Low Back Pain
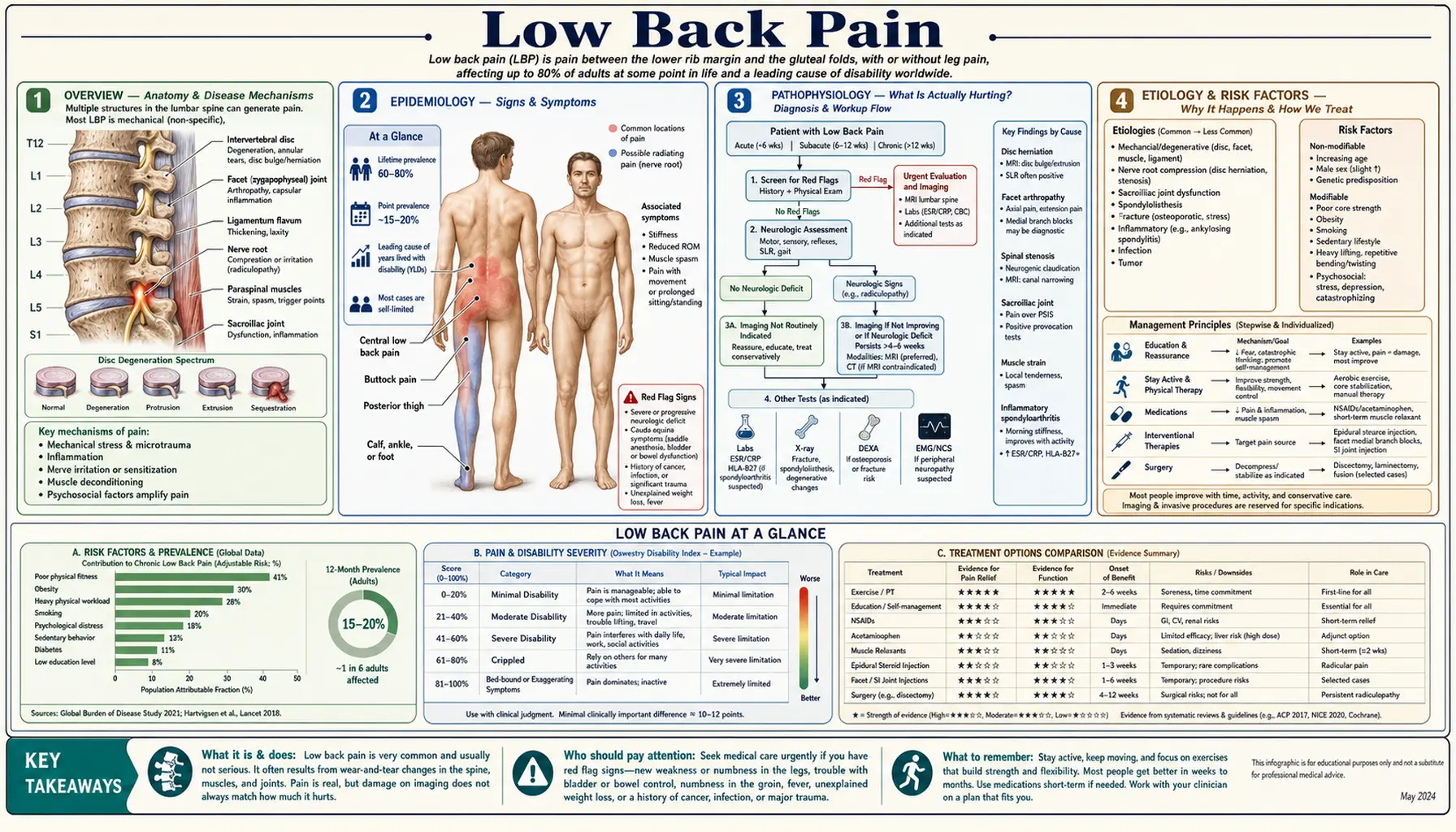
Table of Contents
- Overview
- Epidemiology
- Pathophysiology
- Etiology and Risk Factors
- Clinical Presentation
- Diagnosis
- Treatment
- Complications
- Prognosis
- Prevention
- Recent Research and Advances
- References & Research
- Research Papers
- Connections
- Featured Videos
1. Overview
Low back pain is pain felt anywhere in the area between the bottom of your rib cage and the top of your buttocks (the lumbar region). It is one of the most ordinary experiences in human life: roughly 80% of people will have at least one episode of meaningful low back pain at some point. Globally, low back pain is the single leading cause of disability — it puts more people out of work and out of normal activity than any other health condition on Earth. If your back is hurting right now, you are not unusual, you are not broken, and you are in extremely good company.
