Age-Related Macular Degeneration (AMD)
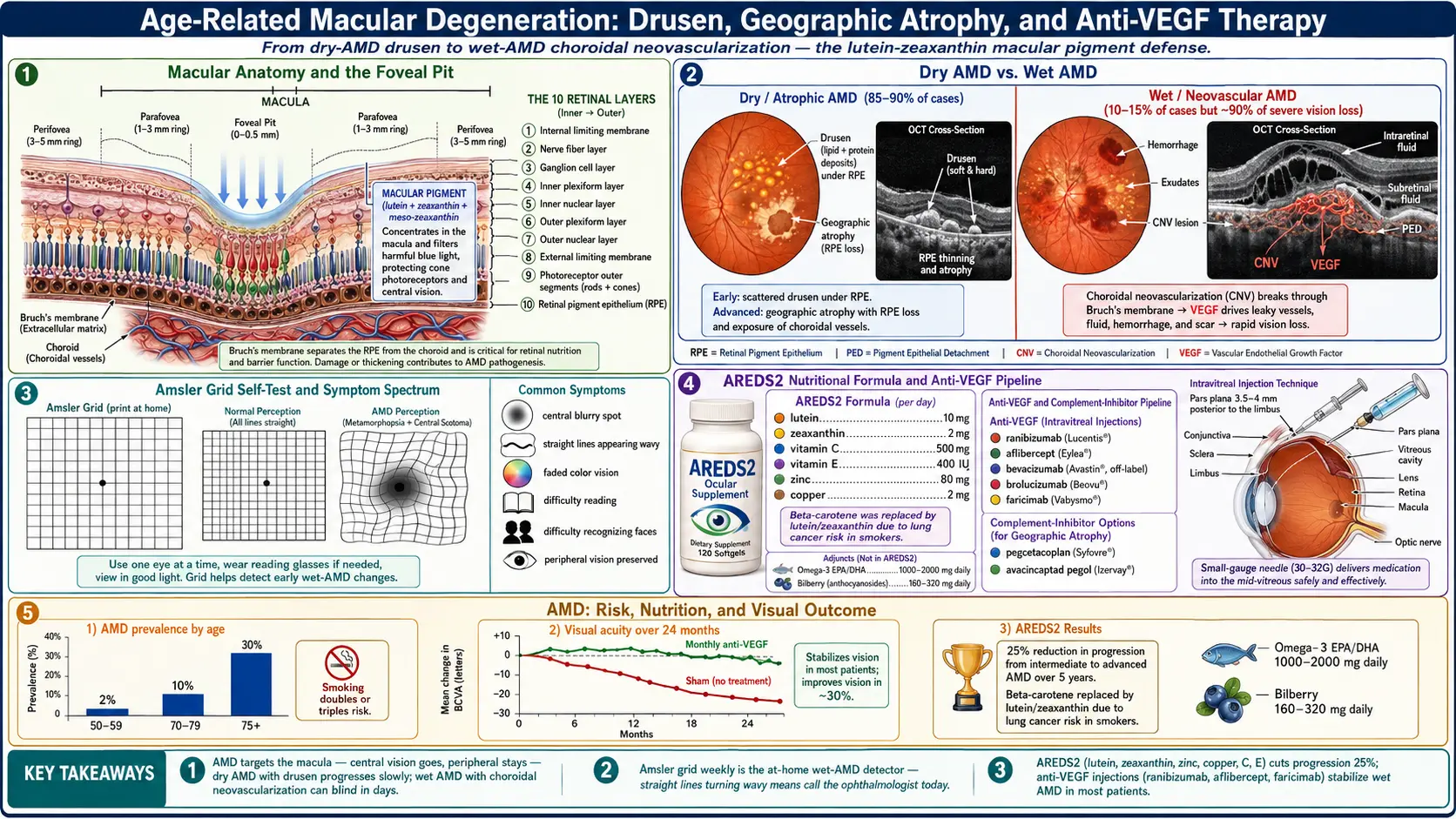
Table of Contents
- Overview
- Epidemiology
- Pathophysiology
- Genetics
- Clinical Presentation
- Diagnosis
- Treatment — Dry AMD
- Treatment — Wet AMD (Anti-VEGF)
- Complications
- Prognosis
- Prevention and Risk Reduction
- Recent Research
- References
- Connections
- Featured Videos
1. Overview
Age-Related Macular Degeneration (AMD) is the leading cause of legal blindness and irreversible central vision loss in adults over 50 years of age in the developed world. The condition affects the macula — the central 5-degree zone of the retina responsible for high-acuity vision used in reading, driving, and recognizing faces — while characteristically sparing peripheral vision and thus rarely causing complete blindness.
