Toxocara: Dog and Cat Roundworm That Infects Millions of Americans Silently
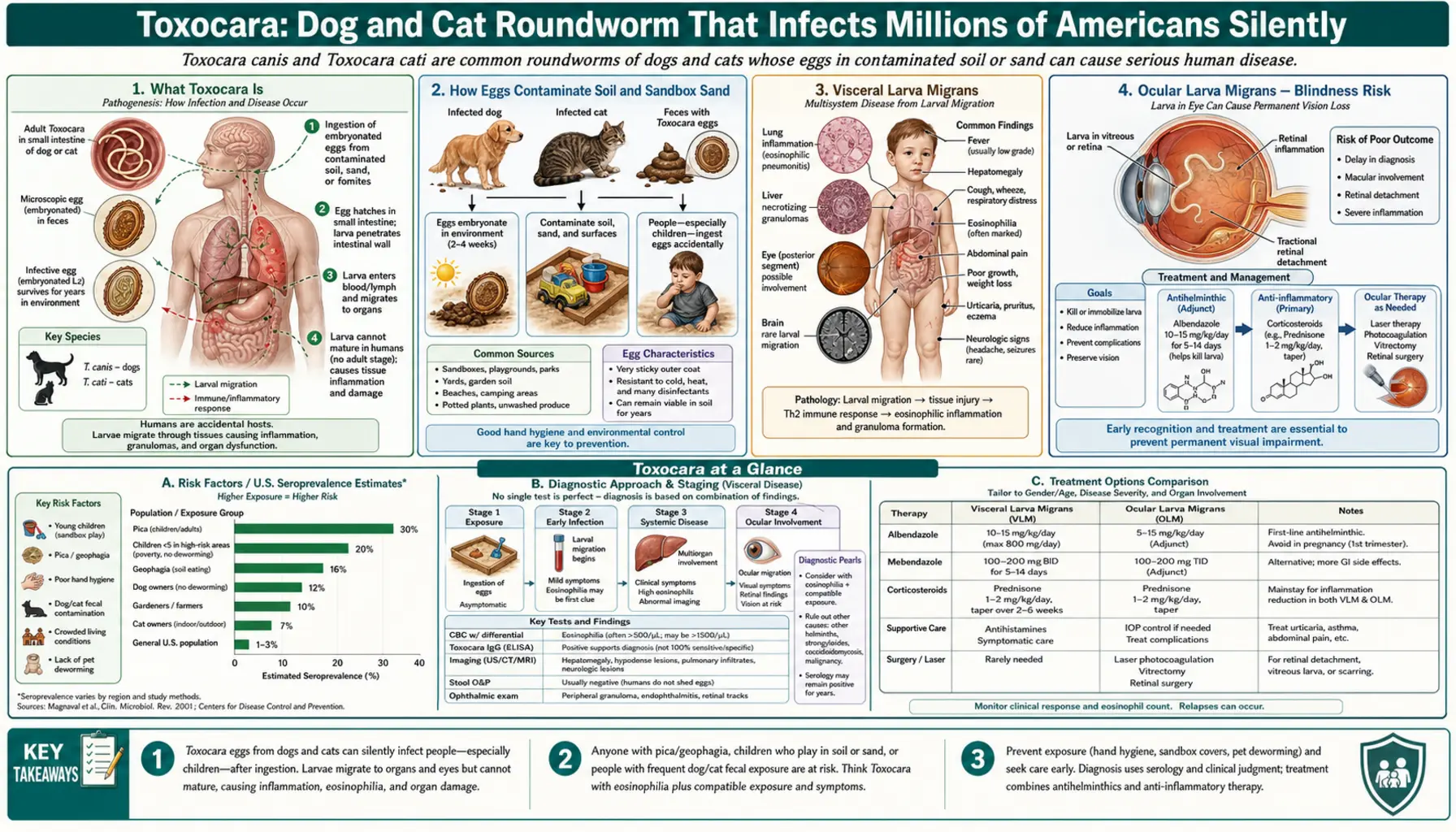
Toxocariasis is caused by Toxocara canis (dog roundworm) and T. cati (cat roundworm) — larvae that hatch from ingested eggs and migrate through human tissues. An estimated 14% of the US population has been exposed. Most infections are silent, but larvae migrating to the eye cause ocular larva migrans (with blindness risk) and to the brain cause neurological symptoms. Toxocariasis is the most common helminth infection in the United States and one of the most underrecognized.
