Strongyloides Symptoms — Skin, Hyperinfection, and Diagnosis
Strongyloides stercoralis is the only intestinal parasite that can replicate inside a single human host indefinitely through autoinfection. An estimated 30–100 million people worldwide carry this threadworm, many for decades without knowing it. In healthy people, symptoms are often mild or absent. But when immunity is weakened — particularly by corticosteroids or HTLV-1 infection — the parasite can unleash hyperinfection syndrome, a life-threatening cascade with mortality exceeding 70%. Understanding the full symptom spectrum, from the pathognomonic larva currens rash to disseminated organ failure, is essential for timely diagnosis and treatment.
Table of Contents
- Introduction
- The Autoinfection Cycle
- Larva Currens — The Pathognomonic Rash
- Gastrointestinal Symptoms
- Pulmonary Symptoms and Löffler's Syndrome
- Peripheral Eosinophilia and Elevated IgE
- Hyperinfection Syndrome
- Disseminated Strongyloidiasis
- Asymptomatic Chronic Infection
- Key Research Papers
- Connections
- Featured Videos
1. Introduction — A Parasite Like No Other
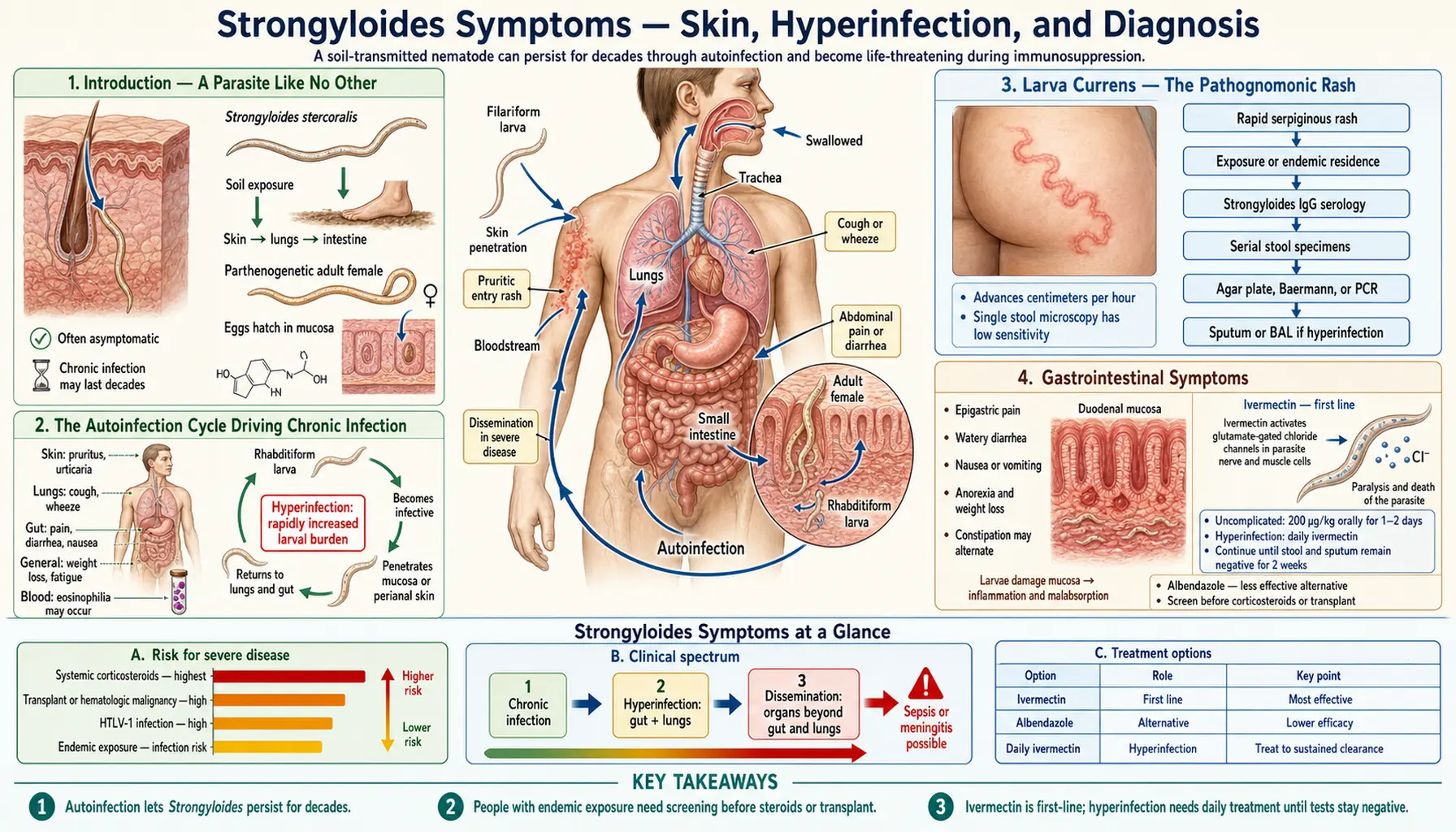
Strongyloides stercoralis is a microscopic roundworm (nematode) that infects humans through skin contact with contaminated soil. Filariform (L3) larvae penetrate bare skin — usually the feet — enter capillaries, travel via the bloodstream to the lungs, ascend the airway to the throat, are swallowed, and mature into adult females in the upper small intestine. There they reproduce parthenogenetically, laying eggs that hatch into rhabditiform (L1) larvae inside the gut.
