Strongyloidiasis
- Overview
- Life Cycle and Autoinfection
- Epidemiology
- Transmission and Risk Factors
- Clinical Manifestations
- Hyperinfection Syndrome
- Disseminated Strongyloidiasis
- Diagnosis
- Treatment
- Prevention and Screening
- References
- Connections
1. Overview
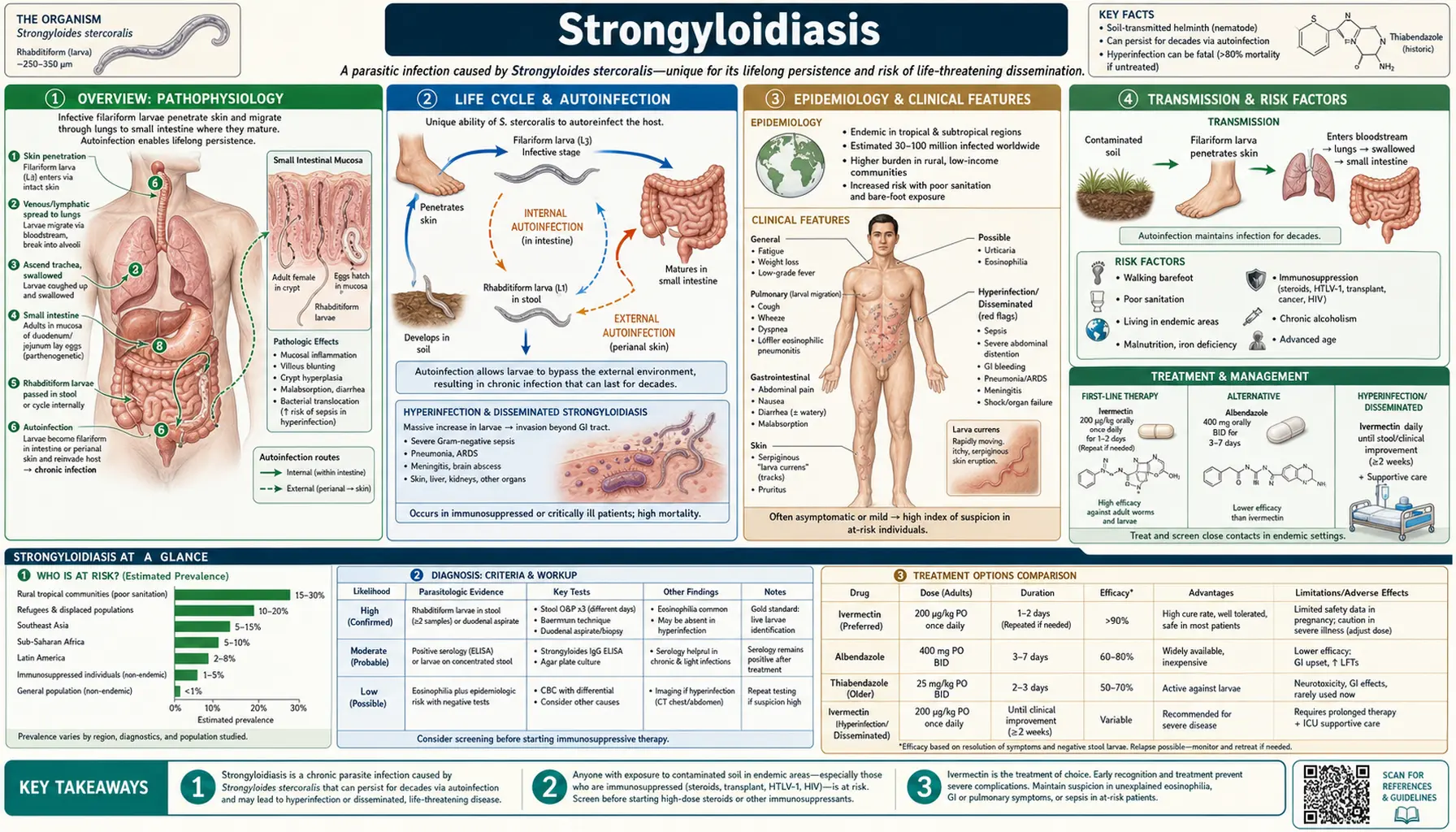
Strongyloidiasis is a chronic intestinal infection caused by Strongyloides stercoralis, a soil-transmitted roundworm (nematode) and the only human helminth capable of completing its entire life cycle within a single host through a process called autoinfection. This unique biological trait allows the parasite to persist for decades — sometimes for the remainder of a person's life — without any re-exposure to contaminated soil.