Here is the single most important message on this page, and it is genuinely good news: about 90% of acute low back pain is "non-specific." "Non-specific" means there is no dangerous underlying cause and no single damaged structure that an X-ray or MRI can pinpoint as the culprit. It is the back's version of a sprained ankle or a tension headache — uncomfortable, sometimes severe, but not a sign that something is seriously wrong. The overwhelming majority of these episodes improve substantially within a few weeks, often on their own, regardless of which treatment you try. Knowing this changes how you should respond: less fear, less rushing for scans, more gentle movement.
This page is built around that reality. It explains what is actually going on in a typical aching back, why the pain frequently has little to do with what shows up on imaging, the small set of red-flag symptoms that genuinely require urgent medical attention (and which you should know cold), and the modern, evidence-based approach to care — which often flips the old advice on its head. The old rule was "rest your back." The new rule, backed by decades of trials, is closer to "keep moving, stay calm, and let it heal."
2. Epidemiology
Low back pain is staggeringly common. The lifetime prevalence — the chance you will experience it at least once — is estimated at 70-85% across populations. At any given moment, roughly one in twelve people worldwide is dealing with activity-limiting low back pain. In 2020, an estimated 619 million people globally were living with low back pain, and that number is projected to rise to 843 million by 2050 as populations age and grow.
The disability burden is what makes low back pain stand out. In the Global Burden of Disease studies, low back pain consistently ranks as the number one cause of years lived with disability across nearly every country and income level. It is the most common reason people miss work and one of the most common reasons for primary-care visits. Importantly, this enormous burden comes almost entirely from ordinary, non-specific back pain — not from serious spinal disease.
Low back pain becomes more common with age, peaking in middle age (around 40-69 years), and is somewhat more prevalent in women. It affects people in physically demanding jobs and people sitting at desks alike. While most episodes settle, a meaningful minority of people develop recurrent or chronic pain, and it is this group that accounts for the bulk of long-term disability and healthcare cost. Crucially, the strongest predictors of who ends up with chronic disability are often not the severity of any structural finding — they are factors like distress, fear of movement, and prior pain episodes.
3. Pathophysiology — What Is Actually Hurting?
The lumbar spine is a beautifully engineered, robust structure: five stacked vertebrae cushioned by shock-absorbing intervertebral discs, stabilized by strong ligaments, hinged at the back by paired facet joints, and surrounded and powered by large muscles. In a typical episode of non-specific low back pain, the pain can arise from any of these tissues — a strained muscle, an irritated ligament, an inflamed facet joint, or a sensitized disc. Often the exact tissue cannot be identified, and that is completely fine, because for everyday back pain it does not change the treatment.
This brings us to one of the most important and most reassuring facts in all of spine medicine, and it deserves to be stated plainly: pain frequently does not correlate with what shows up on imaging. The "wear and tear" findings that get blamed for back pain — disc bulges, disc degeneration, disc protrusions, facet arthritis, even disc dehydration ("black disc") — are extraordinarily common in people who feel completely fine and have no pain at all.
In a landmark 2015 systematic review, Brinjikji and colleagues pooled imaging studies of pain-free adults and found that these "abnormalities" are essentially a normal part of aging:
- Disc degeneration was present in 37% of pain-free 20-year-olds and 96% of pain-free 80-year-olds.
- Disc bulges appeared in 30% of pain-free 20-year-olds, rising to 84% by age 80.
- Disc protrusions were seen in 29% of pain-free 20-year-olds and 43% of pain-free 80-year-olds.
Read that again. A disc bulge on your MRI is, statistically, about as meaningful as a gray hair — it is a normal age-related finding that the majority of symptom-free people your age also have. So when a scan report uses alarming words like "degeneration," "bulging disc," or "annular fissure," it does not mean your spine is crumbling, and it usually does not explain your pain. This single insight defuses an enormous amount of unnecessary fear, fragility, and the belief that one's back is "ruined."