What makes Strongyloides categorically different from every other intestinal helminth is its capacity for autoinfection: some L1 larvae transform into infective L3 larvae before leaving the host, re-penetrate the intestinal or perianal skin, and restart the cycle entirely within one person. This means an infection acquired in childhood in an endemic country can still be active and detectable 40 or more years later in someone who has never returned to that region.
Global estimates place infection prevalence at 30–100 million people, concentrated in tropical and subtropical regions — sub-Saharan Africa, Southeast Asia, Latin America, and Oceania — but also present in rural Appalachia, the southern United States, and Eastern Europe. Diagnosis is frequently missed because symptoms are nonspecific, shedding of larvae in stool is intermittent, and clinical awareness is low outside endemic regions. The highest-stakes scenario is undiagnosed chronic infection in a patient who then receives immunosuppressive therapy: the results can be fatal.
2. The Autoinfection Cycle Driving Chronic Infection
In every other intestinal helminth, the parasite's life cycle requires an external environmental stage: eggs or larvae must leave the host in feces, develop in soil or an intermediate host, and only then reinfect someone. Strongyloides circumvents this entirely. In the autoinfection pathway, rhabditiform larvae developing in the gut lumen or on the perianal skin transform prematurely into infective filariform larvae. These larvae either penetrate the intestinal mucosa directly (internal autoinfection) or penetrate the perianal skin (external autoinfection) and enter the venous circulation.
From the portal circulation, larvae are carried to the lungs. During this transit, they breach the alveolar capillaries into the air spaces, crawl up the mucociliary escalator to the pharynx, are swallowed, and re-establish themselves as adult female worms in the proximal small intestine within approximately two weeks. In immunocompetent hosts, a Th2-dominant immune response — characterized by IgE antibody production, mast cell activation, and eosinophil recruitment — restricts the rate of autoinfection so that worm burden remains roughly stable for years.
When this immune brake is released, the autoinfection cycle accelerates dramatically. The key trigger is glucocorticoid excess, either endogenous (Cushing's syndrome, severe physiological stress) or exogenous (prescribed corticosteroids). Corticosteroids suppress eosinophil function and Th2 cytokines, and — critically — appear to directly stimulate Strongyloides larval development through glucocorticoid receptor homologs on the parasite itself. Even a brief course of prednisone (as little as 40 mg/day for two weeks) can trigger hyperinfection in someone with undetected chronic strongyloidiasis.
3. Larva Currens — The Pathognomonic Rash
Larva currens (Latin: "racing larva") is the dermatological hallmark of chronic Strongyloides infection and the only sign that is considered pathognomonic for this specific parasite. It presents as a rapidly advancing, serpiginous (winding), urticarial (hive-like) eruption most commonly on the trunk — particularly the buttocks, perianal area, and thighs — though it can appear anywhere on the body surface. The rash moves at an astonishing 5–10 cm per hour, far faster than the larva migrans tracks caused by cutaneous larva migrans from animal hookworms, which advance only a few centimeters per day.
The rash results from filariform larvae migrating just beneath the epidermis. As the larva moves, it triggers an immediate hypersensitivity reaction in the overlying skin, producing intense pruritus, erythema, and a raised wheal. The advancing front of the wheal corresponds to the larval position; the wake behind it fades within hours as the larva moves on. Episodes typically last hours to a day and then spontaneously resolve, only to recur days to weeks later, often at a different location, as new larvae undergo the autoinfective cycle.