While most infected individuals carry a low parasite burden and experience only mild or no symptoms, Strongyloides harbors lethal potential in anyone who becomes immunocompromised. Corticosteroid therapy — even a single high-dose course — can trigger hyperinfection syndrome, in which massive amplification of the autoinfective cycle overwhelms the intestinal barrier, seeds gram-negative bacteria into the bloodstream, and causes sepsis, meningitis, and death. Recognizing and screening at-risk patients before immunosuppression is one of the most actionable interventions in travel medicine and transplant infectious disease.
An estimated 100 to 370 million people are infected worldwide, making strongyloidiasis one of the most globally prevalent helminth infections despite its relative obscurity in high-income country medicine. Effective oral therapy with ivermectin is available and curative in most cases.
2. Life Cycle and Autoinfection
The Strongyloides stercoralis life cycle is more complex than that of most intestinal helminths, with both free-living and parasitic phases and the critical capacity for autoinfection.
Skin penetration (infection): Infective filariform (third-stage, L3) larvae live in contaminated soil. When bare skin contacts the soil, L3 larvae penetrate — typically through the soles of the feet or any area of thin, moist skin. They enter cutaneous capillaries, migrate via the venous circulation to the lungs, break through alveolar capillaries into the alveolar space, ascend the bronchial tree to the trachea, are swallowed, and reach the small intestine. In the duodenum and jejunum, larvae mature into parthenogenetic females that burrow into the intestinal mucosa and produce eggs by asexual reproduction without requiring male worms.
Rhabditiform larvae in the gut: Eggs hatch rapidly — often before leaving the intestine — releasing first-stage (rhabditiform, L1) larvae. Most are passed in stool into the environment, where they either develop into infective L3 larvae (direct cycle) or establish a free-living generation of males and females in the soil that subsequently produce infective L3 larvae (indirect cycle).
Autoinfection — the defining trait: Some rhabditiform L1 larvae transform into infective filariform L3 larvae before leaving the host. These L3 larvae can then:
- Internal autoinfection: Penetrate the intestinal mucosa directly in the small intestine or colon, enter the portal circulation, and complete a truncated migration cycle back to the intestinal mucosa, maintaining the adult worm population indefinitely.
- External autoinfection: L3 larvae deposited in perianal skin penetrate the skin at that site, re-enter circulation, and complete the same cycle. This explains the pathognomonic skin finding larva currens — the rapidly migrating perianal/trunk rash.
Under normal immune control (primarily Th2 responses and IgE production), the level of autoinfection is kept low. Immunosuppression, particularly of the Th2 axis by corticosteroids, removes this brake and allows explosive amplification of the autoinfective cycle — the mechanism behind hyperinfection syndrome.
3. Epidemiology
Strongyloidiasis affects an estimated 100 to 370 million people worldwide, with wide uncertainty reflecting the difficulty of diagnosis — the infection is chronically underdiagnosed because standard stool ova-and-parasite examinations miss it in most cases.
Global distribution: The parasite is endemic throughout the tropics and subtropics: sub-Saharan Africa, Southeast Asia, South Asia, Latin America, the Caribbean, and parts of the Pacific. Endemic foci also exist in temperate regions: the Appalachian region of the United States (Kentucky, Tennessee, West Virginia), parts of the rural South, Eastern Europe (including the Balkans and rural Romania), and some Mediterranean areas.
High-risk populations:
- Immigrants from endemic countries — often carry asymptomatic infections for decades after leaving endemic areas. Studies of Southeast Asian and Latin American refugees in the United States show seroprevalence rates of 10–40%.
- Military veterans — United States veterans who served in Vietnam, Korea, the Pacific, and the Caribbean have disproportionately high prevalence. Some Vietnam veterans have been diagnosed with strongyloidiasis 50+ years after service.
- Travelers — short-term travelers to endemic regions can acquire infection, particularly those doing outdoor activities with soil exposure.