A modern, accurate way to think about persistent back pain is that the nervous system itself becomes more sensitive over time — the pain "volume knob" gets turned up — so the back can keep hurting even after any original tissue irritation has healed. This is real pain (it is not "in your head"), but it means the path back to comfort runs through calming and retraining the system with gradual movement, not through hunting for a structural villain to cut out.
It is worth naming the specific tissues that can generate pain, simply so the words on a scan report or in a doctor's note feel less mysterious:
- Muscles and their attachments can fatigue, knot, or go into protective spasm. Spasm is intensely painful but completely benign and self-limited — it is your back guarding itself, not tearing.
- Ligaments that bind the vertebrae can be strained by an awkward movement, much like a sprained ankle.
- Intervertebral discs have nerve endings in their outer rim and can become a pain source ("discogenic pain"), but, as the Brinjikji data show, a degenerated or bulging disc is far more often silent than symptomatic.
- Facet joints — the small paired joints at the back of each spinal segment — can become irritated like any other arthritic joint, often causing pain that is worse with leaning back.
For everyday non-specific pain, the practical point is that you do not need to know which of these is the culprit. The treatment — stay active, use heat, give it time — is the same regardless, which is exactly why chasing a precise structural diagnosis with scans usually does more harm than good.
4. Etiology and Risk Factors
It helps to separate the rare specific causes from the common non-specific ones.
Non-specific low back pain (~90% of acute cases)
No single dangerous cause; pain from muscles, ligaments, discs, or facet joints that cannot be (and need not be) precisely localized. This is the default and the good-news category.
Specific structural causes (a minority)
- Radicular pain / sciatica: a herniated disc or other process compressing or irritating a nerve root, causing pain that radiates down the leg (see Sciatica and Herniated Disc).
- Spinal stenosis: age-related narrowing of the spinal canal, typically causing leg pain and heaviness when walking that eases when sitting or bending forward.
- Vertebral compression fracture: usually from osteoporosis, sometimes with minimal or no trauma in older adults.
- Inflammatory back pain: conditions like ankylosing spondylitis, suggested by morning stiffness lasting over an hour, pain that improves with activity, and onset before age 45.
- Serious causes (rare): infection, tumor/metastasis, or cauda equina syndrome — these are what the red flags below are designed to catch.
Risk factors for developing or prolonging back pain
- Previous episodes of low back pain (the strongest single predictor of a future one).
- Physical inactivity and low fitness, as well as the opposite extreme — heavy repetitive lifting and whole-body vibration.
- Excess body weight (see Obesity) and smoking.
- Psychosocial factors — and these matter enormously: depression, anxiety, high stress, job dissatisfaction, fear of movement, and the belief that the pain signals serious damage. These are among the most powerful predictors of whether acute pain becomes chronic, often outweighing any imaging finding.
5. Clinical Presentation
Most low back pain is a dull, aching, or stiff sensation across the lower back, sometimes spreading into the buttocks or upper thighs. It may flare after a specific movement (bending, lifting, a sudden twist) or arrive for no clear reason at all — both are normal. It can be sharp, it can take your breath away, and it can be genuinely frightening, but severity of pain does not equal severity of damage. A muscle spasm can be agonizing yet completely benign.
Acute vs. chronic
- Acute: lasts less than 6 weeks. The vast majority improve substantially in this window.
- Subacute: 6-12 weeks.
- Chronic: lasts more than 12 weeks. A minority of episodes reach this stage, and they call for a broader, whole-person approach.
Axial vs. radicular
- Axial (mechanical) pain stays in the back itself. This is the common, non-specific kind.
- Radicular pain (sciatica) shoots down the leg, often below the knee, sometimes with numbness, tingling, or weakness, because a nerve root is irritated — most often by a herniated disc. Even most sciatica improves over weeks without surgery (see Sciatica).
Red flags — when back pain is an emergency or needs prompt evaluation
This is the part to read carefully and remember. Red flags are uncommon, but they are the symptoms that turn "ordinary back pain" into "see a doctor now." If you do not have any of these, you almost certainly have non-specific back pain and do not need an urgent scan.