AMD is classified into two major forms based on the mechanism of macular damage. Geographic atrophy (dry AMD), which accounts for approximately 85–90% of all AMD cases, is characterized by the progressive atrophy of retinal pigment epithelial (RPE) cells, photoreceptors, and the choriocapillaris in the central macula, leading to slowly expanding areas of cell loss called geographic atrophy. Neovascular (wet) AMD, accounting for 10–15% of cases but responsible for approximately 90% of severe visual loss from AMD, involves the abnormal growth of fragile new blood vessels from the choroid beneath or into the retina (choroidal neovascularization, CNV), causing subretinal fluid, hemorrhage, and rapid central vision destruction.
The cardinal visual symptom of AMD is central scotoma — a blind spot or area of distorted, blurred, or absent vision in the center of the visual field — combined with metamorphopsia (distortion of straight lines and shapes) in wet AMD. Peripheral vision and the ability to navigate without assistance are typically preserved until very late disease.
2. Epidemiology
AMD is a major global public health problem with a prevalence that rises steeply with advancing age. An estimated 196 million people worldwide had AMD in 2020, a figure projected to reach 288 million by 2040 as global populations age. In the United States, approximately 8 million individuals have advanced AMD (either geographic atrophy or neovascular disease), with an additional 7–8 million at high risk due to bilateral large drusen.
Prevalence data from large population-based studies, including the Beaver Dam Eye Study (BDES) and the Blue Mountains Eye Study, demonstrate that AMD is rare before age 55 but increases sharply thereafter: approximately 2% of adults aged 50–59 have any AMD, rising to over 25% of those aged 75 and older. The BDES 15-year cumulative incidence data showed that the risk of developing any AMD over 15 years was 14.3%, with incidence of neovascular AMD increasing from 0.1% per year in the 55–64 age group to 1.5% per year after age 85.
AMD disproportionately affects white populations of European descent, who have a 2–3-fold higher prevalence of late AMD compared with Black Americans, possibly reflecting differences in macular pigment density, choroidal vascular anatomy, and genetic variant frequencies in complement pathway genes. Women have a modestly higher prevalence of late AMD than men, attributable partly to longer life expectancy. Smoking is the strongest modifiable risk factor, conferring a 2–4-fold increased risk of AMD in current smokers versus never-smokers.
3. Pathophysiology
AMD pathogenesis involves the convergence of aging, oxidative stress, complement dysregulation, lipid metabolism abnormalities, and ultimately RPE and photoreceptor cell death. The primary lesion site is the RPE–Bruch's membrane–choriocapillaris complex.
Drusen Formation
The earliest clinically visible sign of AMD is drusen — focal deposits of extracellular material accumulating between the RPE basal lamina and the inner collagenous layer of Bruch's membrane. Drusen are composed of lipids (including cholesterol esters and apolipoprotein E), complement components (C3, C5b-9, factor H, vitronectin), amyloid beta, and cellular debris from RPE turnover. Small hard drusen (<63 μm) are common with normal aging and carry low progression risk. Large soft drusen (>125 μm) with indistinct edges and drusenoid RPE detachments indicate intermediate AMD and significantly elevate the risk of progression to advanced disease.
RPE Atrophy — Dry AMD Pathway
Progressive accumulation of lipofuscin (a byproduct of incomplete lysosomal digestion of photoreceptor outer segments) within RPE cells impairs their phagocytic and metabolic function. RPE cell death initiates a cascade of overlying photoreceptor loss and choriocapillaris atrophy. The resulting confluent areas of RPE absence, visible on fundus photography as hypopigmented, sharply demarcated zones, are termed geographic atrophy (GA). GA typically begins in a perifoveal distribution and enlarges at a rate of approximately 1.5–2.5 mm² per year, eventually engulfing the fovea and causing central scotoma.
Choroidal Neovascularization — Wet AMD Pathway
In wet AMD, vascular endothelial growth factor (VEGF) — particularly VEGF-A — is upregulated by hypoxic and stressed RPE cells and drives the sprouting of new, abnormally permeable blood vessels from the choriocapillaris through defects in Bruch's membrane into the sub-RPE space (type 1 CNV) or the subretinal space (type 2 CNV). CNV vessels are leaky, causing subretinal and intraretinal fluid accumulation, RPE detachment, and subretinal hemorrhage. Without treatment, fibrovascular scarring (disciform scar) results in permanent central vision loss within 2 years in the majority of untreated eyes.