- HTLV-1 co-infection — Human T-cell lymphotropic virus type 1 (HTLV-1), itself endemic in southern Japan, the Caribbean, and sub-Saharan Africa, dramatically impairs the Th2 immune response required to control Strongyloides, increasing both infection prevalence and risk of hyperinfection syndrome independent of corticosteroid use.
- Rural poor — in endemic areas, lack of shoes, open-pit latrines, and wastewater reuse in agriculture sustain soil contamination. Children are frequently infected through play on contaminated soil.
4. Transmission and Risk Factors
Primary route — skin contact with contaminated soil: Direct skin penetration by filariform L3 larvae in soil contaminated with human feces is the overwhelmingly dominant mode of acquisition. Wearing shoes is protective; the barefoot habit is the single largest behavioral risk factor in endemic areas. Activities such as gardening, farming, and sitting on bare ground also confer risk.
Fecal–oral transmission can occur but is uncommon because eggs are rarely found in stool (larvae hatch rapidly); it has been documented in institutional settings with poor hygiene.
Person-to-person transmission is possible in institutional settings (nursing homes, psychiatric facilities) where hygiene is poor, though this is uncommon compared to soil transmission.
Immunosuppression risk factors for hyperinfection — any condition or therapy that impairs the Th2 immune response can trigger life-threatening hyperinfection in a chronically infected person:
- Corticosteroids — the most important iatrogenic trigger; even a single high-dose course (e.g., for a COPD exacerbation or spinal cord injury) has precipitated fatal hyperinfection in patients with unrecognized chronic strongyloidiasis.
- Solid organ transplantation and post-transplant immunosuppression (tacrolimus, mycophenolate)
- Hematologic malignancies (lymphoma, leukemia)
- HTLV-1 infection (independent of HIV)
- HIV/AIDS (less strongly associated than HTLV-1, but still a risk with advanced immunosuppression)
- Malnutrition, alcoholism
5. Clinical Manifestations
The clinical spectrum of strongyloidiasis spans from completely asymptomatic chronic infection (the most common presentation) to rapidly fatal hyperinfection syndrome, depending primarily on the host's immune status.
Acute infection: At the time of initial skin penetration, a localized pruritic maculopapular or vesicular rash ("ground itch") may develop at the entry site, typically on the feet. During larval migration through the lungs (Löffler-like syndrome), transient dry cough, wheezing, and pulmonary infiltrates on chest X-ray can occur, accompanied by peripheral eosinophilia. These early symptoms are usually mild and self-limited, and most individuals do not seek medical attention.
Chronic asymptomatic infection: The most common scenario globally. Patients carry low parasite burdens for years to decades with no symptoms. The only clue may be incidental peripheral blood eosinophilia (50–80% of infected individuals), which should always prompt evaluation for helminth infection in patients from endemic areas.
Chronic symptomatic infection — gastrointestinal: Intermittent abdominal pain (often epigastric, mimicking peptic ulcer disease or irritable bowel), bloating, nausea, and alternating diarrhea and constipation. Heavy infections can cause malabsorption, protein-losing enteropathy, and weight loss.
Larva currens — the pathognomonic skin finding of chronic strongyloidiasis. Filariform L3 larvae generated by external autoinfection migrate rapidly through the dermis, producing a linear, serpiginous, urticarial rash that advances at up to 10 cm per hour — far faster than any other migratory larva. It characteristically tracks along the trunk, buttocks, and perianal skin following the pattern of larval migration. Individual tracks last hours to days, then resolve, only to recur. The speed of migration (unlike the slower cutaneous larva migrans caused by dog/cat hookworms) is specific enough to make it a clinical diagnostic clue.
Peripheral eosinophilia: Present in 50–80% of infected individuals. It may be the only laboratory abnormality in asymptomatic chronic cases. When eosinophilia is found in a patient from an endemic area, strongyloidiasis should be near the top of the differential — even if the patient has been in a non-endemic country for decades.
6. Hyperinfection Syndrome
Hyperinfection syndrome is the most feared complication of strongyloidiasis and carries a mortality rate of 15–87% depending on the setting, severity, and speed of diagnosis. It occurs when the normal immune brake on autoinfection is removed, allowing massive amplification of the larval burden within the host.