Table of Contents
- What Toxocara Is
- How Eggs Contaminate Soil and Sandbox Sand
- Visceral Larva Migrans
- Ocular Larva Migrans — Blindness Risk
- Covert Toxocariasis
- Who Is Most at Risk
- Diagnosis
- Treatment (Albendazole)
- Prevention — Pet Deworming and Handwashing
- Key Research Papers
- Featured Videos
1. What Toxocara Is
Toxocara canis (dog roundworm) and Toxocara cati (cat roundworm) are intestinal nematodes that normally parasitize dogs and cats, respectively. Their natural life cycle involves adult worms living in the small intestine of their definitive host (dogs or cats), producing eggs shed in the animal's feces. Puppies and kittens are particularly heavily infected — nearly all puppies are born with T. canis, either through transplacental or transmammary transmission from the mother.
In their natural hosts, the larval worms complete a full life cycle, ultimately maturing into adult worms in the intestine. Humans are accidental (paratenic) hosts — we pick up embryonated eggs by ingestion, but the larvae cannot complete their development to adult worms in the human body. Instead, second-stage larvae (L2) migrate through human tissues, sometimes for months to years, causing damage by their physical migration and by triggering immune reactions.
Toxocariasis is far more common in the United States than most clinicians realize. The NHANES (National Health and Nutrition Examination Survey) found that approximately 14% of the US population has serological evidence of past Toxocara exposure, representing roughly 46 million Americans. Prevalence is highest in the southeastern United States, among African Americans, and in children living in poverty in older housing with soil contact.
2. How Eggs Contaminate Soil and Sandbox Sand
The primary route of Toxocara infection in humans is ingestion of embryonated eggs from contaminated soil, sand, or objects. After infected dogs and cats defecate in the environment, eggs are shed in feces. The eggs are not immediately infectious — they require 2–4 weeks in warm, moist soil to embryonate (develop a larva inside), after which they become highly infective.
Once embryonated, the eggs are remarkably resistant: they can survive in soil for years under appropriate conditions. Their sticky outer coat causes them to adhere to surfaces and hands. Sources of egg contamination include:
- Sandboxes and playgrounds: Children's sandboxes are particularly high-risk environments because cats use them as litter boxes and because children engage in hand-to-mouth behavior while playing. Studies have found Toxocara eggs in a high percentage of public sandbox samples in many countries.
- Parks and public green spaces: Areas used by off-leash dogs accumulate fecal contamination. Multiple surveys of urban parks have found Toxocara eggs in significant proportions of soil samples.
- Gardens: Home gardens and yards frequented by cats can accumulate eggs in soil, exposing gardeners through hand-to-soil-to-mouth contact.
- Unwashed vegetables: Raw vegetables grown in contaminated soil can carry eggs to the table if inadequately washed.
- Infected animal meat: Ingestion of raw or undercooked liver or meat from infected animals (cattle, sheep, rabbits) is an underappreciated transmission route in some populations.
3. Visceral Larva Migrans
Visceral larva migrans (VLM) is the syndrome caused by Toxocara larvae migrating through the internal organs. It is the most common clinical syndrome, particularly in young children aged 1–5 who have heavy soil exposure. After ingested eggs hatch in the small intestine, larvae penetrate the gut wall, enter the portal circulation, reach the liver, and then spread via the bloodstream to the lungs, brain, heart, eyes, and muscles.
The liver is often the primary site of damage. Larvae tunneling through hepatic tissue cause focal eosinophilic granulomas, producing hepatomegaly (enlarged liver), elevated transaminases, and abdominal pain. Pulmonary involvement causes cough, wheeze, and transient pulmonary infiltrates on chest X-ray resembling asthma or pneumonia. Systemic manifestations include prolonged fever, malaise, and the characteristic laboratory hallmark: persistent eosinophilia with very high eosinophil counts (sometimes exceeding 30–50% of the white blood cell differential).
VLM is typically self-limited in immunocompetent children, resolving over weeks to months as the larvae die and the granulomatous response subsides. Fatal cases are rare but have occurred with heavy infections, particularly when larvae invade the myocardium or brain. Neurological involvement (neurotoxocariasis) can cause seizures, encephalopathy, and behavioral changes.
