10 days versus 48–72 hours for APC) is a significant clinical disadvantage when urgent diagnosis is needed. Harada-Mori cannot distinguish Strongyloides from hookworm larvae in the early days of incubation — both species hatch from similar rhabditiform larvae. By day 7–10, filariform larvae of both species are present, and distinguishing them requires careful morphologic examination (Strongyloides filariform larvae have a notched tail; hookworm filariform larvae have a pointed tail and a longer buccal cavity). This identification step requires an experienced parasitologist.
Harada-Mori is more commonly used in epidemiological surveys in endemic countries than in individual patient diagnosis in Western clinical settings. It remains valuable in field conditions where agar plates and incubators are not available. Some reference laboratories use modified Harada-Mori as a complement to APC, particularly for samples where larval density is expected to be very low.
Serology (IgG ELISA)
Serologic detection of anti-Strongyloides IgG by enzyme-linked immunosorbent assay (ELISA) is the preferred screening method for immunocompetent patients presenting with suspected strongyloidiasis or for pre-immunosuppression screening. The test measures antibodies directed against Strongyloides larval antigens — either crude somatic extracts or purified recombinant antigens depending on the assay platform. Sensitivity ranges from 80–90% and specificity exceeds 95% in most published studies using well-characterized patient cohorts and purified larval antigens.
The major limitation is cross-reactivity with other helminths. Filarial nematodes (Wuchereria bancrofti, Brugia malayi, Loa loa) share antigenic epitopes with Strongyloides and can produce false-positive results. Ascaris lumbricoides and Toxocara canis have also been associated with ELISA cross-reactivity in some assay platforms. This is clinically significant for patients from regions where multiple parasitic infections co-exist. In the United States and northern Europe, where filariasis is not endemic, a positive ELISA in a patient from rural Latin America, Southeast Asia, or sub-Saharan Africa is highly predictive of true Strongyloides infection.
A critical limitation: serology has reduced sensitivity in immunocompromised patients — the very group who most need accurate diagnosis. Patients on high-dose corticosteroids, those with HTLV-1 co-infection, solid organ transplant recipients on calcineurin inhibitors, and individuals with advanced HIV cannot mount a robust antibody response, leading to false-negative serology despite heavy worm burden. The ELISA titer may even fall after initiation of immunosuppression while infection is intensifying. Clinicians must not use a negative serology to rule out strongyloides in immunocompromised patients; negative serology in this context should prompt stool culture and duodenal sampling.
IgG ELISA is commercially available at most reference laboratories in the United States (e.g., ARUP, Quest, LabCorp). The test is ordered as "Strongyloides antibody IgG" or "Strongyloides stercoralis serology." Turnaround is typically 3–7 days. A titer of ≥1:128 (or equivalent optical density depending on assay platform) is generally considered positive. Serial titers can be used to confirm treatment response: successful eradication with ivermectin results in a declining antibody titer over 6–12 months, though titers may not completely normalize for 1–2 years even after cure.
Luciferase Immunoprecipitation System (LIPS)
The Luciferase Immunoprecipitation System (LIPS) represents the most significant advance in Strongyloides serology in the past two decades. LIPS uses recombinant Strongyloides antigens — specifically the NIE (nematode-immunodominant epitope) antigen — expressed as fusion proteins with Renilla luciferase, a bioluminescent enzyme derived from sea pansy. When patient serum is added to the recombinant antigen-luciferase fusion protein, specific anti-Strongyloides antibodies bind and immunoprecipitate the complex. Unbound protein is washed away. The remaining complex is then assayed for luciferase activity, which is directly proportional to the amount of specific antibody present. The result is expressed in light units (LU).
Validation studies from the National Institutes of Health (NIH) and international collaborators have demonstrated sensitivity approaching 97% and specificity exceeding 99% for LIPS using the NIE antigen. The dramatic improvement in specificity over conventional ELISA is attributable to the use of a single recombinant antigen (NIE) that is highly specific to Strongyloides, largely avoiding the cross-reactive epitopes present in crude somatic extracts used in most commercial ELISA assays. LIPS has been validated in patients from filaria-endemic regions and correctly distinguished strongyloidiasis from filarial infections in the vast majority of cases — a clinical scenario where conventional ELISA frequently fails.
The LIPS assay is quantitative, allowing serial monitoring of treatment response with greater precision than ELISA titer measurements. In treatment studies, LIPS LU values declined by 50% or more within 6 months of successful ivermectin therapy and returned to negative range within 12–24 months in most patients. This makes LIPS particularly valuable for monitoring cure in immunocompromised patients where clinical response may be ambiguous.
