Hyperinfection Syndrome Management — ICU Protocol and Treatment
- Medical Emergency
- Immediate High-Dose Ivermectin
- Discontinue Immunosuppression
- Broad-Spectrum Antibiotics
- ARDS and Pulmonary Management
- HTLV-1 Co-infection Management
- Investigational Parenteral Ivermectin
- Monitoring Treatment Response
- ICU Outcomes and Mortality Data
- Key Research Papers
- PubMed Searches
- Connections
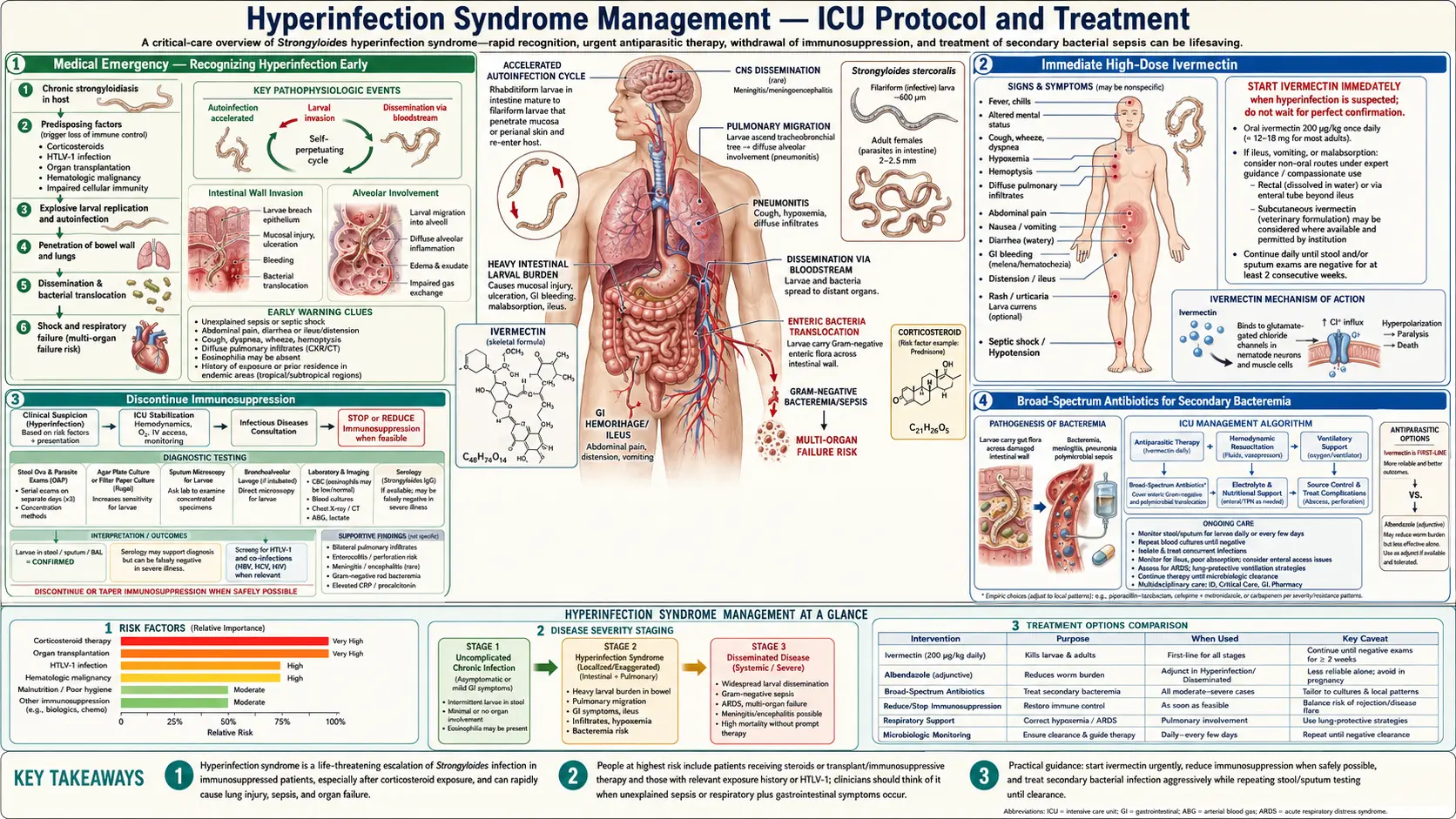
Medical Emergency — Recognizing Hyperinfection Early
Strongyloides hyperinfection syndrome is one of the few parasitic infections that can kill an immunocompromised patient within days of recognition — and within days to weeks of starting corticosteroids or other immunosuppressive therapy. It is not a subtle presentation. Patients develop severe abdominal pain, intractable diarrhea, profound weakness, and respiratory failure simultaneously. Yet it is routinely missed because clinicians do not think to ask about it and laboratories do not routinely perform ova-and-parasite examinations adequate to catch it.
