Spinal Stenosis
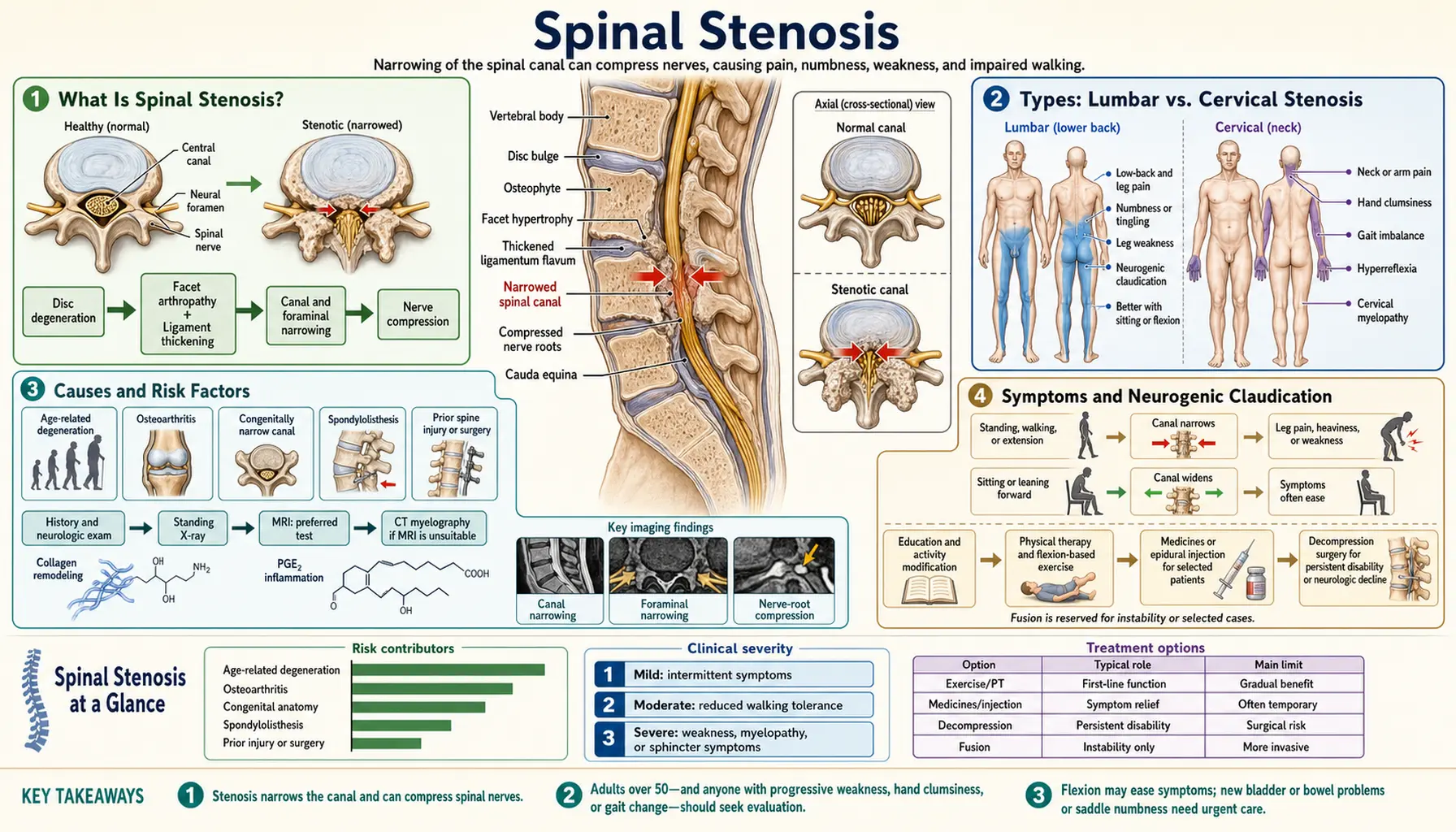
Spinal stenosis is a narrowing of the spaces within the spine that puts pressure on the nerves traveling through the spinal canal. It most commonly affects the lower back (lumbar stenosis) and the neck (cervical stenosis), causing pain, numbness, tingling, and weakness in the arms or legs. While some people with spinal stenosis have no symptoms at all, others experience significant limitations in their ability to walk, stand, or perform daily activities. The condition becomes more common with age and is one of the leading causes of spine surgery in adults over 65.