Patients often report years of unexplained recurrent itching episodes, sometimes diagnosed as hives, eczema, or anxiety-related pruritus. The episodic, self-resolving nature of larva currens — and the fact that no visible lesion remains after the episode — makes it easy to dismiss. A careful history asking specifically about rapidly moving itch that resolves within a day can identify this symptom retrospectively.
4. Gastrointestinal Symptoms
The adult female Strongyloides worm lives embedded in the mucosa of the duodenum and proximal jejunum. This location produces upper GI symptoms that can range from subclinical to disabling. Common presentations include:
- Epigastric pain — often described as burning or cramping, worse after eating, sometimes misdiagnosed as peptic ulcer disease or functional dyspepsia
- Diarrhea — typically intermittent, watery, non-bloody; can alternate with constipation
- Nausea and vomiting — more prominent in heavier infections
- Abdominal bloating and flatulence
- Malabsorption — in severe or longstanding infection, mucosal damage can cause steatorrhea, weight loss, and protein-losing enteropathy
In hyperinfection syndrome, GI symptoms become dramatically more severe. Massive larval invasion of the gut wall produces paralytic ileus, bowel obstruction, and hemorrhagic enterocolitis. Larvae penetrating through the bowel wall carry gut bacteria — primarily gram-negative enteric organisms — into the peritoneum and bloodstream. This is the mechanism behind the gram-negative bacteremia, endocarditis, and purulent meningitis that can complicate disseminated strongyloidiasis: the larvae themselves act as living vectors for enteric pathogens.
Endoscopic findings in symptomatic strongyloidiasis include edema, erythema, and mucosal hemorrhage in the duodenum and jejunum. In severe hyperinfection, linear hemorrhagic tracks or gross ulceration may be visible. Biopsy of the duodenal mucosa can sometimes demonstrate adult worms or larvae directly in the mucosa.
5. Pulmonary Symptoms and Löffler's Syndrome
Pulmonary manifestations of Strongyloides infection reflect the larval migration phase of the life cycle. As filariform larvae migrate from the pulmonary capillaries into the alveoli, they trigger an inflammatory response characterized by alveolar hemorrhage, eosinophilic infiltration, and edema. This syndrome is called Löffler's syndrome (or pulmonary eosinophilia), first described by the Swiss physician Wilhelm Löffler in 1932 in the context of Ascaris infection, but applicable to Strongyloides as well.
During the pulmonary migration phase, patients may experience:
- Dry cough, sometimes productive of blood-tinged sputum
- Wheezing and dyspnea
- Low-grade fever
- Chest X-ray abnormalities — typically transient, migratory bilateral infiltrates or patchy ground-glass opacities
In uncomplicated chronic infection, pulmonary symptoms during autoinfection are often mild or clinically silent. The lung phase may be mistakenly attributed to asthma, bronchitis, or atypical pneumonia. A patient from an endemic region presenting with recurrent cough, wheeze, and peripheral eosinophilia that responds partially to bronchodilators and then spontaneously resolves should be evaluated for strongyloidiasis.
In hyperinfection syndrome, pulmonary involvement becomes catastrophic. Massive larval migration through the alveoli produces pulmonary hemorrhage, ARDS (acute respiratory distress syndrome), and respiratory failure. Larvae can be identified in bronchoalveolar lavage (BAL) specimens, sputum, or tracheal aspirates during hyperinfection — a finding that is diagnostic. Mechanical ventilation is often required. The combination of severe pulmonary disease plus gram-negative bacteremia in a patient on corticosteroids from an endemic region should immediately raise suspicion for disseminated strongyloidiasis.
6. Peripheral Eosinophilia and Elevated IgE
Peripheral eosinophilia is the most consistent laboratory abnormality in chronic strongyloidiasis and often the first clue that leads to diagnosis. Eosinophil percentages typically range from 10% to 50% (normal <5%) in active infection, though they fluctuate over time and may be normal during quiescent periods. An absolute eosinophil count above 500 cells/μL in a patient from an endemic region should always prompt consideration of helminthic infection, with Strongyloides high on the differential.