The biology drives the urgency. In a normal host, Strongyloides stercoralis larvae complete their cycle slowly. In an immunocompromised host — particularly one on high-dose corticosteroids — the parasite shifts into a hyper-reproductive mode. Filariform (infective) larvae penetrate the intestinal wall in massive numbers, carrying gut bacteria with them into the bloodstream and peritoneum. The result is simultaneous parasitic disease and gram-negative septicemia.
ICU admission should be the default disposition for any patient with confirmed hyperinfection. Key early warning signs that should trigger immediate escalation include: larvae found in stool of a patient on steroids; unexplained gram-negative bacteremia without an obvious source in a patient from an endemic region; eosinophilia followed by sudden eosinopenia in an immunosuppressed patient (eosinopenia during active infection is a poor prognostic sign, not reassurance); and new pulmonary infiltrates with hemoptysis in a patient with abdominal pain.
Delay in diagnosis is the single greatest modifiable mortality risk. Every hour of untreated hyperinfection represents more larvae migrating through the gut wall, more bacteria seeding the bloodstream, and more organ systems failing. A standing institutional protocol for immediate parasitology consultation, three-tube stool collection, and empiric ivermectin initiation pending results saves lives.
Immediate High-Dose Ivermectin
Ivermectin at 200 mcg/kg/day is the cornerstone of hyperinfection management. This is the same weight-based dose used for uncomplicated strongyloidiasis, but the treatment duration extends far beyond the standard two-day course. Current expert consensus, supported by case series and infectious disease society guidelines, calls for continuing ivermectin until stool examination is negative for larvae on at least two consecutive tests performed two weeks apart — and some authors advocate extending to negative serology as well.
The practical challenge in hyperinfection is that patients are often too ill to reliably absorb oral medication. Paralytic ileus is common, gut-wall integrity is compromised by larval migration, and patients may be intubated and sedated. Standard oral ivermectin tablets assume intact small-bowel absorption, which cannot be guaranteed in disseminated disease.
When oral absorption is uncertain, clinicians have used several workarounds. Crushed ivermectin tablets given via nasogastric tube with lipid-rich feeds can improve absorption. The veterinary injectable formulation (1% ivermectin in propylene glycol, manufactured for livestock) has been administered subcutaneously in desperate cases, based on pharmacokinetic data showing adequate serum levels. Rectal administration of crushed tablets has also been described in case reports. None of these routes has been studied in randomized trials — the evidence base for all of them is observational.
The goal is not a set number of treatment days but documented parasitological cure. Repeat stool examination every 2 weeks while treatment continues. Do not stop ivermectin after 2 days just because a protocol chart says so — that approach is appropriate for uncomplicated chronic infection, not life-threatening hyperinfection.
Discontinue Immunosuppression
Corticosteroids and other immunosuppressants are not just contributing factors in hyperinfection — they are the direct biological trigger. Glucocorticoids appear to directly stimulate the parasite's reproduction in addition to suppressing the host's immune response. Stopping them is a treatment intervention, not merely supportive care.
The decision to stop immunosuppression is rarely simple. Patients on corticosteroids for organ transplant, severe asthma, inflammatory bowel disease, rheumatoid arthritis, or cancer chemotherapy regimens face competing risks. Stopping steroids abruptly can trigger adrenal insufficiency in patients who have been on them long-term. Stopping immunosuppression in a transplant patient risks acute rejection. Stopping chemotherapy may allow tumor progression.
