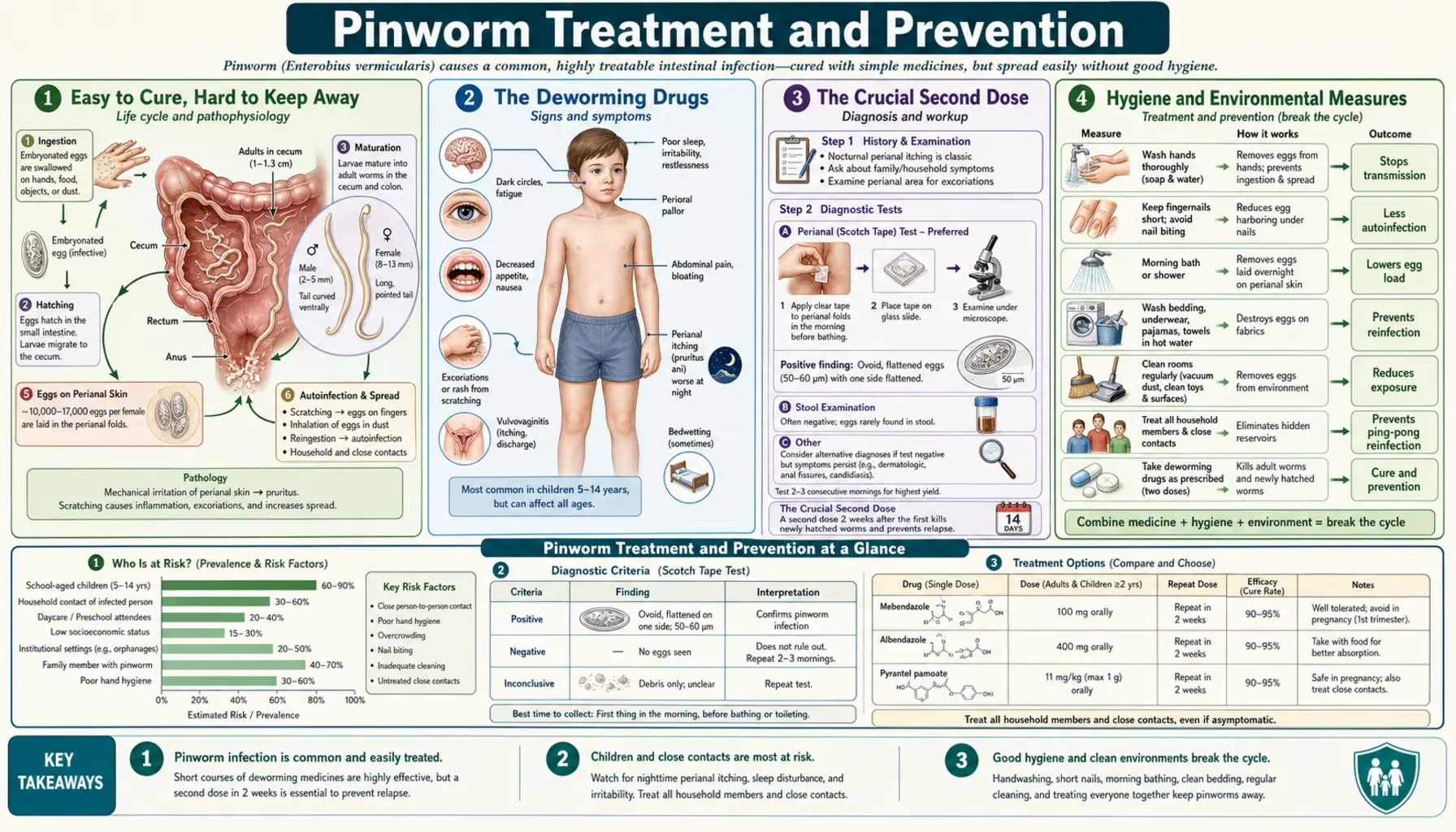
Pinworm Treatment and Prevention
Pyrantel & Albendazole Treatment
The simple over-the-counter and prescription cures — and why a second dose two weeks later matters.