- What Is Spinal Stenosis?
- Types: Lumbar vs. Cervical Stenosis
- Causes and Risk Factors
- Symptoms and Neurogenic Claudication
- Diagnosis (MRI, CT Myelogram, Physical Exam)
- Conventional Treatment (Medications, Epidural Injections, Surgery)
- Physical Therapy and Exercise
- Natural and Complementary Approaches
- Surgical Options (Laminectomy, Spinal Fusion, MILD Procedure)
- Complications and Prognosis
- Living With Spinal Stenosis
- Key Research Papers
- Connections
What Is Spinal Stenosis?
The spinal canal is a tube of bone and ligament that runs the length of your backbone, protecting the spinal cord and the nerve roots that branch off it. In a healthy spine, this canal provides ample room for the nerves. Spinal stenosis occurs when something causes that canal — or the smaller openings where nerve roots exit (foramina) — to become too narrow. When nerves get compressed inside a tight space, they send out distress signals: pain, burning, tingling, numbness, or weakness that can travel far from the actual site of compression.
The word "stenosis" simply means narrowing, and it can happen anywhere along the spine. However, the lower back and the neck are by far the most common locations because those are the segments of the spine that bear the most mechanical load and move the most over a lifetime. The thoracic (mid-back) region is affected far less often because its connection to the rib cage limits movement and wear.
Spinal stenosis affects an estimated 250,000 to 500,000 people in the United States, and imaging studies suggest that structural narrowing is present in a much larger portion of the aging population — many without symptoms. The condition is rarely dangerous on its own, but severe cases can lead to cauda equina syndrome (loss of bladder or bowel control), which is a surgical emergency requiring immediate attention.
Types: Lumbar vs. Cervical Stenosis
Lumbar spinal stenosis involves narrowing in the lower back, specifically in the region between the first lumbar vertebra (L1) and the fifth (L5), or at the L5-S1 junction. This is the most common form and typically causes symptoms in the buttocks, thighs, calves, and feet. The hallmark feature is neurogenic claudication — leg pain and weakness that worsens with walking or standing and is relieved by sitting or bending forward (like leaning over a shopping cart). This positional component is what distinguishes spinal stenosis from simple herniated disc or peripheral artery disease.
Cervical spinal stenosis affects the neck region (C1 through C7). Because the spinal cord itself passes through this part of the canal — not just individual nerve roots — cervical stenosis can produce a syndrome called cervical myelopathy, which involves coordination problems, difficulty with fine motor tasks (like buttoning a shirt), balance issues, and in severe cases, weakness or spasticity in the arms and legs. Neck pain and radiating arm pain (cervical radiculopathy) are also common. Cervical stenosis with myelopathy is considered more urgent than lumbar stenosis because the spinal cord itself is at risk.
Foraminal stenosis refers specifically to narrowing of the nerve exit holes (foramina) on either side of the vertebrae, rather than the central canal. This type often affects just one nerve root, producing symptoms on one side of the body. It can occur at any spinal level and frequently results from bone spurs growing into the foraminal opening or from disc collapse that reduces the height of the opening.
Tandem stenosis — narrowing at both cervical and lumbar levels simultaneously — occurs in a subset of patients, particularly older adults, and can make diagnosis more complex because symptoms from both regions overlap.
Causes and Risk Factors
The vast majority of spinal stenosis cases are degenerative — meaning they develop gradually over time as a result of normal aging wear on the spine's structures. However, several specific processes contribute to the narrowing:
Osteoarthritis and bone spurs (osteophytes): As the facet joints that link vertebrae together degenerate, the body attempts to stabilize the joint by growing extra bone. These bone spurs can project into the spinal canal or foramina, directly compressing nerves. Facet joint arthritis is present in nearly all cases of lumbar stenosis in older adults.
Ligamentum flavum hypertrophy: The ligamentum flavum is a tough yellow ligament that lines the back wall of the spinal canal. With age, it can thicken and buckle inward when the spine is extended (straightened or bent backward), significantly reducing available space for the nerve roots. Thickened ligamentum flavum is a major contributor to the postural nature of lumbar stenosis symptoms.
Disc degeneration and herniation: Intervertebral discs lose water content and height with age. A flattened disc reduces foraminal height, and disc material that bulges or herniates into the canal adds to compression. Disc collapse also causes the vertebrae above and below to settle closer together, further narrowing the openings.