Go to the emergency room immediately — this can be cauda equina syndrome, a true emergency in which compressed nerves can cause permanent damage within hours:
- Saddle numbness — loss of feeling in the area that would touch a saddle (genitals, buttocks, inner thighs).
- New loss of bladder or bowel control — incontinence, or being unable to urinate or feel the urge.
- Weakness in both legs, or rapidly worsening leg weakness.
- New erectile dysfunction together with back pain and any of the above.
Seek prompt (same-day to within-days) medical evaluation if back pain comes with any of these:
- Fever, chills, or recent infection, or injection drug use (risk of spinal infection).
- History of cancer, or unexplained weight loss (risk of spinal metastasis).
- Significant trauma — a fall or accident — especially in older adults or anyone with osteoporosis (risk of fracture).
- Age extremes: a first episode of significant back pain before age 20 or after age 50, which slightly raises the odds of a specific cause.
- Progressive neurological deficit — worsening numbness, tingling, or weakness in a leg or foot.
- Pain that is constant, unrelenting, worse at night, or not relieved by any position or rest, or use of long-term steroids.
That is the whole list worth memorizing. If none of it applies, the most evidence-based thing you can do is take a breath, stay gently active, and let time do most of the work.
6. Diagnosis
For typical low back pain, diagnosis is built almost entirely from a history and physical exam — not from a scan. The clinician's main job is to sort your pain into one of three buckets: (1) non-specific (the common, benign kind), (2) radicular (nerve-root involvement / sciatica), or (3) a possible serious cause flagged by one of the red flags above. The exam checks how you move, your reflexes, strength, and sensation in the legs, and specific maneuvers (like the straight-leg raise) that suggest nerve involvement.
Why routine imaging is harmful for typical acute back pain
It feels intuitive that an X-ray or MRI would help "find out what's wrong." For ordinary back pain without red flags, the evidence is clear and counterintuitive: early imaging does not help, and it tends to make things worse. This is one of the most thoroughly studied recommendations in medicine, and the American College of Physicians and the Choosing Wisely campaign both explicitly advise against imaging for low back pain in the first six weeks unless red flags are present. Here is why:
- No better outcomes. Randomized trials and a large meta-analysis (Chou et al., Lancet 2009) show that patients imaged early do not recover faster or have less pain than those who are not — their pain, function, and quality of life are the same.
- Incidentalomas everywhere. Because disc bulges and degeneration are normal (see Brinjikji above), a scan will almost always find something. These harmless findings get labeled as "the cause," which frightens patients and can make pain worse.
- It snowballs into more procedures. Early imaging is associated with more specialist referrals, more injections, and more surgery — and, in studies, with worse outcomes and higher costs, not better.
- Radiation and cost. CT and X-ray expose you to radiation for no benefit, and the workup is expensive.
So the rule is simple: image only if there is a red flag, a clear neurological problem, or pain that persists despite weeks of good conservative care. Declining an early scan for ordinary back pain is not your doctor cutting corners — it is them following the best evidence and protecting you from harm.
7. Treatment
Modern, evidence-based care for low back pain overturns a lot of old advice. The framework comes largely from the 2017 American College of Physicians (ACP) guideline and the 2018 Lancet low back pain series. The headline: start with non-drug, active approaches; use medications sparingly and modestly; avoid the things that don't work or cause harm.
The single most important treatment: stay active
The old prescription — "go to bed and rest your back" — is now known to be harmful. Bed rest delays recovery, weakens muscles, and worsens mood. The evidence-based instruction is the opposite: stay as active as your pain allows, and return to normal activities as soon as you can. Movement is not dangerous for a non-specific sore back — it is the treatment. Reassurance and education on this point are themselves a proven therapy, because reducing fear speeds recovery.
First-line non-drug therapies (ACP)
For acute and subacute back pain, the ACP recommends starting with non-drug care: superficial heat (good evidence), massage, acupuncture, or spinal manipulation, along with reassurance and staying active. Most acute pain improves on its own, so the goal is comfort and confidence while nature heals it.
For chronic low back pain, the ACP recommends non-drug therapy first, with the best-supported options being:
- Exercise of essentially any kind — the most consistently supported treatment, including general activity and core/back exercise (see Exercise).
- Physical therapy and structured rehabilitation.