Complement Pathway Dysregulation
Genome-wide association studies have established the complement pathway as central to AMD pathogenesis. The complement factor H (CFH) Y402H polymorphism — present in approximately 30% of the general population in homozygous form — reduces CFH binding affinity for heparin and C-reactive protein on RPE cell surfaces and in Bruch's membrane, impairing the critical regulatory step that prevents uncontrolled complement activation at this site. The resulting chronic low-grade complement-mediated inflammation drives RPE cell injury, drusen formation, and progression. Other complement pathway variants (C3, C9, factor B, factor I, complement receptor 1) further illustrate the central role of dysregulated alternative pathway activity in AMD.
Oxidative Stress
The macula is the highest-oxygen-consuming region of the body per unit tissue volume, exposed to intense photic stress throughout life. RPE cells accumulate reactive oxygen species (ROS) from photoreceptor outer segment phagocytosis, light absorption, and mitochondrial metabolism. Age-related declines in antioxidant enzyme activity (superoxide dismutase, catalase, glutathione peroxidase) and in the macular pigment carotenoids lutein and zeaxanthin — which act as blue-light filters and ROS scavengers — increase oxidative damage to RPE mitochondrial DNA, membranes, and proteins, accelerating drusen formation and geographic atrophy.
4. Genetics
AMD is one of the most heritable common complex diseases, with an estimated heritability of 50–70% based on twin studies. Genetic studies have identified over 50 AMD-associated loci, but two chromosome regions account for the majority of genetic risk:
CFH Y402H — Chromosome 1q31
The single nucleotide polymorphism rs1061170 in the CFH gene (complement factor H) encoding the tyrosine-to-histidine substitution at amino acid 402 is the most strongly associated common genetic variant for AMD. Individuals homozygous for the risk allele (HH genotype) have an approximately 6–7-fold increased risk of AMD compared with homozygous non-carriers (YY), with heterozygotes (YH) showing intermediate risk (approximately 2.7-fold). CFH is the primary soluble inhibitor of the complement alternative pathway; the Y402H variant reduces its regulatory efficacy at sites of complement activation in the choroid and Bruch's membrane.
ARMS2 A69S — Chromosome 10q26
The rs10490924 variant in ARMS2 (age-related maculopathy susceptibility 2), encoding an alanine-to-serine change at codon 69, confers an approximately 3-fold increased risk per allele for advanced AMD. The functional role of ARMS2 protein — located in the outer segment of photoreceptors and implicated in mitochondrial function — remains under active investigation. The 10q26 locus also contains HTRA1 (HtrA serine peptidase 1), which modulates extracellular matrix remodeling in Bruch's membrane; variants in ARMS2 and HTRA1 are in high linkage disequilibrium and both contribute to AMD risk.
Additional Genetic Loci
Beyond CFH and ARMS2/HTRA1, multiple complement pathway genes carry AMD-associated variants: C3 (R102G), C9, CFB/C2 (on chromosome 6p21), CFI, and CFHR1/3 deletions (which are protective). Non-complement risk loci include APOE (the ε4 allele is weakly protective in AMD, in contrast to its risk role in Alzheimer's disease), COL8A1, TGFBR1, and VEGFA. Gene–environment interactions are clinically important: the CFH risk genotype amplifies smoking's effect on AMD risk, and the combination of homozygous CFH risk and ARMS2 risk genotypes confers an approximately 50-fold increased risk of advanced AMD. Genetic testing panels are now available clinically but are used primarily in research settings.
5. Clinical Presentation
Dry AMD
Early and intermediate dry AMD are often asymptomatic or cause only mild difficulty with reading in dim light or slightly reduced contrast sensitivity. On fundoscopic examination, multiple medium or large soft drusen and pigmentary changes (hyperpigmentation or hypopigmentation of the RPE) are visible in the macula. As geographic atrophy develops and enlarges toward the fovea, patients report slowly progressive central vision loss, difficulty reading fine print, and reduced ability to see in low-light conditions (rod photoreceptor dysfunction precedes cone loss in the perifoveal regions). Visual acuity may remain relatively preserved until GA involves the foveal center, at which point a dense central scotoma develops and reading without magnification becomes impossible. The clinical course is measured in years to decades.