Spondylolisthesis: This occurs when one vertebra slips forward over the one below it. The mismatch in alignment creates a kink in the canal. Degenerative spondylolisthesis (without a fracture) is particularly common in the L4-L5 segment of middle-aged and older women.
Congenital factors: Some people are born with a naturally narrower spinal canal. They may be asymptomatic for decades, but any additional age-related narrowing quickly pushes them into symptomatic territory.
Paget's disease of bone: This condition causes abnormal bone remodeling that can lead to enlarged, deformed vertebrae that encroach on the canal. It is an uncommon but recognized cause of stenosis in older adults.
Risk factors include age over 50, female sex (for degenerative spondylolisthesis), a history of spine injury or surgery, obesity (which increases mechanical load on the lumbar spine), occupations involving heavy lifting or prolonged spinal loading, and a family history of spinal problems.
Symptoms and Neurogenic Claudication
Spinal stenosis symptoms range from mild and intermittent to severe and disabling. The pattern of symptoms depends heavily on the location and degree of narrowing.
Neurogenic claudication is the defining symptom of lumbar spinal stenosis. Patients describe a cramping, aching, or burning sensation in the legs — sometimes described as heaviness or a feeling that their legs will give out — that comes on after walking a certain distance or standing for a period of time. The distance or time before symptoms appear varies widely: some people can walk only a block, while others can manage half a mile before discomfort forces them to stop. The key distinguishing feature is that bending forward, sitting down, or leaning over something provides rapid relief. This is because forward flexion opens up the spinal canal slightly, reducing pressure on the compressed nerve roots. Patients often unconsciously adopt a flexed posture and may find they can walk longer distances pushing a grocery cart (the "shopping cart sign").
Lumbar stenosis symptoms also include pain in the low back, buttocks, or thighs; numbness or tingling running down one or both legs; and in more severe cases, weakness in the legs that may cause stumbling or difficulty climbing stairs. The symptoms are often bilateral (both legs), though one side may be worse than the other.
Cervical stenosis symptoms include neck pain; pain, numbness, or tingling radiating into one or both arms (cervical radiculopathy); and — when the spinal cord is compressed — cervical myelopathy. Myelopathy symptoms include clumsy hands (trouble with fine motor tasks), a peculiar "electric shock" sensation down the spine when the neck is flexed (Lhermitte's sign), gait instability (wide-based walking, tendency to fall), urinary urgency or incontinence in advanced cases, and diffuse weakness.
Red flag symptoms that warrant urgent evaluation include sudden onset of bladder or bowel dysfunction (inability to urinate or loss of bowel control), rapidly progressive leg weakness, or saddle anesthesia (numbness in the groin and inner thighs). These may signal cauda equina syndrome — a neurological emergency requiring surgery within hours to prevent permanent paralysis.
Diagnosis (MRI, CT Myelogram, Physical Exam)
Diagnosing spinal stenosis requires combining the patient's clinical history and physical examination with appropriate imaging. The diagnosis is never made on imaging alone — many people have significant structural narrowing on MRI but no symptoms, and treatment decisions must be based on the clinical picture.
Medical history and symptom review are central to the diagnostic process. A spine specialist will ask about the specific character of leg or arm symptoms, what makes them better or worse (especially the positional component), how far the patient can walk, and whether symptoms have progressed. The history of neurogenic claudication — worsening with walking, relieved by sitting — is so characteristic that it often points directly to lumbar stenosis before any imaging is ordered.
Physical examination may reveal limited range of motion in the spine, tenderness over the affected vertebral segments, and neurological deficits including reduced reflexes, muscle weakness, or sensory loss in a dermatomal pattern. The "stoop test" — having the patient walk until symptoms appear, then stoop forward — can confirm the postural nature of lumbar stenosis. However, physical examination findings can be subtle or absent in early cases.
MRI (magnetic resonance imaging) is the gold-standard imaging study for spinal stenosis. It provides high-resolution images of the spinal canal, disc tissue, ligaments, nerve roots, and spinal cord without radiation. MRI can quantify the degree of canal narrowing, identify thickened ligamentum flavum, detect disc herniations, and show nerve root compression directly. The cross-sectional area of the dural sac (the membrane surrounding the spinal cord and nerve roots) can be measured; a value below 100 mm² at the lumbar level is generally considered stenotic.