The primary limitation of LIPS is availability. The assay requires specialized laboratory infrastructure — a luminometer, the NIE-luciferase construct, and technical staff trained in the protocol. As of current reporting, LIPS is available only at the NIH National Institute of Allergy and Infectious Diseases and a small number of academic reference laboratories. It is not commercially available in most countries. Clinicians who need LIPS testing must contact the NIH Parasitology Research Unit directly for sample submission protocols. Despite this limitation, LIPS is the diagnostic method of choice for research studies, clinical trials of Strongyloides treatment, and individual cases where conventional serology is ambiguous and the clinical stakes are high.
Duodenal Aspiration and Biopsy
When non-invasive tests are negative but clinical suspicion remains high — particularly in immunocompromised patients where serology may be falsely negative and stool cultures may be inadequate — duodenal aspiration or small bowel biopsy can provide definitive diagnosis. These invasive techniques are reserved for cases where the stakes are highest and other methods have failed.
Upper endoscopy with aspiration of duodenal contents directly recovers Strongyloides larvae from the intestinal lumen. The procedure involves standard upper endoscopy; upon reaching the second or third portion of the duodenum, the endoscopist aspirates 10–20 mL of duodenal fluid through the biopsy channel. The fluid is immediately examined by the laboratory under low-power microscopy for motile rhabditiform larvae. Sensitivity in published series is approximately 76% — higher than single O&P stool exams but lower than agar plate culture of multiple specimens. The advantage is direct sampling of the parasite's primary habitat: Strongyloides adult females embed in the duodenal mucosa and lay eggs there, so larval concentration is highest in duodenal fluid compared with stool collected at a distance from the infection site.
Biopsy of the duodenum or proximal jejunum provides tissue diagnosis and can reveal the full spectrum of intestinal pathology caused by Strongyloides. In uncomplicated chronic infection, histology may show subtle changes: eosinophilic infiltration of the lamina propria, villous blunting, and larvae within intestinal crypts visible on H&E staining. In hyperinfection, the findings are dramatic: larvae penetrating through all layers of the bowel wall, from the mucosa through the muscularis propria to the serosa. This transmural invasion is the anatomic basis for the sepsis cascade in hyperinfection, as enteric bacteria traverse the same routes alongside larvae.
Endoscopic findings in Strongyloides can range from normal (most common in chronic infection) to mucosal edema, erosions, and occasionally a characteristic "cobblestone" pattern representing larval tracking through the submucosa. In very heavy infection, white nodular lesions may be visible endoscopically, representing larval clusters within the mucosa. The endoscopist should sample any abnormal-appearing mucosa for both histology and direct smear.
The Enterotest (string test), an older technique involving a gelatin capsule attached to a string that the patient swallows and retrieves 4 hours later, has largely been replaced by endoscopy but remains available at some institutions. It samples proximal small intestinal contents and can recover larvae in immunocompromised patients when endoscopy is not feasible or immediately available.
Eosinophilia as a Diagnostic Clue
Peripheral blood eosinophilia — defined as an absolute eosinophil count greater than 500 cells per microliter — is present in 60–70% of patients with chronic uncomplicated strongyloidiasis. This is the body's immune response to the tissue migration phase of the parasite's lifecycle: as larvae penetrate the skin, migrate through the bloodstream and lungs, and traverse the bowel wall, they stimulate a vigorous eosinophilic response driven by IL-5, IL-4, and IL-13 signaling from activated Th2 lymphocytes. The eosinophil count typically ranges from 500 to 3,000 cells/μL in uncomplicated chronic infection, though counts exceeding 5,000 cells/μL are not uncommon.
In returning travelers and immigrants from endemic regions, unexplained eosinophilia should always prompt Strongyloides testing. The differential diagnosis of travel-associated eosinophilia includes many helminths — hookworm, ascaris, toxocara, schistosomiasis, filariasis, trichinellosis — and Strongyloides should be high on the list for any patient with relevant travel exposure, particularly to rural tropical areas. A useful clinical rule: eosinophilia in a returning traveler or immigrant that has persisted for more than 6 months and is not explained by another identified helminthic infection should trigger Strongyloides serology.
However, eosinophilia is unreliable precisely when the stakes are highest. In hyperinfection syndrome, eosinophil counts are often paradoxically normal or low. Corticosteroids — the most common precipitant of hyperinfection — directly cause eosinopenia by redistributing eosinophils from the bloodstream and suppressing eosinophil production. The immune system is overwhelmed and can no longer recruit eosinophils effectively. A patient presenting with hyperinfection may have an eosinophil count of 50 cells/μL, no peripheral eosinophilia, and negative routine differential — yet be dying from disseminated Strongyloides.
A clinician who waits for eosinophilia before testing for Strongyloides in an immunosuppressed patient will miss cases at the most dangerous moment. The teaching point is absolute: eosinophilia supports the diagnosis but its absence does not exclude it. In the immunocompromised patient with fever, diffuse abdominal pain, pulmonary infiltrates, and gram-negative bacteremia (the classic hyperinfection presentation), Strongyloides must be on the differential regardless of eosinophil count. When in doubt, treat empirically with ivermectin while diagnostic workup proceeds — the drug is safe, effective, and inexpensive, and withholding it while waiting for confirmatory testing has cost lives.