Mechanism: In a chronically infected, immunocompetent host, the Th2-driven immune response (IgE, mast cells, eosinophils) limits the number of larvae completing each autoinfective cycle. Corticosteroids directly suppress Th2 responses and increase corticosteroid receptor signaling in Strongyloides larvae, which accelerates larval development from rhabditiform to filariform stages. The result is an exponential increase in the number of larvae penetrating the gut wall and migrating throughout the body.
The corticosteroid danger: This is not a theoretical risk. Fatal hyperinfection has been reported after short courses of oral or parenteral corticosteroids given for conditions as common as asthma exacerbations, COPD flares, spinal cord injury, and organ rejection prophylaxis — in patients who had no idea they carried Strongyloides. The corticosteroid dose required to trigger hyperinfection is not well defined; there is no clearly safe threshold.
Clinical features of hyperinfection:
- Severe gastrointestinal disease: Profuse watery or bloody diarrhea, nausea, vomiting, abdominal pain, ileus. Larvae in massive numbers disrupt the intestinal mucosa, causing protein-losing enteropathy and ulceration.
- Pulmonary involvement: Large numbers of larvae migrating through the lungs cause hemorrhagic pneumonitis — cough, hemoptysis, dyspnea, diffuse bilateral alveolar infiltrates on chest imaging. Larvae can be found in BAL (bronchoalveolar lavage) fluid — a diagnostic finding.
- Gram-negative bacteremia and sepsis: Migrating larvae carry intestinal bacteria (especially E. coli, Klebsiella, Enterococcus) through the disrupted intestinal wall into the bloodstream and meninges. Recurrent gram-negative bacteremia or gram-negative meningitis in an immunosuppressed patient from an endemic area should immediately trigger testing for hyperinfection. Empiric antibiotics alone, without treating the underlying Strongyloides, are ineffective — the bacteria keep seeding through the gut wall as long as larvae continue migrating.
- Central nervous system: Bacterial meningitis (gram-negative organisms carried by larvae to the meninges) and, rarely, direct larval infiltration of the CNS (eosinophilic meningitis).
The pre-immunosuppression screening imperative: Any patient from an endemic area (including immigrants, refugees, and veterans) who is about to receive corticosteroids, organ transplant immunosuppression, or chemotherapy for hematologic malignancy should be screened for Strongyloides with serology (ELISA) and treated with ivermectin before immunosuppression begins. This simple precaution prevents a potentially fatal complication.
7. Disseminated Strongyloidiasis
Disseminated strongyloidiasis is distinguished from hyperinfection syndrome by the spread of larvae beyond the gastrointestinal tract and lungs to organs not normally traversed by Strongyloides in its standard migration: the liver, heart, kidneys, central nervous system, skin (widespread), and virtually any organ. It is defined as larvae identified in a site outside the normal gut-lung migration pathway.
Disseminated disease carries the highest mortality of any form of strongyloidiasis — reported rates exceed 80–90% in some series, especially when diagnosis is delayed or made only at autopsy. Clinical findings include hepatomegaly with abnormal liver function tests, myocarditis, renal involvement, and widespread skin manifestations beyond the typical larva currens pattern.
Diagnosis of disseminated strongyloidiasis often requires high clinical suspicion. Larvae have been found in urine, cerebrospinal fluid, bronchoalveolar lavage fluid, peritoneal fluid, skin biopsies, liver biopsies, and at autopsy in virtually every organ. Finding larvae in an unusual body fluid in an immunosuppressed patient from an endemic area should be treated as a medical emergency.
Treatment is the same as for hyperinfection — high-dose or extended-course ivermectin — but outcomes are substantially worse and supportive care for multi-organ dysfunction is required.
8. Diagnosis
Diagnosis of strongyloidiasis is challenging because standard stool examinations miss the infection in the majority of cases and no single test has both high sensitivity and high specificity. A combination of methods, guided by clinical context, is most effective.
Stool microscopy: Rhabditiform (L1) larvae — not eggs — are the diagnostic target in stool. Key morphologic distinction: rhabditiform larvae of Strongyloides have a short buccal cavity (mouth region), distinguishing them from hookworm rhabditiform larvae (long buccal cavity). Single stool examination sensitivity is only 25–30%; three or more samples improve sensitivity to approximately 60–80% for active infections. Concentration techniques (Baermann funnel, agar plate culture) significantly improve sensitivity and should be used when strongyloidiasis is suspected.