CT myelography remains useful when MRI is contraindicated (patients with certain pacemakers or metallic implants) or when the degree of bony narrowing needs to be more precisely defined. In this procedure, contrast dye is injected into the spinal fluid space and CT images are obtained, providing excellent detail of the bony anatomy and the outline of the compressed nerve roots.
Electrodiagnostic studies (EMG and nerve conduction velocity tests) can help distinguish spinal stenosis from peripheral neuropathy, peripheral artery disease, or hip pathology, all of which can mimic stenosis symptoms. They are particularly useful when the clinical picture is ambiguous or when multiple diagnoses may coexist.
Differential diagnosis includes peripheral artery disease (vascular claudication), hip osteoarthritis, peripheral neuropathy, lumbar disc herniation, sacroiliac joint dysfunction, and — in the cervical spine — amyotrophic lateral sclerosis (ALS) or multiple sclerosis when myelopathy is the presenting feature.
Conventional Treatment (Medications, Epidural Injections, Surgery)
Treatment for spinal stenosis is guided by symptom severity. Mild to moderate stenosis with manageable symptoms is typically treated conservatively first, reserving more invasive options for patients who fail to improve or whose symptoms are severe from the outset.
NSAIDs (nonsteroidal anti-inflammatory drugs) such as ibuprofen or naproxen can reduce inflammation around compressed nerve roots and provide pain relief. They are most useful for short-term flares and should be used with caution in older adults due to risks of gastrointestinal bleeding, kidney stress, and cardiovascular effects. Acetaminophen is a safer alternative for pure pain relief, though it does not address inflammation.
Neuropathic pain medications such as gabapentin (Neurontin) and pregabalin (Lyrica) are frequently prescribed for the radiating, burning, or tingling nerve pain associated with stenosis. These drugs work by dampening abnormal electrical signaling in compressed nerve roots. Side effects include drowsiness, dizziness, and cognitive blunting, which can be particularly problematic in older adults.
Muscle relaxants (cyclobenzaprine, methocarbamol) may help when painful muscle spasm accompanies stenosis-related pain, though evidence for their efficacy specifically in stenosis is limited.
Opioid analgesics are generally avoided in spinal stenosis due to the chronic nature of the condition and the high risks of dependence, falls (especially in older adults), and cognitive side effects. They may be considered for short-term use during severe acute exacerbations when other options have failed.
Epidural steroid injections (ESIs) deliver corticosteroid medication directly into the epidural space around the compressed nerve roots, reducing local inflammation and swelling. They can provide significant but usually temporary relief — typically weeks to a few months. The SPORT trial and subsequent studies showed that ESIs provide short-term symptom reduction in lumbar stenosis patients, though they do not appear to alter the long-term course of the disease or reduce the eventual rate of surgery. Most specialists recommend limiting injections to three per year at any given spinal level to avoid potential side effects such as bone density loss, adrenal suppression, and rare epidural abscess.
Calcitonin (a hormone involved in bone metabolism, available as a nasal spray) has been studied for spinal stenosis based on its potential to reduce pain through central nervous system effects. Some small trials showed modest benefit for walking capacity, but evidence is inconsistent and it is not widely used.
Physical Therapy and Exercise
Physical therapy is a cornerstone of conservative management for spinal stenosis and has strong evidence behind it. The goals are to reduce pain, improve functional capacity, strengthen the muscles that support the spine, and teach patients postures and movement strategies that minimize nerve compression.
Flexion-based exercise is particularly well suited to lumbar stenosis. Because forward bending opens the spinal canal, exercises that promote lumbar flexion — knee-to-chest stretches, posterior pelvic tilts, seated lumbar flexion — directly address the mechanical cause of symptoms. The Williams flexion exercises (a classic set developed by Paul Williams in 1937 specifically for lumbar pathology) remain widely used. These contrast with extension-based exercises (McKenzie protocol), which are better suited for pure disc herniations but tend to worsen stenosis symptoms.
Core stabilization training — strengthening the deep abdominal muscles (transversus abdominis), multifidus muscles, and pelvic floor — reduces the mechanical load on the lumbar spine during daily activities. A strong "core" acts like an internal brace, limiting the excessive spinal movement that aggravates stenosis. Studies show that supervised core stabilization programs lead to meaningful improvements in pain and function in stenosis patients.