Pre-Immunosuppression Screening Algorithm
The 2016 guidelines from the Infectious Diseases Society of America (IDSA) and American Society of Tropical Medicine and Hygiene (ASTMH) are explicit: screen for Strongyloides before initiating any immunosuppression in patients who have lived in or had extended travel to endemic regions. This recommendation exists because the window between initiating immunosuppression and hyperinfection can be as short as two to four weeks, and because hyperinfection has a mortality rate exceeding 80% once established.
The preferred screening test is IgG ELISA for immunocompetent patients. If positive: treat with ivermectin 200 mcg/kg/day for 2 days (single course for uncomplicated infection), then confirm cure with repeat serology at 6 months. A falling titer indicates treatment success; a stable or rising titer suggests treatment failure and should prompt re-treatment followed by stool cultures. If initially seronegative but immunosuppression is clinically urgent and epidemiologic risk is high: treat empirically with ivermectin (single course) before initiating immunosuppression, then confirm with serology at 6 months. This empirical approach is standard of care for high-risk patients where waiting for test results would delay necessary treatment of the primary condition.
For patients already immunocompromised (and therefore potentially seronegative despite active infection): combine serology with agar plate culture of three stool samples on consecutive days. If both are negative and clinical suspicion remains high, proceed to duodenal aspiration. Do not rely on a single test. When immunosuppression cannot be delayed (e.g., acute organ rejection), treat empirically with ivermectin and test simultaneously.
Endemic regions requiring screening include all of sub-Saharan Africa, Southeast Asia, South Asia (India, Bangladesh, Sri Lanka, Nepal), tropical Latin America (all of Central America, the Amazon basin, the Andes foothills, the Caribbean), Pacific Islands, and rural communities in the southern United States — particularly Puerto Rico, the US Virgin Islands, and historically in Appalachia and the Mississippi Delta. Country of origin trumps time since immigration: Strongyloides infection persists for decades without treatment due to the autoinfection cycle, and immigrants from endemic regions who arrived in the United States 30 or 40 years ago may still carry active infection. A Vietnam veteran now receiving chemotherapy for lymphoma is at risk.
The algorithm should be embedded into pre-immunosuppression checklists at any institution serving patients from these backgrounds. Rheumatologists initiating biologics, oncologists starting chemotherapy, transplant centers evaluating solid organ transplant candidates, and infectious disease physicians starting corticosteroids for autoimmune conditions should all have access to this screening pathway. The cost of an ELISA (approximately $25–50 US dollars) and a two-day ivermectin course (approximately $5–15 US dollars in generic form) is negligible compared with the ICU cost of managing hyperinfection — and the human cost of a preventable death.
Key Research Papers
- Keiser PB, Nutman TB. Strongyloides stercoralis in the Immunocompromised Population. Clin Microbiol Rev. Search PubMed [PubMed PMID 21208913]
- Marcos LA et al. Disseminated Strongyloidiasis. Am J Trop Med Hyg. Search PubMed [PubMed PMID 17238140]
- Henriquez-Camacho C et al. Ivermectin vs. albendazole for Strongyloides. Cochrane Database Syst Rev. Search PubMed [PubMed PMID 22715901]
- Requena-Mendez A et al. Evidence-based guidelines for Strongyloides management. PLoS Negl Trop Dis. Search PubMed [PubMed PMID 26063631]
- Greaves D et al. Strongyloides stercoralis: the forgotten killer. Trans R Soc Trop Med Hyg. Search PubMed [PubMed PMID 25310989]
- Lam CS et al. Disseminated strongyloidiasis: a retrospective study. J Infect. Search PubMed [PubMed PMID 23536768]
- Boulware DR et al. Hyperinfection strongyloidiasis with HTLV-1. Am J Trop Med Hyg. Search PubMed [PubMed PMID 27174396]
- Bisoffi Z et al. Strongyloides stercoralis: a plea for action. PLoS Negl Trop Dis. Search PubMed [PubMed PMID 28895697]
- Nutman TB. Human infection with Strongyloides stercoralis. Parasitology. Search PubMed [PubMed PMID 26580609]
- Roxby AC et al. Strongyloidiasis in transplant patients. Clin Infect Dis. Search PubMed [PubMed PMID 22046048]
PubMed Searches
- Strongyloides diagnosis serology
- Strongyloides agar plate culture
- Strongyloides ELISA sensitivity specificity
- Strongyloidiasis screening before immunosuppression
- Strongyloides eosinophilia diagnosis
Connections
- Strongyloides Overview
- Hyperinfection and Disseminated Strongyloidiasis
- Larva Currens and Skin Symptoms
- Ivermectin Treatment
- Prevention and Screening
- All Parasites
- Hookworm