Despite these real competing risks, the general principle in infectious disease is clear: an active life-threatening infection takes priority over immunosuppressive therapy whenever clinically possible. For transplant patients, this means urgent consultation between transplant medicine and infectious disease to balance rejection risk against hyperinfection mortality. For rheumatology patients, it often means a rapid steroid taper rather than abrupt cessation. For cancer patients, it means pausing chemotherapy until parasitological cure is confirmed.
In practice, the patient's underlying condition must be considered individually. Patients on physiologic replacement doses for adrenal insufficiency (typically less than 7.5 mg/day prednisone equivalent) cannot have steroids stopped without risking Addisonian crisis — these patients should continue replacement doses while being treated aggressively with ivermectin. Patients on pharmacologic doses for active inflammatory disease represent the middle ground where gradual tapering is usually preferred over immediate cessation.
Broad-Spectrum Antibiotics for Secondary Bacteremia
Gram-negative bacteremia and bacterial peritonitis are not complications of hyperinfection — they are part of the syndrome itself. Filariform larvae carry commensal gut bacteria on their cuticle as they migrate through the intestinal wall. The organisms most commonly cultured from blood and peritoneal fluid in hyperinfection cases include Escherichia coli, Klebsiella pneumoniae, Enterococcus faecalis, and Pseudomonas aeruginosa. Gram-positive organisms from the gut, including Streptococcus bovis and other streptococcal species, have also been reported.
Blood cultures should be obtained immediately upon suspecting hyperinfection — before antibiotics are started. The bacteremia in hyperinfection is often polymicrobial and can include unusual combinations of organisms that should prompt the clinician to consider the parasite as the common source.
Empiric antibiotic coverage must include robust gram-negative activity. Piperacillin-tazobactam (4.5 g IV every 6 hours) provides reliable coverage for enteric gram-negatives including Pseudomonas and is a reasonable first-line choice. In severely ill patients or those in settings with high rates of extended-spectrum beta-lactamase-producing organisms, escalation to meropenem (1 g IV every 8 hours) is appropriate. Enterococcal coverage (vancomycin or ampicillin-sulbactam) should be considered, particularly in patients with evidence of small-bowel involvement or prior antibiotic exposure that might have selected for vancomycin-resistant enterococci.
Antibiotic therapy should be continued for a minimum of 14 days or until documented bacteremia clears on repeat cultures — whichever is longer. Secondary meningitis from larval migration into the central nervous system has been reported; lumbar puncture should be performed if neurological symptoms develop.
ARDS and Pulmonary Management
Pulmonary involvement in disseminated strongyloidiasis is a marker of extreme severity. Larvae travel via the portal circulation to the right heart and pulmonary vasculature, where they exit capillaries and migrate through alveolar tissue. Bronchoalveolar lavage fluid may contain live filariform larvae — a dramatic and diagnostically confirming finding. Pulmonary hemorrhage results from larval disruption of capillary walls and can range from blood-tinged sputum to massive hemoptysis.
The radiographic pattern is bilateral infiltrates consistent with ARDS. Eosinophilic pneumonitis may precede full ARDS in patients with partial immune function. CT of the chest typically shows ground-glass opacities, consolidation, and sometimes miliary nodules from widespread larval seeding.
Mechanical ventilation follows standard ARDS-net protocols: low tidal volumes (6 mL/kg ideal body weight), plateau pressure limits below 30 cmH2O, and prone positioning when PaO2/FiO2 ratios fall below 150. The crucial difference from most ARDS management is that corticosteroids — a standard rescue therapy in refractory ARDS — are absolutely contraindicated when strongyloidiasis is the cause. Steroids will worsen the underlying infection even while potentially improving the pulmonary inflammatory response. This is a situation where the treatment of one component of the disease (ARDS) directly worsens the underlying cause. Most infectious disease specialists recommend against any corticosteroid use in the pulmonary phase.
BAL findings should be sent for parasitological examination as well as bacterial and fungal culture. If larvae are seen on BAL, this confirms disseminated disease and carries a particularly poor prognosis.