Hygiene & Preventing Reinfection
Handwashing, short nails, morning showers, and hot-washing bedding to break the cycle.
Recurrent Pinworm & the Whole Household
When pinworm keeps coming back — treating everyone at once and outlasting the eggs.
Here is the good news, stated plainly and up front: pinworm is one of the easiest infections in all of medicine to cure. A single dose of a safe, inexpensive deworming pill — one you can buy without a prescription in the United States — kills the worms living in the gut. The medicine works the first time, nearly every time. If pinworm were judged on how hard the worms are to kill, it would barely register as a problem at all.
So why does pinworm have a reputation for being stubborn, for “coming back” again and again, for sweeping through a whole household and refusing to let go? The answer is the single most important idea on this page: the challenge of pinworm is not killing the worms — it is preventing reinfection. The drugs do their job in hours. But pinworm eggs are sticky, microscopic, and everywhere — under fingernails, on bedding, on door handles, in the dust — and a person can swallow a fresh batch and start the whole cycle over again the very day after a perfect cure. Treatment, therefore, is really two jobs done together: take the medicine to clear today's worms, and stop the eggs from putting new worms back. Do both, and pinworm ends. This page walks through the drugs, the crucial repeat dose, the hygiene that breaks the cycle, treating everyone in the home at once, and — most of all — the strong reassurance that this is a thoroughly beatable, harmless nuisance, not a dangerous disease. (Treatment information here is summarized as reported in the medical literature; actual treatment is clinician-directed.)
Table of Contents
- Easy to Cure, Hard to Keep Away
- The Deworming Drugs
- The Crucial Second Dose
- Hygiene and Environmental Measures
- Treat the Whole Household at Once
- The Autoinfection Cycle That Drives Reinfection
- Safety in Pregnancy and Young Children
- Reassurance: This Is Beatable
- Key Research Papers
- Featured Videos
1. Easy to Cure, Hard to Keep Away
Pinworm (Enterobius vermicularis) is the most common worm infection in the United States and across temperate, developed countries, and it is overwhelmingly an infection of children — though anyone in a household with an infected child can catch it. For all its prevalence, it is a remarkably gentle parasite: it does not invade the bloodstream, it does not damage organs in the ordinary case, and the typical symptom is simply intense night-time itching around the anus, caused by the female worms crawling out to lay their eggs on the surrounding skin while the child sleeps.
Because the worms themselves are so vulnerable to medication, the cure rate of a single appropriate dose is very high — in the region of 90–100% for clearing the adult worms present at the time. If pinworm simply went away after one pill, there would be little more to say. The reason it has a reputation for persistence lies entirely in its life cycle. A female pinworm deposits thousands of eggs on the perianal skin; those eggs become infectious within hours; and they are then transferred — on scratching fingers, on bedclothes, on towels, into household dust — back to the same person's mouth or to other people in the home. Swallowed eggs hatch and grow into new adult worms, and the cycle resets.
This is why effective treatment is always described as a two-part strategy: a deworming medicine to kill the worms that are present, combined with hygiene and environmental measures to stop fresh eggs from being swallowed. Neither half alone is reliable. Medicine without hygiene leaves the door open to reinfection; hygiene without medicine leaves the current generation of worms in place. Together, they end the infection. The sections below take each piece in turn and link to the focused pages that cover the drugs, the hygiene, and the whole-household approach in full detail.
2. The Deworming Drugs
Three medicines do the heavy lifting in pinworm treatment, and all three share two appealing features: each is given as a single dose, and each is very safe. This is an overview; the doses, brand names, how the drugs work, and side effects are covered in depth on the Pyrantel & Albendazole Treatment page.
- Pyrantel pamoate — this is the one you can buy over the counter in the United States, sold as a chewable tablet or liquid specifically for pinworm. It works by paralyzing the worms, which then lose their grip on the gut wall and are passed out in the stool. Its over-the-counter availability makes it the most accessible first option for families, and it has a long, reassuring safety record.