- Yoga and tai chi.
- Mind-body approaches: cognitive behavioral therapy (CBT), mindfulness-based stress reduction, and progressive relaxation (see Meditation).
- Spinal manipulation, massage, and acupuncture — each helps some people, with generally small to moderate benefits.
Honest framing: none of these is a miracle. The benefits are real but typically modest, and they work best as part of an active, engaged approach rather than something done to you while you stay passive.
Medications — what helps, what doesn't, and what to avoid
- NSAIDs (ibuprofen, naproxen) are the recommended first-line medication when one is needed. The benefit over placebo is modest (Machado 2017), and they carry stomach, kidney, and cardiovascular risks, so use the lowest effective dose for the shortest time.
- Acetaminophen (paracetamol) is, surprisingly, no better than placebo for low back pain. A landmark Lancet trial (Williams 2014) found it did not speed recovery from acute back pain at all. It is not a recommended primary treatment for this condition.
- Muscle relaxants can give short-term relief of acute pain but cause drowsiness; use briefly if at all.
- Opioids should be avoided. This is emphatic and evidence-based. A major randomized trial (Krebs, JAMA 2018) found opioids did not improve back-pain-related function compared with non-opioid medications — and they carry serious risks of dependence, overdose, and worsening pain over time. The harms outweigh the limited benefit.
- Duloxetine (an SNRI antidepressant) has modest evidence for chronic low back pain and is an option when first-line measures fall short.
What is overused
- Spinal injections (epidural steroids) have limited and short-lived benefit, mostly for radicular leg pain, and little role for ordinary axial back pain.
- Surgery has a place for specific indications — cauda equina, progressive neurological deficit, or persistent severe sciatica from a confirmed herniation — but it is not a treatment for non-specific low back pain. Fusion surgery for ordinary back pain has disappointing results and should be approached with great caution.
A practical first-week plan for ordinary back pain
If you have a fresh, painful back with no red flags, here is a sensible, evidence-aligned approach you can start today:
- Keep moving within comfort. Take short, frequent walks. Do not go to bed to "rest the injury" — gentle motion is the medicine.
- Use heat. A heating pad or warm bath relaxes muscle guarding and has real evidence behind it for acute pain.
- Stay calm and trust the timeline. Remind yourself this is almost certainly non-specific and the great majority of episodes settle within weeks.
- Use medication minimally if needed. A short course of an NSAID like ibuprofen, at the lowest dose that helps, is reasonable if you have no contraindication.
- Resume normal activity progressively. Aim to be back to your usual routine as soon as you reasonably can, nudging the boundary a little each day.
- Seek care if a red flag appears, if pain is not improving at all after several weeks, or if you simply want reassurance and guidance on activity.
In short: most people get better with reassurance, movement, heat, and time. Reserve scans, injections, and surgery for the minority who truly need them.
8. Complications
The most consequential "complication" of low back pain is not structural — it is the transition from a brief, self-limited episode into chronic pain and disability. A small fraction of people get caught in a cycle where pain leads to fear, fear leads to avoiding movement and activity, avoidance leads to deconditioning and low mood, and all of that feeds back into more pain. This is the fear-avoidance cycle, and breaking it early — with reassurance, gentle activity, and addressing distress — is one of the most important things modern care tries to do.
Other complications are largely the downstream harms of over-treatment: anxiety provoked by alarming-but-normal scan findings, side effects from medications (especially opioid dependence), and the risks and frequent disappointment of unnecessary spinal surgery. Genuine medical complications — permanent nerve damage from missed cauda equina syndrome, or untreated spinal infection or tumor — are rare and are exactly what the red-flag list exists to catch in time. Chronic low back pain also commonly travels with depression, sleep disturbance, and reduced quality of life, which is why treating the whole person matters.
9. Prognosis — Honestly Reassuring
The outlook for an episode of low back pain is genuinely good. Most acute episodes improve rapidly in the first few weeks: pain and disability typically drop sharply within about 6 weeks, with continued slower improvement after that. The majority of people are substantially better within a month or two, often without any specific treatment.