Wet AMD
In contrast to dry AMD's gradual progression, neovascular AMD characteristically presents with sudden or rapidly worsening central vision loss occurring over days to weeks. The hallmark symptom is metamorphopsia — distortion of straight lines, which appear wavy or bowed on Amsler grid testing. Patients may notice that door frames are curved, text appears warped, or faces are distorted. A central scotoma develops as subretinal fluid and hemorrhage accumulate. Subretinal hemorrhage may cause a dense, dark central spot. Vision in dim light is disproportionately impaired due to rod dysfunction. The time to seek urgent ophthalmological evaluation is critical: anti-VEGF treatment initiated within days of symptom onset achieves better visual outcomes than treatment delayed by weeks.
Amsler Grid Self-Monitoring
The Amsler grid — a 10×10 cm grid of 5 mm squares with a central fixation dot — is the standard tool for patient self-monitoring of metamorphopsia. Patients with intermediate AMD or AMD in one eye are instructed to cover each eye alternately and observe whether the grid lines appear straight, whether the central dot is visible, and whether any lines are missing or distorted. New or worsening distortion should prompt urgent ophthalmological review. The preferential hyperacuity perimeter (PHP) is a more sensitive electronic version that detects early CNV before it becomes symptomatic.
6. Diagnosis
Slit-Lamp Biomicroscopy and Fundus Examination
Dilated fundus examination with a slit lamp and contact or condensing lens is the foundation of AMD diagnosis and staging. Characteristic findings include: drusen (categorized by size — small <63 μm, medium 63–124 μm, large ≥125 μm — and type), RPE pigmentary abnormalities, geographic atrophy (sharply defined RPE loss with visible underlying choroidal vessels), subretinal fluid, subretinal hemorrhage, and disciform scarring. The AREDS severity scale grades AMD from 1 (no AMD) through 4 (advanced AMD: geographic atrophy and/or neovascular AMD in at least one eye) based on drusen size and area and pigmentary changes.
Optical Coherence Tomography (OCT)
OCT has become the gold standard for AMD diagnosis, staging, and treatment monitoring. High-resolution cross-sectional imaging of the retina, RPE, and choroid enables detection of subretinal fluid, intraretinal fluid, drusen morphology, RPE detachments, and the presence and extent of geographic atrophy. OCT angiography (OCTA) provides non-invasive flow-based imaging of the choriocapillaris and can detect CNV without fluorescein injection. Swept-source OCT enables deeper choroidal imaging. OCT is used at every anti-VEGF injection visit to guide retreatment decisions in the treat-and-extend protocol.
Fundus Fluorescein Angiography (FFA)
Intravenous injection of sodium fluorescein with serial fundus photography delineates CNV lesion type and extent. Classic CNV appears as early, well-defined hyperfluorescence with late leakage. Occult CNV (fibrovascular RPE detachment or late leakage of undetermined source) shows a more irregular pattern. FFA is used to confirm CNV when OCT findings are ambiguous and to characterize lesion composition before planning treatment. Indocyanine green angiography (ICGA) provides superior choroidal vessel imaging and is used to detect polypoidal choroidal vasculopathy (PCV), a CNV variant more common in Asian populations.
Fundus Autofluorescence (FAF)
FAF imaging exploits the autofluorescent properties of lipofuscin in RPE cells to map RPE health across the posterior pole. Areas of geographic atrophy appear as sharply defined areas of absent autofluorescence (RPE cell loss). Increased autofluorescence at the borders of GA identifies zones of stressed RPE at greatest risk of progression — a key measure in GA clinical trials. FAF is increasingly used alongside OCT in AMD monitoring.
7. Treatment — Dry AMD
AREDS and AREDS2 Nutritional Supplementation
The Age-Related Eye Disease Study (AREDS), a randomized controlled trial enrolling 3,640 participants at high risk of advanced AMD, demonstrated that a daily supplement regimen of antioxidants (vitamins C 500 mg, E 400 IU, beta-carotene 15 mg) plus zinc (80 mg zinc oxide, 2 mg cupric oxide) reduced the risk of progression to advanced AMD by 25% over 5 years in participants with intermediate AMD or advanced AMD in one eye (odds ratio 0.72; 99% CI 0.52–0.98). The AREDS2 trial subsequently replaced beta-carotene (which increased lung cancer risk in current and former smokers) with lutein 10 mg and zeaxanthin 2 mg, achieving comparable AMD risk reduction without the lung cancer concern and with potentially superior benefit. The AREDS2 formulation is now the standard of care for secondary prevention of progression in individuals with intermediate AMD or advanced AMD in one eye — it does not treat early AMD or restore lost vision but meaningfully slows progression in the target population.