4. Ocular Larva Migrans — Blindness Risk
Ocular larva migrans (OLM) is a distinct and potentially devastating syndrome that occurs when a Toxocara larva migrates into the eye. OLM typically affects older children and young adults (less commonly young children who get VLM) and usually presents as unilateral visual disturbance or decreased vision.
The larva reaches the eye via the retinal or ciliary blood vessels, lodges in the posterior segment, and triggers an intense local inflammatory (eosinophilic granulomatous) reaction as it dies. The resultant endophthalmitis (inflammation inside the eye) can damage the retina and vitreous, producing:
- Posterior pole granuloma: A white mass on the retina near the macula or optic disc, sometimes visible as a "leukocoria" (white pupil) if large
- Peripheral granuloma with retinal traction bands
- Vitritis (inflammation of the vitreous humor)
- Retinal detachment in severe cases
OLM can cause permanent unilateral blindness. It is frequently misdiagnosed as retinoblastoma (a childhood eye cancer) because both can present with leukocoria, and incorrect enucleation (eye removal) of non-cancerous eyes has resulted from this confusion. Ophthalmological evaluation by a specialist experienced with both conditions is critical when leukocoria is identified in a child. Unlike VLM, OLM typically occurs without systemic symptoms or significant eosinophilia, making the clinical picture less obvious.
5. Covert Toxocariasis
Covert toxocariasis is a term used for low-grade Toxocara infection that produces nonspecific symptoms without the classic VLM or OLM syndromes. Symptoms attributed to covert toxocariasis include chronic abdominal pain, headache, behavioral changes in children (including associations with attention problems), chronic cough, and recurrent urticaria (hives).
The relationship between seropositivity for Toxocara and these nonspecific symptoms is epidemiologically documented but the causal link is difficult to establish rigorously, since seroprevalence is high in the general population and many seropositive individuals have no symptoms at all. Research has suggested associations between Toxocara seropositivity and childhood asthma, epilepsy, and cognitive delays, but these findings remain areas of active investigation.
The concept of covert toxocariasis is clinically important because it may be responsible for a burden of chronic nonspecific illness that is currently attributed to other diagnoses — or labeled idiopathic — in children with high-risk environmental exposures.
6. Who Is Most at Risk
Risk of toxocariasis is shaped by behavioral and environmental exposures:
- Young children (ages 1–5): Hand-to-mouth behavior during outdoor play dramatically increases exposure to contaminated soil. Children with pica (compulsive ingestion of soil, clay, or non-food items) are at particularly high risk of heavy infection.
- Dog and cat owners: Particularly those with puppies or kittens, who shed the heaviest egg burdens. Dogs should receive routine deworming as puppies.
- Residents of low-income, urban communities: Environmental contamination is higher in areas with dense dog populations and inadequate waste management. African American children living in poverty in the southeastern US have the highest seroprevalence rates.
- Gardeners and farmers: Soil contact in gardens frequented by cats or dogs increases exposure.
- People who eat raw or undercooked animal liver: A less-recognized transmission route associated with VLM outbreaks in Japan linked to consumption of raw chicken or cattle liver.
7. Diagnosis
Diagnosis of toxocariasis relies primarily on clinical features combined with serology:
- Serology (ELISA for IgG antibodies to Toxocara excretory-secretory antigens): The primary diagnostic test for VLM and covert toxocariasis. Sensitivity approximately 78–90% for VLM; lower for OLM because OLM occurs at lower worm burdens, often insufficient to generate high systemic antibody titers. A positive result confirms exposure; interpretation requires clinical correlation since many exposed individuals have no active disease.
- Complete blood count with differential: Eosinophilia (elevated eosinophil percentage) is a key laboratory feature of VLM, though it may be absent in OLM. The degree of eosinophilia correlates roughly with worm burden.
- Liver function tests: Elevated transaminases suggest hepatic involvement.
- Imaging: Liver ultrasound or MRI may show focal hyperechoic lesions (eosinophilic granulomas). Chest X-ray may show transient infiltrates in pulmonary VLM. For OLM, dilated indirect ophthalmoscopy with fluorescein angiography identifies retinal lesions.
- Stool examination: Not useful — Toxocara does not produce eggs in humans (since larvae never mature into adult worms), so no eggs will be found in human stool.