The honest nuance is that low back pain is frequently recurrent — many people will have another episode within a year. This is not a sign of failure or damage; it is simply the nature of backs, much like the occasional cold or headache. Recurrences are usually as self-limited as the first episode. A minority develop persistent pain, and for them the right framing is hopeful too: chronic back pain can almost always be improved and managed — through activity, conditioning, sleep, mood, and confidence — even when it cannot be made to vanish. The presence of "degeneration" on a scan does not doom you to a painful future, because those findings are present in countless people who feel perfectly well.
10. Prevention
When it comes to actually preventing future episodes of low back pain, the evidence points strongly to one intervention above all others.
- Exercise is the only well-supported preventive measure. A major systematic review (Steffens, JAMA Internal Medicine 2016) found that exercise — alone or combined with education — meaningfully reduces the risk of a future back-pain episode and time off work. Notably, back belts, shoe insoles, and education on their own did not prevent recurrences. The type of exercise matters less than doing it consistently: general aerobic activity, core/back strengthening, and overall fitness all help (see Exercise).
- Keep moving. Avoid prolonged sitting and prolonged bed rest; change positions often; build regular movement into your day.
- Sensible lifting mechanics. Bending the knees, keeping loads close, and avoiding twisting under load are reasonable habits — though their preventive power is modest, so don't let fear of "wrong" lifting make you avoid lifting altogether.
- Maintain a healthy weight (see Obesity), which reduces mechanical load and inflammation.
- Quit smoking. Smoking is associated with more back pain and slower healing.
- Reasonable ergonomics. A workstation that lets you move and shift posture, with support for your lower back, is helpful — but the best posture is largely the next one. Variety beats any single "perfect" position.
The unifying theme is that a strong, fit, active body — not a protected, rested, fragile one — is the best defense against back pain.
11. Recent Research and Advances
Research over the past decade has reinforced and refined the active, anti-overmedicalization approach:
- The 2018 Lancet low back pain series (Hartvigsen, Foster, Buchbinder) was a watershed, declaring that low back pain is overmedicalized worldwide and calling for a global shift away from imaging, injections, opioids, and surgery toward active, low-cost, evidence-based care. It explicitly highlighted the gap between what guidelines recommend and what patients actually receive.
- Stratified ("STarT Back") care uses a brief questionnaire to gauge a patient's risk of poor outcome — driven largely by psychosocial factors — and matches treatment intensity to that risk. Trials show this improves outcomes and reduces wasted care.
- Pain neuroscience education and CBT-based programs that teach the "hurt does not equal harm" principle and reduce fear-avoidance have growing evidence for chronic pain, consistent with the biopsychosocial model.
- Cognitive functional therapy (CFT), a personalized approach combining movement retraining with addressing beliefs and fears, has shown large, durable benefits for chronic disabling back pain in recent randomized trials.
- Research continues to push away from opioids and routine imaging and toward exercise, self-management, and addressing the psychosocial drivers of chronic pain.
The throughline of all of it: for the typical aching back, the most powerful "advanced" treatment turns out to be accurate reassurance, staying active, and not turning a normal life experience into a medical catastrophe.
12. References & Research
Historical Background
For much of the 20th century, the standard prescription for low back pain was bed rest — sometimes for weeks — combined with a search for a structural "lesion" to explain the pain. As imaging technology advanced through the 1980s and 1990s, MRI made it possible to see disc bulges and degeneration in exquisite detail, and these findings were widely blamed for pain. Two converging bodies of evidence overturned this model. First, trials showed that bed rest delayed recovery while staying active sped it up, ushering in the active-management paradigm. Second, imaging studies of pain-free volunteers — culminating in Brinjikji's 2015 synthesis — revealed that "degenerative" findings are nearly universal with age and poorly correlated with symptoms, exposing the harms of routine imaging and the overdiagnosis it drives. These insights were codified in the 2017 American College of Physicians guideline (non-drug therapy first; avoid opioids; image only with red flags) and broadcast globally by the influential 2018 Lancet low back pain series, which reframed low back pain as a largely benign, self-limited, and badly overmedicalized condition.
Key Research Papers
- GBD 2021 Low Back Pain Collaborators (Ferreira ML, et al.). Global, regional, and national burden of low back pain, 1990-2020, its attributable risk factors, and projections to 2050: a systematic analysis of the Global Burden of Disease Study 2021. The Lancet Rheumatology, 2023;5(6):e316-e329.