Aquatic therapy (hydrotherapy) is particularly valuable for patients who cannot tolerate land-based exercise due to severe pain. Water buoyancy unloads the spine, allowing patients to walk and exercise with far less pain. The gentle resistance of water builds strength without heavy impact. Many patients find that walking in a pool is one of the few forms of aerobic activity they can perform without triggering neurogenic claudication.
Stationary cycling is another well-tolerated aerobic option. The forward-leaning, slightly flexed position on a bike naturally opens the lumbar canal, allowing many stenosis patients to sustain longer exercise sessions than walking permits. Recumbent bikes are especially comfortable as they support the lower back.
Manual therapy — joint mobilization and soft tissue techniques by a physical therapist or chiropractor — can reduce pain and improve mobility in some stenosis patients, though it must be applied carefully to avoid aggravating nerve compression. Traction (gently pulling apart the vertebrae to create more space) can provide temporary relief for some patients.
Posture and gait training teaches patients to maintain a slightly flexed lumbar spine during walking (leaning slightly forward), use assistive devices (walking poles or a walker) when helpful, and modify daily activities to reduce symptom-provoking positions. Education about pacing — stopping to rest before symptoms peak, then resuming — is a simple strategy that extends walking tolerance considerably.
A landmark comparative study (the SPORT trial, PMID 18287073) found that at 4-year follow-up, patients who had surgery for lumbar stenosis had greater improvements in pain and function than those treated non-operatively — but a substantial portion of non-operative patients also improved significantly, supporting a trial of conservative care before surgery for most patients.
Natural and Complementary Approaches
Several natural and complementary therapies have evidence or plausible biological rationale for helping manage spinal stenosis symptoms. These approaches work best as part of an integrated program alongside physical therapy and, when needed, conventional medical care.
Anti-inflammatory nutrition: A diet rich in omega-3 fatty acids (found in fatty fish like salmon and sardines), colorful vegetables, and whole grains while limiting processed foods, refined sugars, and trans fats can reduce systemic inflammation. Chronic low-grade inflammation amplifies nerve sensitivity and pain; reducing it through diet is a sensible background strategy. The Mediterranean diet, which emphasizes these foods, has been associated with lower levels of inflammatory markers in multiple studies.
Magnesium plays a role in nerve function and muscle relaxation. Deficiency — common in older adults — can worsen muscle spasm and nerve sensitivity. Magnesium glycinate or citrate (200–400 mg daily) is well tolerated and may reduce muscle cramping associated with stenosis. Foods rich in magnesium include leafy greens, pumpkin seeds, and dark chocolate. See Magnesium for detailed information.
Vitamin D3 is essential for bone health, muscle function, and nerve integrity. Deficiency is extremely common in people with chronic musculoskeletal pain, and correcting it can reduce pain sensitivity and improve muscle strength. Adequate vitamin D also supports the health of the vertebral bones themselves, potentially slowing the osteoarthritis progression that drives stenosis. See Vitamin D3.
Collagen and connective tissue support: Collagen is the primary structural protein in the intervertebral discs and spinal ligaments. Collagen peptide supplements combined with vitamin C have shown benefit for joint cartilage in some clinical trials, and the same principle may apply to disc health. See Collagen.
Curcumin (turmeric): Curcumin has documented anti-inflammatory and neuroprotective properties in animal and in vitro studies, with some positive human trials for osteoarthritis pain. Its bioavailability is low but can be enhanced by pairing with piperine (black pepper extract) or using phospholipid formulations. As an adjunct for pain management, curcumin is generally safe and may reduce the need for NSAIDs.
Acupuncture has a reasonable evidence base for chronic low back pain and neuropathic pain. Several controlled trials and systematic reviews suggest that acupuncture provides pain relief beyond placebo in back pain conditions, though study quality varies. For spinal stenosis specifically, acupuncture may help reduce the neurogenic pain component and improve quality of life.
TENS (transcutaneous electrical nerve stimulation) uses low-level electrical currents applied to the skin to interrupt pain signals. It is widely available, non-invasive, and safe. Evidence for TENS in spinal stenosis is modest, but many patients report useful symptomatic relief and it can be used as often as needed without cumulative side effects.
Heat and cold therapy — heating pads to relax muscle spasm, cold packs to reduce acute inflammation — are simple, low-cost tools that provide temporary relief and are safe for home use.
Weight management: Excess body weight, particularly central obesity, increases the mechanical load on the lumbar spine and accelerates degenerative changes. Losing even 10–15 pounds can meaningfully reduce the forces acting on compressed nerve roots. Weight loss also reduces systemic inflammation and improves the response to exercise therapy.