Pegcetacoplan (Syfovre) for Geographic Atrophy
Pegcetacoplan (Syfovre, Apellis Pharmaceuticals) is the first FDA-approved treatment for geographic atrophy, approved in February 2023. It is a pegylated cyclic peptide inhibitor of complement component 3 (C3) — the convergence point of all three complement activation pathways — administered by monthly or every-other-month intravitreal injection. The OAKS and DERBY phase 3 trials (PMID 36459296) enrolled 1,258 participants with GA. Monthly pegcetacoplan reduced the rate of GA lesion area growth by approximately 22% (OAKS) and 19% (DERBY) versus sham at 12 months, with monthly dosing showing greater efficacy than every-other-month dosing. At 24 months, monthly treatment showed 36% slowing of GA growth in OAKS. The primary safety concern is conversion of dry AMD to wet AMD (exudative conversion) in approximately 7–9% of treated eyes, requiring monitoring and anti-VEGF treatment if needed.
Avacincaptad Pegol (Izervay) for Geographic Atrophy
Avacincaptad pegol (Izervay, Astellas), approved by the FDA in August 2023, is a pegylated RNA aptamer inhibitor of complement component 5 (C5), administered monthly by intravitreal injection. C5 inhibition prevents formation of the membrane attack complex (C5b-9) without affecting upstream C3 function. The GATHER1 and GATHER2 trials demonstrated approximately 14–35% reduction in GA growth rate versus sham over 12 months. Exudative conversion rates were approximately 6–7% versus 3–4% in sham arms. Both pegcetacoplan and avacincaptad pegol represent the first disease-modifying treatments for geographic atrophy after decades without effective therapy.
Low Vision Rehabilitation
For patients with established central vision loss from advanced dry AMD, low vision rehabilitation — including magnifying spectacles, handheld and stand magnifiers, closed-circuit television (CCTV) magnifiers, screen-reading software, and eccentric viewing training — can significantly improve functional independence and quality of life. Referral to a low vision specialist should be made early, rather than waiting for complete foveal involvement.
8. Treatment — Wet AMD (Anti-VEGF)
Intravitreal anti-VEGF therapy is the standard of care for neovascular AMD and has transformed its prognosis from near-certain severe vision loss to vision maintenance or gain in the majority of treated patients.
Ranibizumab (Lucentis)
Ranibizumab is a humanized monoclonal antibody Fab fragment targeting all isoforms of VEGF-A, administered by monthly intravitreal injection (0.5 mg). The pivotal MARINA trial (PMID 17021309) enrolled 716 patients with minimally classic or occult CNV and demonstrated that monthly ranibizumab maintained visual acuity at 24 months in approximately 90% of patients, compared with 52% in the sham group, with 25–34% of treated patients gaining 15 or more letters. The ANCHOR trial (PMID 28375968) compared ranibizumab with photodynamic therapy (verteporfin PDT) in classic CNV, establishing ranibizumab as dramatically superior (36% of ranibizumab patients gained 15+ letters versus 6% with PDT at 12 months). These pivotal studies established intravitreal anti-VEGF as the treatment paradigm for neovascular AMD.
Aflibercept (Eylea)
Aflibercept (VEGF Trap-Eye) is a recombinant fusion protein combining the binding domains of VEGF receptors 1 and 2 with the Fc region of IgG1, providing high-affinity binding to VEGF-A, VEGF-B, and placental growth factor (PlGF). The VIEW 1 and VIEW 2 trials (PMID 22156682) enrolled 2,457 patients across the United States and internationally, demonstrating that aflibercept administered every 8 weeks after three monthly loading doses was non-inferior to monthly ranibizumab for visual acuity maintenance at 52 weeks (approximately 95% of patients maintaining vision in all active treatment groups). Every-8-week dosing reduces the injection burden compared with monthly ranibizumab while maintaining comparable efficacy — a clinically meaningful advantage for patients and healthcare systems. High-dose aflibercept (8 mg) has subsequently demonstrated extended durability in phase 3 trials.