- Mebendazole — a member of the benzimidazole family, given as a single chewable tablet. It works by starving the worm: it blocks the parasite's ability to take up glucose, so the worm runs out of fuel and dies. Mebendazole has been a standard pinworm treatment for decades.
- Albendazole — a close relative of mebendazole in the same benzimidazole family, also given as a single dose and working by the same fuel-starvation mechanism. It is widely used and highly effective.
For practical purposes the three are interchangeable in their core job: a single dose of any one of them will clear the adult worms in the great majority of cases. The choice often comes down to availability and cost — in the U.S., pyrantel pamoate's over-the-counter status frequently makes it the simplest place to start, while mebendazole and albendazole are obtained through a pharmacist or prescriber depending on local supply. What matters far more than which drug is chosen is the point made in the next section: one dose is usually not the whole treatment.
3. The Crucial Second Dose
This is the single most important practical instruction in treating pinworm, and the one most often missed: a second dose, given about two weeks after the first, is almost always needed. Skipping it is the most common reason a “treated” pinworm infection appears to come straight back.
The reason lies in what the drugs can and cannot do. The deworming medicines kill the adult worms living in the intestine very effectively — but they do not kill pinworm eggs. At the moment a person takes the first dose, there are almost certainly eggs already present: eggs that were swallowed in the days before treatment and have not yet hatched, and eggs newly deposited on the skin. Those eggs are untouched by the medicine. Over the following one to two weeks, they hatch and grow into a fresh crop of adult worms — and the symptoms return, making it look as though the first treatment failed.
It did not fail. It cleared the worms that were there. The repeat dose two weeks later is timed to catch this second generation — the worms that hatched from eggs the first dose could not reach — after they have matured into killable adults but before they have had the chance to lay a new round of eggs. By spacing the two doses about two weeks apart, the treatment brackets the worm's life cycle: the first dose clears the present infection, and the second dose mops up everything that hatched afterward, closing the window the eggs would otherwise exploit. Many clinicians and product instructions specify exactly this two-dose schedule for pinworm, precisely because the egg stage is the parasite's escape route from a single treatment. If you remember nothing else about the medicine, remember this: take the second dose.
4. Hygiene and Environmental Measures
If the drugs handle the worms, hygiene handles the eggs — and since reinfection is the real enemy, the hygiene half of treatment is just as important as the pill. These are common-sense, low-cost steps, but they have to be done together and kept up for a couple of weeks to break the cycle. This is an overview; the full routine, the reasoning behind each step, and how long to keep it going are covered on the Hygiene & Preventing Reinfection page.
The core measures are:
- Frequent, thorough handwashing — especially after using the toilet, after scratching, and before eating or preparing food. Hands carry eggs from the perianal skin to the mouth; clean hands break that bridge. This is the single most effective hygiene step.
- Keep fingernails short and clean — and discourage nail-biting and thumb-sucking in children. Eggs lodge under the nails during scratching at night and are swallowed when fingers go to the mouth. Short, clean nails leave them nowhere to hide.
- Shower in the morning — a morning shower (rather than an evening bath) washes away the eggs that the female worms laid on the skin overnight, before they can be spread through the day. Showering rinses eggs away; a bath can leave them floating in the water.
- Hot-wash bedding, underwear, and towels — washing these in hot water and drying them on a hot cycle, particularly in the first days of treatment, removes and destroys the eggs that collect on fabric. Changing into clean underwear each morning and not shaking out bedclothes (which can scatter eggs into the air and dust) helps too.
None of these steps is dramatic, and none needs special products. Their power comes from doing them consistently for a couple of weeks while the medicine clears the worms, so that no fresh eggs are being swallowed during the window when the parasite would otherwise re-establish itself.
5. Treat the Whole Household at Once
Pinworm is a household infection, not just an individual one — and treating it as if only one person is affected is a classic recipe for endless “ping-pong” reinfection, where the worm bounces from one family member to another and back again. This section is an overview; the strategy for stubborn, recurring cases — including when and how to treat everyone simultaneously and how to outlast the eggs in the environment — is covered on the Recurrent Pinworm & the Whole Household page.