Surgical Options (Laminectomy, Spinal Fusion, MILD Procedure)
Surgery for spinal stenosis is generally recommended when conservative treatment has been tried for at least 3–6 months without adequate relief, when symptoms significantly impair daily function or quality of life, or when neurological deficits (weakness, loss of bladder/bowel control) are progressing. The choice of procedure depends on the location and extent of stenosis, the presence of spinal instability or deformity, and patient-specific factors such as age, bone density, and overall health.
Laminectomy (decompressive laminectomy) is the most common surgical procedure for lumbar spinal stenosis. The surgeon removes all or part of the lamina — the bony arch that forms the back wall of the spinal canal — along with any thickened ligamentum flavum and bone spurs, creating more space for the nerve roots. It is usually done through a midline incision under general anesthesia. Laminectomy alone is effective when the spine is stable; when instability is present (such as spondylolisthesis), fusion is typically added. The SPORT trial showed that at 8-year follow-up, patients who had laminectomy maintained significant advantages over non-operatively treated patients in terms of pain and function.
Spinal fusion is added to laminectomy when spinal instability exists — when one vertebra is slipping on another (spondylolisthesis), or when removing enough bone to decompress adequately would make the spine unstable. Fusion uses bone graft material (from the patient's own hip, a bone bank, or synthetic sources) along with metal screws and rods to permanently join two or more vertebrae together. The Swedish Spinal Stenosis Study (PMID 27074066) found that adding fusion to decompression did not improve outcomes over decompression alone in patients without spondylolisthesis — an important finding that has shaped modern surgical decision-making.
Minimally invasive spine surgery (MISS) approaches accomplish the same decompression through smaller incisions using specialized retractors and endoscopic or microscopic visualization. Advantages include less blood loss, shorter hospital stays, faster recovery, and less damage to the paraspinal muscles. MISS techniques are increasingly favored for straightforward single-level stenosis in appropriate candidates.
Laminoplasty is used specifically for cervical stenosis. Instead of removing the lamina entirely, the surgeon cuts it open on one side and props it open like a hinge, enlarging the canal without destabilizing the cervical spine. This preserves more of the posterior spinal structures and avoids the need for fusion in many cases.
The MILD procedure (minimally invasive lumbar decompression) is a percutaneous (through-the-skin) outpatient procedure developed specifically for lumbar stenosis caused by thickened ligamentum flavum. A small device is inserted through the skin and used to remove portions of the overgrown ligament and bone from the back of the spinal canal. MILD requires no general anesthesia, leaves no implants, and does not prevent future surgery if needed. Clinical trials (PMID 21289521 and follow-up data) have shown meaningful improvements in walking tolerance and pain at 2-year follow-up. It is best suited for patients with predominantly ligamentum flavum-driven stenosis who are poor surgical candidates.
Interspinous spacer devices (such as the X-STOP) are implants placed between the spinous processes — the bony projections at the back of each vertebra — to hold the spine in slight flexion, mechanically opening the canal at the treated level. They can be placed under local anesthesia and are removable. However, long-term data showed higher reoperation rates compared to standard laminectomy in some studies, limiting their adoption.
Surgical outcomes are generally good for well-selected patients. Most studies report that 70–80% of patients achieve significant improvement in leg pain and walking capacity. Success rates are higher for lumbar than cervical surgery, and for patients without complex degenerative changes or prior spine surgery. Age alone is not a contraindication — appropriately selected octogenarians can achieve good outcomes with careful perioperative management.
Complications and Prognosis
The natural history of spinal stenosis is highly variable. Unlike some progressive neurological conditions, lumbar stenosis does not inevitably worsen over time. Multiple long-term follow-up studies show that approximately one-third of untreated patients improve, one-third stay the same, and one-third worsen over periods of 3–5 years. This variability makes it difficult to predict who will need surgery and when.
Spontaneous improvement is more common than many patients expect and may result from changes in posture habits, natural anti-inflammatory processes, or modest remodeling of soft tissue around the canal. Patients who start with mild to moderate symptoms and who engage actively in physical therapy and lifestyle modification have the best chance of sustained non-operative improvement.
Without treatment, severely symptomatic patients — those who cannot walk more than a block or who have significant neurological deficits — are unlikely to improve spontaneously and generally benefit from surgical intervention. Prolonged nerve compression can lead to permanent nerve damage, meaning there is a window of opportunity before irreversible deficits develop.