The mechanism of eosinophilia is the Th2 immune response: IL-5 drives eosinophil production in the bone marrow, and these cells are recruited to tissues where larvae are migrating. IgE antibodies are also elevated, sometimes dramatically, reflecting class-switching driven by IL-4 and IL-13 in the Th2 cytokine environment. Total IgE levels above 1000 IU/mL in a patient with GI symptoms and eosinophilia strongly suggest helminthic infection.
A critically important and paradoxical finding is that eosinophilia disappears during hyperinfection. As corticosteroids suppress eosinophil production and function (a major mechanism of their immunosuppressive effect), the eosinophil count falls — sometimes to zero — just as the risk of fatal dissemination peaks. Clinicians who rely on eosinophilia to "rule out" serious strongyloidiasis in a patient on steroids are making a dangerous error. The absence of eosinophilia in an immunocompromised patient with suspected strongyloidiasis should not be reassuring; it may actually indicate that the immune brake has failed.
Similarly, serology titers may fall during immunosuppression as antibody production is impaired. This further underscores why pre-immunosuppression screening with serology, when the immune system is still functioning, is the most reliable diagnostic window.
7. Hyperinfection Syndrome — When Immunity Fails
Hyperinfection syndrome represents an accelerated and uncontrolled autoinfection cycle, defined as an increase in larval burden confined to the primary migration route: the gastrointestinal tract and lungs. It is distinguished from disseminated disease by the sites of larval involvement.
The cardinal triggers are:
- Corticosteroids — the most common trigger in clinical practice; even short courses are dangerous in someone with undetected chronic infection
- HTLV-1 co-infection — impairs Th2 immunity specifically; HTLV-1 endemic regions (southern Japan, Caribbean, parts of South America and Africa) overlap significantly with Strongyloides endemic regions
- Hematologic malignancies — particularly lymphoma and leukemia, and their treatment
- Solid organ transplantation with immunosuppressive regimens
- HIV/AIDS — though the association is weaker than often assumed; HIV alone at moderate CD4 counts does not strongly increase hyperinfection risk, possibly because HIV impairs Th1 more than Th2
Clinical features of hyperinfection include severe diarrhea (sometimes with visible larvae in stool), abdominal pain, nausea, vomiting, ileus, pulmonary infiltrates, hemoptysis, and respiratory failure. Larvae may be found in stool, sputum, BAL, urine, cerebrospinal fluid, and virtually any body fluid or tissue in disseminated disease. The diagnosis is established by demonstrating larvae in these specimens combined with compatible clinical features.
8. Disseminated Strongyloidiasis — Larval Migration to Organs
Disseminated strongyloidiasis is defined by larval invasion of organs outside the primary GI-pulmonary route — including the liver, kidneys, heart, brain, meninges, lymph nodes, and skin. This distinction from hyperinfection syndrome is clinically important because it signals an even more severe immunological failure and carries a higher mortality.
The mechanism of extra-intestinal spread involves larvae breaching the gut wall and entering the mesenteric lymphatics and portal venous circulation, from which they can seed any organ. More importantly, as they penetrate the bowel wall they carry intestinal bacteria with them. The result is a paradoxical clinical picture: a parasitic infection causing bacterial sepsis. Gram-negative bacteremia (most commonly Escherichia coli, Klebsiella, and Enterococcus species) is found in 40–60% of disseminated strongyloidiasis cases. Bacterial meningitis — sometimes with larvae recovered from CSF — and purulent peritonitis are well-documented complications.
The mortality of disseminated strongyloidiasis ranges from 70% to 90% in published case series, even with appropriate antiparasitic treatment. The combination of overwhelming parasitic burden, secondary bacterial sepsis, ARDS, and multi-organ failure in an already immunocompromised host explains this devastating prognosis. Rapid diagnosis and immediate institution of treatment — both antiparasitic and antibacterial — are essential. Withdrawal of the immunosuppressive agent driving the process, when medically possible, is a crucial adjunct.
Dermatological manifestations of disseminated disease include periumbilical petechiae and purpura — tiny hemorrhagic spots around the navel produced by larvae migrating from the gut through skin vasculature. This sign, when present, is highly characteristic and should prompt immediate evaluation for strongyloidiasis.