Agar plate culture: Stool is placed on nutrient agar; larvae migrate and leave bacterial tracks visible to the naked eye. Sensitivity of approximately 96% in active infections, superior to direct microscopy, but requires specialized laboratory setup and 2–3 days to complete.
Serology (ELISA for IgG): The most sensitive single test for chronic strongyloidiasis — reported sensitivity of approximately 94% for detection of anti-Strongyloides IgG. The principal limitation is cross-reactivity with other helminths (particularly Toxocara, Schistosoma, and filarial species), reducing specificity in co-endemic areas. Serology remains positive after successful treatment for months to years, limiting its utility in confirming cure; a fourfold or greater decline in titer suggests treatment success. Serology is the recommended first test for pre-immunosuppression screening.
PCR (stool or BAL): Real-time PCR targeting Strongyloides-specific sequences in stool has sensitivity comparable to or exceeding agar plate culture in research settings, with higher specificity than serology. BAL PCR is valuable in diagnosing hyperinfection syndrome in patients with pulmonary involvement. PCR is not yet universally available.
Peripheral eosinophilia: While not specific, eosinophilia (>500 eosinophils/mm³, or >5% of white cells) is present in 50–80% of cases and in the right epidemiologic context should prompt parasite serology. Notably, eosinophilia may decrease or disappear during corticosteroid therapy — its absence in an immunosuppressed patient does not exclude strongyloidiasis or hyperinfection.
In hyperinfection: Rhabditiform and filariform larvae in stool, BAL, urine, or other body fluids. Larvae may be visible on direct microscopy of BAL cytology or sputum. Blood cultures for gram-negative bacteria should accompany parasite testing.
9. Treatment
Ivermectin (first-line): Ivermectin 200 mcg/kg/day orally for 2 consecutive days is the recommended first-line treatment for uncomplicated strongyloidiasis (chronic or acute). It is significantly more effective than albendazole or the older thiabendazole. Cure rates with a 2-day course range from 83–100% in clinical trials. The drug is FDA-approved for strongyloidiasis.
Ivermectin works by binding glutamate-gated chloride channels in invertebrate nerve and muscle cells, causing hyperpolarization and paralysis of the parasite. It is generally well tolerated; the most common side effects are mild gastrointestinal upset and dizziness. It should be taken on an empty stomach (or with water only) for optimal absorption.
Albendazole (second-line): Albendazole 400 mg twice daily for 7 days is an acceptable alternative when ivermectin is unavailable or contraindicated. Cure rates are lower (approximately 45–75%) than ivermectin. Not FDA-approved for strongyloidiasis but widely used off-label internationally.
Hyperinfection syndrome treatment: Ivermectin 200 mcg/kg/day orally (or via nasogastric tube in patients unable to swallow) continued daily until two consecutive stool samples obtained 2 weeks apart are negative for larvae — typically 2–4 weeks of therapy, sometimes longer. For patients unable to absorb oral ivermectin due to severe ileus or malabsorption (a real concern in hyperinfection, as larvae disrupt intestinal absorption), subcutaneous or rectal administration has been used. Concurrent broad-spectrum antibiotics targeting gram-negative enteric organisms are essential. Corticosteroids should be tapered or stopped as rapidly as is safe for the underlying condition.
Post-treatment monitoring: Serology can remain positive for months to years after cure. Follow-up stool examination (3 stool samples, 4 weeks after treatment) and/or repeat serology with attention to titer decline is used to confirm parasitologic cure, particularly before re-initiating immunosuppression.
Thiabendazole (the original treatment) is now largely abandoned due to high rates of side effects (nausea, vomiting, dizziness, hepatotoxicity) and inferior efficacy compared to ivermectin.
10. Prevention and Screening
Personal protective measures: Wearing shoes or sandals consistently in endemic areas is the single most effective individual measure. Avoid direct skin contact with potentially contaminated soil, particularly in areas with poor sanitation. Travelers to endemic regions should be counseled about ground contact risks.