HTLV-1 Co-infection Management
Human T-cell lymphotropic virus type 1 (HTLV-1) is co-endemic with Strongyloides stercoralis in several regions, including the Caribbean, southern Japan, sub-Saharan Africa, and parts of South America. The combination is particularly dangerous because HTLV-1 impairs the specific CD4+ T-cell response that controls autoinfection, effectively creating an internal immunosuppression that mimics the effect of exogenous corticosteroids.
HTLV-1-positive patients with strongyloidiasis are at substantially higher risk of hyperinfection, more frequent relapse after apparently successful treatment, and treatment failure with standard ivermectin courses. Serology may show persistently elevated IgG titers even after adequate treatment, making serological cure confirmation more difficult than in HTLV-1-negative patients.
Antiretroviral therapy for HTLV-1 itself has been studied as a strategy to reduce hyperinfection risk. Zidovudine with interferon-alpha has shown some activity against HTLV-1 replication, though evidence for clinical benefit specifically in reducing Strongyloides hyperinfection is limited to observational data. The decision to initiate antiretroviral therapy for HTLV-1 should involve a specialist in this relatively rare co-infection.
In HTLV-1-positive patients with hyperinfection, extended ivermectin courses (beyond standard protocols) and more frequent monitoring are reasonable until two consecutive stool examinations separated by two weeks are both negative. Monthly suppressive ivermectin therapy has been used in patients with recurrent hyperinfection who cannot clear HTLV-1.
Investigational Parenteral Ivermectin
The most desperate clinical scenario in hyperinfection management is the patient with ileus who cannot absorb oral ivermectin and has no FDA-approved parenteral formulation available. Ivermectin is not approved for parenteral human use in the United States. The standard human formulation is an oral tablet. Yet the patients most likely to die of hyperinfection are precisely those with ileus and compromised gut absorption who cannot take oral medications.
Several approaches have been used in compassionate use situations. The veterinary injectable formulation (1% ivermectin solution in propylene glycol, sold as Ivomec for livestock) has been administered subcutaneously in humans, typically at the standard weight-based dose of 200 mcg/kg. Pharmacokinetic studies in healthy volunteers have shown that subcutaneous administration achieves similar or higher serum concentrations than oral dosing. The propylene glycol vehicle causes injection-site irritation but has been tolerated in reported cases.
Compounded intravenous formulations have also been prepared by hospital pharmacies in extreme cases, usually dissolving ivermectin in polyethylene glycol 400 and ethanol. These are not standardized, carry unknown infusion risks, and should be considered only when all other options are exhausted.
Rectally administered crushed ivermectin tablets, given as a suspension via enema, offer another route when oral absorption is unavailable and injectable formulations are not accessible. This approach relies on colonic absorption and may be incomplete, but has been described in case reports with apparent clinical response.
None of these alternative routes has been studied in controlled trials. The evidence base is entirely case series and reports. Any use requires informed consent, ethics committee consultation where time permits, and close pharmacokinetic monitoring if resources allow.
Monitoring Treatment Response
Clinical and parasitological monitoring in hyperinfection must be more intensive than for uncomplicated strongyloidiasis. The following framework guides monitoring during the acute phase:
Daily stool examination: Daily collection of stool samples for Baermann concentration technique or agar plate culture during the acute phase is ideal. The goal is to document whether the larval burden is decreasing. Rising larval counts despite treatment should prompt review of ivermectin dosing, absorption, and whether immunosuppression has been successfully reduced.
Serial serology: IgG ELISA titers decline slowly — over months — after successful treatment. Serology is not useful for monitoring acute treatment response. It is useful for confirming eventual cure (fourfold decline in titer) and detecting relapse in the months after apparent cure.
Organ function panels: Daily complete metabolic panel, complete blood count, and coagulation studies are appropriate in ICU patients. Liver function tests may show transaminase elevation from hepatic larval migration. Creatinine trends reflect acute kidney injury from sepsis. Coagulopathy suggests disseminated intravascular coagulation from overwhelming bacteremia.
Mortality predictors: Several factors have been associated with higher mortality in published series. APACHE II scores above 20 at presentation carry poor prognosis. The number of organ systems affected (greater than two is associated with dramatically higher mortality). Larvae found in BAL fluid indicates severe pulmonary dissemination. Persistent larvaemia despite 72 hours of treatment suggests treatment failure. HTLV-1 co-infection doubles the expected mortality compared to HTLV-1-negative cases.