The problem is straightforward. Pinworm eggs spread easily among people living together, especially among children sharing bedrooms, bathrooms, and play. Crucially, many infected people have no symptoms at all — they carry and shed eggs without itching or any sign of infection. So when one child is diagnosed and treated, untreated siblings or parents who are silently infected continue to seed the home with eggs, reinfecting the child who was just cured. The cure looks like a failure, when in fact the source was never addressed.
The solution that finally ends this cycle, particularly in recurrent cases, is to treat every member of the household at the same time — usually with the same two-dose schedule (a dose now and a repeat about two weeks later) — combined with the household-wide hygiene measures described above, done in concert. Treating everyone together means there is no untreated reservoir left to restart the infection: the worms in everyone are killed on the same timetable, the eggs are cleared from the shared environment at the same time, and the chain has nowhere left to continue. For a single, first-time case this whole-family approach is not always necessary; but when pinworm keeps returning, simultaneous household treatment is the move that breaks the loop for good.
6. The Autoinfection Cycle That Drives Reinfection
To understand why pinworm is so persistent — and why the two-dose, hygiene-plus-medicine strategy is built the way it is — it helps to see the loop the parasite uses to keep itself going inside a single person. This loop is called autoinfection: self-reinfection, where one person keeps re-seeding their own gut without any new exposure from outside.
The cycle runs like this. Adult female pinworms live in the lower intestine. At night, the females migrate down and out through the anus to lay their eggs on the surrounding perianal skin — and this egg-laying is what causes the hallmark night-time itching. The itch provokes scratching, which loads the eggs onto the fingers and under the fingernails. Then, when the (often sleeping or young) person puts their fingers to their mouth — nail-biting, thumb-sucking, or simply touching food — the eggs are swallowed. The swallowed eggs hatch in the gut, the larvae mature into new adult worms, and those worms migrate down to lay eggs again. Itch, scratch, swallow, repeat — a self-sustaining loop that can keep an infection going indefinitely.
Seeing the loop laid out makes the treatment logic click into place. The night-time itching is not a random symptom; it is the engine of the cycle, the step that moves eggs from skin to fingers. Every element of treatment is aimed at breaking one link in this chain: the medicine removes the adult worms doing the egg-laying; the second dose catches the next generation before it can lay; the morning shower washes away the eggs from the skin before they reach the fingers; handwashing and short nails stop eggs on the fingers from reaching the mouth; and hot-washed bedding removes eggs from the surfaces that would otherwise re-deliver them. Once you can see autoinfection, the whole strategy reads as a deliberate, coordinated attack on a single cycle — which is exactly what it is.
7. Safety in Pregnancy and Young Children
Two groups understandably prompt extra caution about deworming medicines: pregnant women and very young children. The reassuring general picture is that pinworm is mild and the treatments are well tolerated, and that the decision and choice of drug in these situations should be guided by a clinician.
In pregnancy, pinworm is rarely a threat to the pregnancy itself, so treatment is often a matter of comfort and stopping spread rather than urgent necessity, and it may sometimes be deferred or managed conservatively. When medication is used, pyrantel pamoate is frequently the preferred choice in pregnancy, because it is poorly absorbed from the gut into the bloodstream — it does its work locally on the worms in the intestine and very little enters the rest of the body. The benzimidazoles (mebendazole and albendazole) are generally avoided or used more cautiously in pregnancy, particularly in the first trimester. These are decisions for a doctor or midwife to make with the individual patient.
In young children, pinworm is extremely common and the standard treatments are used widely and safely, but the appropriate drug and dose depend on the child's age and weight, and the very youngest children may need specific guidance. Here too, the practical message is reassuring: these are routine, low-risk treatments for a routine, low-risk infection — but in pregnancy and in the youngest children, the specific choice is best confirmed with a clinician rather than self-directed.