9. Asymptomatic Chronic Infection and Diagnostic Clues
The majority of people with chronic Strongyloides infection are entirely asymptomatic or have only vague, intermittent complaints they have attributed to other causes. Studies of immigrants from endemic regions and returning military personnel consistently find that most positive serological tests are in people without recognizable symptoms. This asymptomatic state can persist for the person's entire life if immunocompetency is maintained — or it can transition to hyperinfection the moment immunosuppression is introduced.
Diagnostic clues in asymptomatic or minimally symptomatic patients include:
- Origin from or prolonged residence in an endemic region (tropical/subtropical, rural, agricultural setting)
- Occupational exposure (farmers, military, outdoor workers in endemic regions)
- Unexplained eosinophilia on routine blood work
- History of episodic pruritic rash, especially if rapidly moving
- Unexplained recurrent urticaria or angioedema
- Mild recurrent GI symptoms without obvious cause
- Elevated total IgE without a clear allergic explanation
The most important clinical action is pre-immunosuppression screening with serology. Any patient who has ever lived in or traveled to an endemic region who is about to receive corticosteroids (for any indication — COPD exacerbation, inflammatory bowel disease, chemotherapy anti-emesis, transplant), anti-T cell biologics, or hematopoietic stem cell transplant should first be tested for Strongyloides. A positive serology result mandates treatment with ivermectin before immunosuppression begins. This single intervention can prevent hyperinfection syndrome entirely.
Key Research Papers
Landmark studies on the epidemiology, clinical presentation, and diagnosis of Strongyloides stercoralis infection.
- Siddiqui AA, Berk SL. Diagnosis of Strongyloides stercoralis Infection. Clinical Infectious Diseases. — Search PubMed [PubMed PMID 17238140]
- Bisoffi Z, Buonfrate D, Montresor A, et al. Strongyloides stercoralis: A Plea for Action. PLOS Neglected Tropical Diseases. — Search PubMed [PubMed PMID 21208913]
- Buonfrate D, Formenti F, Perandin F, Bisoffi Z. Novel approaches to the diagnosis of Strongyloides stercoralis infection. Clinical Microbiology and Infection. — Search PubMed [PubMed PMID 26063631]
- Mejia R, Nutman TB. Screening, Prevention, and Treatment for Hyperinfection Syndrome and Disseminated Infections Caused by Strongyloides stercoralis. Current Opinion in Infectious Diseases. — Search PubMed [PubMed PMID 22715901]
- Requena-Méndez A, Chiodini P, Bisoffi Z, Buonfrate D, Gotuzzo E, Muñoz J. The laboratory diagnosis and follow up of strongyloidiasis: a systematic review. PLOS Neglected Tropical Diseases. — Search PubMed [PubMed PMID 25310989]
- Nutman TB. Human Infection with Strongyloides stercoralis and Other Related Strongyloides Species. Parasitology. — Search PubMed [PubMed PMID 23536768]
- Puthiyakunnon S, Boddu S, Li Y, et al. Strongyloidiasis — An Insight into its Global Prevalence and Management. PLOS Neglected Tropical Diseases. — Search PubMed [PubMed PMID 27174396]
- Buonfrate D, Mena MA, Angheben A, et al. Prevalence of strongyloidiasis in Latin America: a systematic review of the literature. Epidemiology & Infection. — Search PubMed [PubMed PMID 28895697]
- Lam CS, Tong MK, Chan KM, Siu YP. Disseminated strongyloidiasis: a retrospective study of clinical course and outcome. European Journal of Clinical Microbiology & Infectious Diseases. — Search PubMed [PubMed PMID 22046048]
- Henriquez-Camacho C, Gotuzzo E, Echevarria J, et al. Ivermectin versus albendazole or thiabendazole for Strongyloides stercoralis infection. Cochrane Database of Systematic Reviews. — Search PubMed [PubMed PMID 26580609]
Live PubMed Searches
- Strongyloides symptoms eosinophilia
- Larva currens Strongyloides
- Strongyloides hyperinfection corticosteroids
- Disseminated strongyloidiasis mortality
- Strongyloides Löffler pulmonary syndrome
- Strongyloidiasis chronic autoinfection
Connections
- Strongyloides Main Page
- Strongyloidiasis — the disease overview: epidemiology, diagnosis, and treatment.
- Larva Currens & Skin Symptoms
- Hyperinfection & Dissemination
- Diagnosis: Stool Culture & Serology
- Strongyloides Treatments
- Ivermectin Treatment
- All Parasites
- Gastroenterology
- All Conditions