- Hartvigsen J, Hancock MJ, Kongsted A, et al. What low back pain is and why we need to pay attention. The Lancet, 2018;391(10137):2356-2367.
- Foster NE, Anema JR, Cherkin D, et al. Prevention and treatment of low back pain: evidence, challenges, and promising directions. The Lancet, 2018;391(10137):2368-2383.
- Maher C, Underwood M, Buchbinder R. Non-specific low back pain. The Lancet, 2017;389(10070):736-747.
- Qaseem A, Wilt TJ, McLean RM, Forciea MA. Noninvasive Treatments for Acute, Subacute, and Chronic Low Back Pain: A Clinical Practice Guideline From the American College of Physicians. Annals of Internal Medicine, 2017;166(7):514-530.
- Chou R, Deyo R, Friedly J, et al. Nonpharmacologic Therapies for Low Back Pain: A Systematic Review for an American College of Physicians Clinical Practice Guideline. Annals of Internal Medicine, 2017;166(7):493-505.
- Chou R, Deyo R, Friedly J, et al. Systemic Pharmacologic Therapies for Low Back Pain: A Systematic Review for an American College of Physicians Clinical Practice Guideline. Annals of Internal Medicine, 2017;166(7):480-492.
- Brinjikji W, Luetmer PH, Comstock B, et al. Systematic Literature Review of Imaging Features of Spinal Degeneration in Asymptomatic Populations. American Journal of Neuroradiology, 2015;36(4):811-816.
- Chou R, Fu R, Carrino JA, Deyo RA. Imaging strategies for low-back pain: systematic review and meta-analysis. The Lancet, 2009;373(9662):463-472.
- Williams CM, Maher CG, Latimer J, et al. Efficacy of paracetamol for acute low-back pain: a double-blind, randomised controlled trial. The Lancet, 2014;384(9954):1586-1596.
- Machado GC, Maher CG, Ferreira PH, et al. Non-steroidal anti-inflammatory drugs for spinal pain: a systematic review and meta-analysis. Annals of the Rheumatic Diseases, 2017;76(7):1269-1278.
- Krebs EE, Gravely A, Nugent S, et al. Effect of Opioid vs Nonopioid Medications on Pain-Related Function in Patients With Chronic Back Pain or Hip or Knee Osteoarthritis Pain (SPACE). JAMA, 2018;319(9):872-882.
- Hayden JA, van Tulder MW, Malmivaara A, Koes BW. Exercise therapy for treatment of non-specific low back pain. Cochrane Database of Systematic Reviews, 2005;(3):CD000335.
- Steffens D, Maher CG, Pereira LSM, et al. Prevention of Low Back Pain: A Systematic Review and Meta-analysis. JAMA Internal Medicine, 2016;176(2):199-208.
Research Papers
Explore the primary literature on low back pain through these curated PubMed searches. Each link opens a live, up-to-date list of peer-reviewed studies in a new tab.
- Non-specific low back pain management
- Low back pain imaging overuse
- Lumbar MRI findings in asymptomatic people
- Cauda equina syndrome and red flags
- Exercise therapy for chronic low back pain
- Cognitive behavioral therapy for low back pain
- Opioids and chronic low back pain outcomes
- Fear-avoidance model of low back pain
- Yoga and tai chi for low back pain
- Spinal manipulation for low back pain
- Biopsychosocial model of back pain
- Prevention of recurrent low back pain
Connections
- Herniated Disc — a common specific cause of radiating back and leg pain.
- Sciatica — radicular leg pain from nerve-root irritation.
- Tendinitis — another common self-limited musculoskeletal pain condition.
- Orthopedics — all musculoskeletal conditions.
- Osteoarthritis — degenerative joint changes, including the spine's facet joints.
- Osteoporosis — a cause of vertebral compression fractures.
- Ankylosing Spondylitis — inflammatory back pain to distinguish from mechanical pain.
- Fibromyalgia — widespread pain with central sensitization.
- Chronic Pain — the biopsychosocial framework that underlies persistent back pain.
- Depression — a powerful driver and companion of chronic back pain.
- Obesity — a modifiable risk factor for back pain.
- Exercise — the best-supported treatment and the only proven prevention.
- Meditation — mindfulness for pain coping and reducing fear-avoidance.