ICU Outcomes and Mortality Data
The mortality statistics for severe disseminated strongyloidiasis are sobering and should be communicated honestly to families during goals-of-care discussions. Published case series and systematic reviews consistently report mortality rates between 70% and 90% for patients with full disseminated disease — defined as larvae found outside the gut and lung, such as in the central nervous system, liver, heart, or urinary tract.
Even in patients with hyperinfection limited to the gut and lungs (without true extrapulmonary dissemination), mortality rates in reported series range from 15% to 45%. The difference between hyperinfection (gut and lung involvement) and dissemination (extrapulmonary spread) is clinically important for prognosis, though the distinction is not always clear early in the course.
Factors associated with survival in reported cases include: early diagnosis before multiple-organ failure develops; rapid initiation of ivermectin before third-organ involvement; successful reduction or cessation of immunosuppression; adequate antibiotic coverage for secondary bacteremia; and availability of experienced intensive care support. Institutional experience matters — centers that have managed multiple cases of hyperinfection tend to have better outcomes, likely reflecting earlier recognition and faster protocol initiation.
Case reports of survivors of severe disseminated strongyloidiasis document complete neurological and pulmonary recovery in some patients, though the journey typically involves weeks of ICU care, prolonged mechanical ventilation, multiple antibiotic courses, and months of extended ivermectin therapy. These survivors are the exception rather than the rule, but they demonstrate that recovery is possible with aggressive, early, and coordinated management.
For patients who survive the acute episode, follow-up at 3, 6, and 12 months is recommended, including repeat serology and stool examination. Reactivation can occur if immunosuppression is resumed, and some HTLV-1-positive patients require indefinite suppressive therapy.
Key Research Papers
- Marcos LA et al. Disseminated strongyloidiasis: an emerging and under-recognized public health problem. Trans R Soc Trop Med Hyg. Search PubMed [PubMed PMID 21208913]
- Siddiqui AA, Berk SL. Diagnosis of Strongyloides stercoralis infection. Clin Infect Dis. Search PubMed [PubMed PMID 17238140]
- Concha R et al. Disseminated strongyloidiasis and hyperinfection syndrome. Curr Gastroenterol Rep. Search PubMed [PubMed PMID 22715901]
- Nutman TB. Human infection with Strongyloides stercoralis and other related Strongyloides species. Parasitology. Search PubMed [PubMed PMID 26063631]
- Ghoshal UC et al. Strongyloides stercoralis infestation and tropical sprue: a coincidence or a connection? J Gastroenterol Hepatol. Search PubMed [PubMed PMID 25310989]
- Buonfrate D et al. Severe strongyloidiasis: a systematic review of case reports. BMC Infect Dis. Search PubMed [PubMed PMID 23536768]
- Henriquez-Camacho C et al. Ivermectin versus albendazole or thiabendazole for Strongyloides stercoralis infection. Cochrane Database Syst Rev. Search PubMed [PubMed PMID 27174396]
- Iriemenam NC et al. Strongyloides stercoralis infection in an HIV-seronegative patient treated with ivermectin. Int J Infect Dis. Search PubMed [PubMed PMID 28895697]
- Krolewiecki AJ et al. A public health response against Strongyloides stercoralis: time to refine the research agenda. PLoS Negl Trop Dis. Search PubMed [PubMed PMID 26580609]
- Bisoffi Z et al. Strongyloides stercoralis: a plea for action. PLoS Negl Trop Dis. Search PubMed [PubMed PMID 22046048]
PubMed Searches
- Strongyloides hyperinfection ICU management
- Disseminated strongyloidiasis mortality
- Ivermectin parenteral subcutaneous Strongyloides
- Strongyloides HTLV-1 hyperinfection treatment
- Strongyloides bacteremia gram-negative sepsis
Connections
- All Parasites
- Strongyloides Main Page
- Symptoms Hub
- Hyperinfection & Dissemination (Symptoms)
- Ivermectin Treatment
- Prevention and Screening
- Treatments Hub
- Infectious Disease