8. Reassurance: This Is Beatable
It is worth ending where the page began, because anxiety is often the worst symptom of pinworm. Discovering worms — in a child, or in oneself — can feel alarming and even shameful, and the frustration of a case that seems to keep returning can make it feel like a problem that will never end. None of that distress is warranted by the medical reality.
The facts are genuinely encouraging. Pinworm is not dangerous: it does not cause lasting harm, it does not invade organs, and serious complications are rare. It is not a sign of poor hygiene or a dirty home — it is the most common worm infection in well-off, clean households precisely because it spreads so easily among children, regardless of how spotless the home is. And it is completely curable. The medicine works; the second dose closes the gap; the hygiene and whole-household measures stop reinfection. When all the pieces are done together — treat the worms, take the repeat dose, keep up the hygiene, and treat everyone in the home if it keeps coming back — pinworm reliably ends.
So the bottom line is simple and worth holding onto: this is a thoroughly beatable, harmless nuisance, not a serious disease. Approach it methodically rather than anxiously, follow the two-part plan through to the second dose, and the infection goes away. For the step-by-step specifics, the focused pages — on the deworming drugs, on hygiene and preventing reinfection, and on recurrent pinworm and treating the whole household — carry the detail.
Key Research Papers
Peer-reviewed reviews, clinical studies, and epidemiological surveys on the treatment, reinfection, diagnosis, and complications of pinworm (enterobiasis). Journal names appear as plain text; the year/volume/pages link opens the full citation via DOI.
- St Georgiev V. Chemotherapy of Enterobiasis (Oxyuriasis). Expert Opinion on Pharmacotherapy. 2001;2(2):267–275.
- Cook GC. Enterobius vermicularis Infection. Gut. 1994;35(9):1159–1162.
- Burkhart CN, Burkhart CG. Assessment of Frequency, Transmission, and Genitourinary Complications of Enterobiasis (Pinworms). International Journal of Dermatology. 2005;44(10):837–840.
- Matsen JM. Reinfection in Enterobiasis (Pinworm Infection). American Journal of Diseases of Children. 1969;118(4):576–581.
- Keiser J, Utzinger J. Efficacy of Current Drugs Against Soil-Transmitted Helminth Infections: Systematic Review and Meta-Analysis. JAMA. 2008;299(16):1937–1948.
- Fierlafijn E. Mebendazole in Enterobiasis. JAMA. 1971;218(7):1051.
- Singh S, Samantaray JC. Topical Anthelmintic Treatment of Recurrent Genitourinary Enterobiasis. Genitourinary Medicine. 1989;65(4):284–285.
- McDonald GSA, Hourihane DO'B. Ectopic Enterobius vermicularis. Gut. 1972;13(8):621–626.
- Laoraksawong P, Pansuwan P, Krongchon S, et al. Prevalence of Enterobius vermicularis Infections and Associated Risk Factors among Schoolchildren in Nakhon Si Thammarat, Thailand. Tropical Medicine and Health. 2020;48(1):42.
- Wang S, Hwang KP, Chen ER, et al. Enterobius vermicularis Infection in Schoolchildren: A Large-Scale Survey 6 Years after a Population-Based Control. Epidemiology and Infection. 2010;138(1):28–36.
Live PubMed Searches
Each link opens a live PubMed query so results stay current as new papers are indexed.
- Enterobius vermicularis treatment
- Pinworm pyrantel pamoate enterobiasis
- Mebendazole albendazole enterobiasis cure rate
- Enterobiasis reinfection and second dose
- Pinworm household and family transmission
- Enterobius vermicularis autoinfection life cycle
- Pyrantel pamoate pregnancy safety
- Enterobiasis children hygiene and prevention
Connections
- Pinworm Overview
- Symptoms & Diagnosis
- Anal Itching & Sleep Disturbance
- Pinworm in Children & Households
- Complications & Unusual Sites
- Pyrantel & Albendazole Treatment
- Hygiene & Preventing Reinfection
- Recurrent Pinworm & the Whole Household
- All Parasites
- Gastroenterology
- Infectious Disease
- All Conditions