8. Treatment (Albendazole)
Albendazole is the treatment of choice for symptomatic toxocariasis. Standard dosing is 400 mg twice daily for 5 days (for adults; weight-based dosing for children). Albendazole is a benzimidazole antiparasitic that inhibits tubulin polymerization in the worm, disrupting cellular processes and killing the larva. It achieves good tissue penetration and is effective against migrating larvae.
For VLM, treatment with albendazole resolves systemic symptoms and eosinophilia, and is generally recommended for all symptomatic cases. For OLM, management is more complex. Albendazole is used to kill the offending larva, but if the larva has already died, antiparasitic treatment will not reverse the damage. Corticosteroids are typically used to control the inflammatory reaction in OLM and protect vision. The timing of antihelminthic treatment relative to corticosteroids requires specialist guidance to avoid triggering an inflammatory surge from a dying larva.
Mebendazole is an alternative but has lower bioavailability than albendazole and is generally considered less effective for tissue migration syndromes. Diethylcarbamazine (DEC) has been used historically but is less well-studied for toxocariasis than albendazole.
9. Prevention — Pet Deworming and Handwashing
Toxocariasis is preventable through a combination of pet health maintenance and personal hygiene:
- Deworming puppies and kittens: Veterinary guidelines recommend deworming puppies starting at 2 weeks of age, continuing every 2 weeks until 8 weeks, then monthly until 6 months. Pregnant and nursing dogs should also be treated. Regular anthelmintic treatment of pet dogs and cats throughout their lives greatly reduces environmental contamination with Toxocara eggs.
- Prompt disposal of pet feces: Removing dog feces from yards, parks, and public spaces within 24 hours (before eggs embryonate to become infective) prevents environmental contamination. Picking up and bagging dog waste is a public health measure that reduces Toxocara transmission.
- Handwashing: Teaching children to wash hands after playing outdoors, before eating, and after touching soil or sand. Adults should wash hands after gardening or handling soil.
- Covering sandboxes: Keeping sandboxes covered when not in use prevents cats from using them as litter boxes.
- Washing vegetables: Thoroughly washing raw vegetables that may have been grown in contaminated soil.
- Avoiding pica: Counseling parents about the risks of soil ingestion (pica) in children, and assessing for iron deficiency (which can drive pica) in affected children.
Key Research Papers
Landmark studies and reviews on Toxocara epidemiology, clinical syndromes, and management.
- Despommier D. Toxocariasis: Clinical Aspects, Epidemiology, Medical Ecology, and Molecular Aspects. Clinical Microbiology Reviews. 2003;16(2):265–272.
- Won KY, Kruszon-Moran D, Schantz PM, Jones JL. National Seroprevalence and Risk Factors for Zoonotic Toxocara spp. Infection. American Journal of Tropical Medicine and Hygiene. — Search PubMed [PubMed PMID 18840750]
- Rubinsky-Elefant G, Hirata CE, Yamamoto JH, Ferreira MU. Human Toxocariasis: Diagnosis, Worldwide Seroprevalences, and Clinical Expression of the Systemic and Ocular Forms. Annals of Tropical Medicine and Parasitology. — Search PubMed [PubMed PMID 20109274]
- Pawlowski Z. Toxocariasis in Humans: Clinical Expression and Treatment Dilemma. Journal of Helminthology. — Search PubMed [PubMed PMID 11321591]
- Woodhall D, Eberhard M, Parise M. Neglected Parasitic Infections in the United States: Toxocariasis. American Journal of Tropical Medicine and Hygiene. — Search PubMed [PubMed PMID 25070995]
Live PubMed Searches
- Toxocariasis Toxocara canis human
- Ocular larva migrans Toxocara retina
- Visceral larva migrans eosinophilia
- Toxocara seroprevalence United States
- Albendazole toxocariasis treatment
- Toxocara soil contamination playground
Connections
- Toxocara Symptoms
- Visceral Larva Migrans
- Ocular Larva Migrans
- Diagnosis: ELISA and Imaging
- Toxocara Treatments
- Albendazole Treatment
- Ocular Toxocariasis Treatment
- Prevention and Pet Hygiene
- All Parasites
- Ascaris
- Hookworm
- Strongyloides
- Pinworm
- Ophthalmology
- Infectious Disease
- All Conditions