Surgical complications include infection (1–2%), bleeding, dural tear (inadvertent puncture of the membrane surrounding the spinal fluid, occurring in 3–5% of cases), nerve injury, failed back syndrome (persistent pain after technically successful surgery), and adjacent segment disease (accelerated degeneration above or below a fusion). Perioperative medical complications — cardiac events, pneumonia, deep vein thrombosis — are of particular concern in older patients undergoing longer fusion procedures.
Reoperation rates are a concern after lumbar surgery. Studies suggest that 15–20% of patients require a second surgery within 10 years due to recurrent stenosis at the treated level, adjacent segment disease, or hardware failure in fusion cases. Minimizing fusion extent — only fusing unstable levels — reduces but does not eliminate this risk.
Cervical myelopathy carries a more guarded prognosis without surgery. Many patients with myelopathy experience a stepwise decline — periods of stability punctuated by acute worsening, often triggered by minor trauma. Once significant cord damage has occurred, recovery is partial at best. Surgery for cervical myelopathy stabilizes or partially reverses deficits in most cases but rarely restores full baseline function when cord damage is advanced.
Living With Spinal Stenosis
Most people with spinal stenosis live full lives with the condition, particularly when they learn to manage their symptoms proactively. Understanding the positional nature of the pain — that bending forward helps and straightening up hurts — empowers patients to adapt their daily activities intelligently.
Adaptive strategies for daily life: Use a shopping cart or walking poles when walking long distances. Sit and rest briefly before symptoms peak rather than waiting until pain forces a stop — this "interval walking" technique extends total daily walking distance significantly. Choose a chair or car seat that supports a slightly reclined position to take pressure off the lumbar spine. Sleep with a pillow between the knees when on your side, or with pillows under the knees when on your back, to maintain a natural lumbar flexion.
Ergonomic modifications: Raise the height of work surfaces to avoid prolonged bending (which is fine for stenosis) versus prolonged standing in extension (which is not). Use a recliner or adjustable chair rather than a hard upright chair. Install grab bars in the bathroom if balance is affected. Consider a raised toilet seat if getting up from low positions is painful.
Staying active is critical. Deconditioning — the muscle weakness and cardiovascular decline that comes from inactivity — dramatically worsens the functional impact of stenosis. Patients who remain as active as possible within their tolerance consistently report better outcomes than those who rest and avoid activity. Aquatic exercise and stationary cycling allow meaningful aerobic activity even when walking is limited.
Mental health and pain management: Chronic pain from spinal stenosis takes a significant toll on mental health. Depression and anxiety are common companions to chronic musculoskeletal conditions and directly amplify pain perception through central sensitization mechanisms. Cognitive behavioral therapy (CBT) for pain has strong evidence and should be considered part of comprehensive management. Mindfulness meditation and stress reduction techniques also reduce the suffering component of chronic pain without any side effect risk.
Planning for bad days: Stenosis symptoms often fluctuate. Having a clear plan for flares — knowing which medications to use, how to modify activity, when to call the doctor — reduces the anxiety that frequently accompanies unpredictable pain episodes. Keeping a symptom diary can help identify specific triggers (long car rides, cold weather, certain activities) and inform treatment adjustments.
Communication with your healthcare team: Stenosislive is a condition where patient-reported symptoms drive treatment more than imaging findings. Being specific about symptom progression — can you walk less than before? are your hands becoming weaker? do you have any new bladder urgency? — helps your physician accurately gauge whether the situation is stable or deteriorating and adjust the treatment plan accordingly.
Key Research Papers
- Search PubMed
- Search PubMed
- Forsth P et al., 2016 — A randomized, controlled trial of fusion surgery for lumbar spinal stenosis. Swedish Spinal Stenosis Study. N Engl J Med. PMID: 27074066
- Search PubMed
- Search PubMed
- Search PubMed
- Search PubMed
- Search PubMed
- Search PubMed
- Search PubMed
- Search PubMed
- Search PubMed
Connections
- Orthopedics
- Herniated Disc
- Low Back Pain
- Sciatica
- Scoliosis
- Fibromyalgia
- Osteoarthritis
- Osteoporosis
- Calcium
- Magnesium
- Vitamin D3
- Collagen
- Vitamin C
- Turmeric (Curcumin)
- Carpal Tunnel Syndrome