Pre-immunosuppression screening — the highest-yield intervention: All patients with epidemiologic risk (birth in or prolonged residence in an endemic country, history of military service in endemic regions, immigration from endemic areas, even decades prior) should be screened for Strongyloides before starting:
- Any corticosteroid regimen (including high-dose short courses)
- Solid organ transplantation or post-transplant immunosuppressive therapy
- Hematologic malignancy chemotherapy
- Biologic agents that impair cellular immunity
Serology (ELISA for IgG) is the preferred screening test — sensitivity ~94%, requires only a blood draw, and results can be available within days. Positive serology in an asymptomatic patient scheduled for immunosuppression should trigger treatment with ivermectin and confirmation of cure before proceeding. This low-cost intervention prevents a frequently fatal complication.
Public health measures: Safe sanitation (latrines, sewage treatment), wastewater treatment before use in agriculture, and health education about footwear and soil contact are the long-term community-level interventions. Mass drug administration (MDA) programs with ivermectin for co-endemic neglected tropical diseases (onchocerciasis, lymphatic filariasis) provide incidental benefit against Strongyloides.
11. References
- Schar F, et al. Strongyloides stercoralis: Global Distribution and Risk Factors. PLoS Negl Trop Dis. 2013;7(7):e2288. PMID: 23875033
- Buonfrate D, et al. Severe strongyloidiasis: a systematic review of case reports. BMC Infect Dis. 2013;13:78 — Search PubMed
- Marcos LA, et al. Strongyloides hyperinfection syndrome: an emerging global infectious disease. Trans R Soc Trop Med Hyg. 2008;102(4):314–318. PMID: 18321548
- Nutman TB. Human infection with Strongyloides stercoralis and other related Strongyloides species. Parasitology. 2017;144(3):263–273 — Search PubMed
- Lim S, et al. Ivermectin versus albendazole for the treatment of Strongyloides stercoralis infection: a randomized, open label trial in an endemic area. Int J Infect Dis. 2018;68:10–14 — Search PubMed
- Concha R, et al. Intestinal strongyloidiasis: recognition, management, and determinants of outcome. J Clin Gastroenterol. 2005;39(3):203–211 — Search PubMed
- Suputtamongkol Y, et al. Comparison of repeated stool examinations, agar plate culture, and a rapid ELISA for diagnosis of Strongyloides stercoralis in asymptomatic and mildly symptomatic individuals. Diagn Microbiol Infect Dis. 2014;79(3):347–350 — Search PubMed
- Greaves D, et al. Strongyloides stercoralis infection in former British Far East prisoners of war. J Infect. 2001;43(1):74–75 — Search PubMed
- Keiser PB, Nutman TB. Strongyloides stercoralis in the Immunocompromised Population. Clin Microbiol Rev. 2004;17(1):208–217. PMID: 14726461
- Vadlamudi RS, et al. Strongyloides stercoralis in patients with lymphoma, recurrent abdominal pain, or malnutrition and eosinophilia. Cancer. 2006;106(9):2016–2026 — Search PubMed
- Mejia R, Nutman TB. Screening, prevention, and treatment for hyperinfection syndrome and disseminated infections caused by Strongyloides stercoralis. Curr Opin Infect Dis. 2012;25(4):458–463 — Search PubMed
- Sarangi G, Panda S. Eosinophilic meningitis due to Strongyloides stercoralis in an immunocompromised patient: a review of mechanisms and outcomes. J Parasit Dis. 2020;44(1):1–7 — Search PubMed
Search PubMed for more research on Strongyloides stercoralis infection and treatment, strongyloidiasis hyperinfection and immunosuppression, and Strongyloides screening before corticosteroids.
12. Connections
- Chagas Disease
- Leishmaniasis
- Schistosomiasis
- Acanthamoeba Infection
- Strongyloides Symptoms — larva currens, hyperinfection, and eosinophilia in detail.
- Leptospirosis
- Brucellosis
- Bartonellosis
- Ehrlichiosis
- Zinc — Immune Function
- Vitamin A — Immune Defense
- Laboratory Tests
- Infectious Disease Index
- Hyperinfection and Dissemination — how immunosuppression turns a silent infection into a fatal one.
- Strongyloides — the parasite hub for the nematode itself: life cycle, symptoms, and treatment pages in one place.