Brolucizumab (Beovu)
Brolucizumab is a single-chain antibody fragment (scFv) with high molar concentration per injection (6 mg) that enables every-12-week dosing in a majority of patients after three monthly loading doses. The HAWK and HARRIER trials demonstrated that approximately 50–56% of brolucizumab-treated patients were maintained on a 12-week injection interval without disease activity. Brolucizumab achieved superior central subfield thickness reduction versus aflibercept. However, postmarketing surveillance identified intraocular inflammation (IOI) and retinal vasculitis/occlusion as uncommon but vision-threatening adverse events (incidence approximately 3–4% IOI, 0.7% retinal vascular occlusion), requiring careful patient selection and monitoring.
Faricimab (Vabysmo)
Faricimab (Vabysmo, Roche/Genentech) is the first bispecific antibody for neovascular AMD, simultaneously inhibiting VEGF-A and angiopoietin-2 (Ang-2). Ang-2 destabilizes vessel walls and promotes CNV formation independently of VEGF; dual inhibition addresses both pathogenic mechanisms. The Tenaya and Lucerne trials (PMID 35303425) enrolled 1,329 patients and demonstrated non-inferiority to aflibercept at 48 weeks, with approximately 45% of faricimab-treated patients qualifying for every-16-week dosing — the longest approved anti-VEGF injection interval, representing a major advance in reducing treatment burden. Faricimab received FDA approval in January 2022.
Treat-and-Extend Protocol
The treat-and-extend (T&E) protocol — in which patients are treated at every visit, and the injection interval is extended in 2-week increments when disease is inactive and shortened when activity recurs — has become the dominant real-world treatment paradigm. T&E reduces total injection burden compared with fixed monthly dosing while maintaining visual outcomes comparable to fixed dosing in the ALTAIR and ARIES trials. The individualized interval cap (maximum 16 weeks for faricimab, 12 weeks for aflibercept, 8–12 weeks for ranibizumab/brolucizumab) is determined per patient based on their disease activity profile.
Port Delivery System (PDS)
The Port Delivery System with ranibizumab (Susvimo, Genentech) is a surgically implanted refillable intraocular reservoir placed in the pars plana that continuously releases ranibizumab into the vitreous. The ARCHWAY phase 3 trial demonstrated that PDS with 100 mg/mL ranibizumab refilled every 24 weeks was non-inferior to monthly intravitreal ranibizumab for visual acuity maintenance, offering dramatically reduced injection frequency. The procedure requires vitreoretinal surgery for implantation and carries implant-specific risks (conjunctival erosion, vitreous hemorrhage, endophthalmitis) that limit its use to patients with established treatment need and stable disease.
9. Complications
- Legal blindness: AMD is the leading cause of legal blindness (best-corrected visual acuity 20/200 or worse in the better eye) in adults over 50 in developed countries. Advanced bilateral disease — geographic atrophy involving both foveas or bilateral disciform scarring — results in dense central scotomas that preclude most visually demanding activities.
- Driving cessation: Loss of central visual acuity to below the legal minimum for driving forces cessation of driving, with profound impacts on independence, employment, and social participation. AMD accounts for a substantial proportion of driving cessation in older adults.
- Falls and hip fractures: Central vision loss from AMD significantly impairs depth perception and obstacle detection, increasing fall risk. Population-based studies demonstrate a 1.5–2-fold increased risk of falls and a 2-fold increased risk of hip fractures in individuals with visual impairment from AMD compared with age-matched controls with intact vision.
- Depression and social isolation: AMD has a profound impact on mental health. The prevalence of major depressive disorder in patients with AMD is approximately 30–35%, substantially higher than in age-matched controls. Loss of the ability to read, watch television, recognize faces, and engage in hobbies drives social withdrawal, loss of occupational role, and reduced quality of life.
- Reading disability: The inability to read without magnification is the most functionally limiting consequence for most patients. Even moderate central visual acuity loss (20/80–20/200) renders standard-size print illegible and forces reliance on large-print or audio materials, significantly affecting information access and independence.
- Subretinal hemorrhage (wet AMD): Large subretinal hemorrhages from ruptured CNV vessels can cause acute, severe vision loss and, if left untreated, result in permanent photoreceptor toxicity from products of hemoglobin degradation (iron, hemosiderin). Urgent anti-VEGF treatment and, in selected cases, intravitreal tissue plasminogen activator (tPA) with gas tamponade, are employed for hemorrhage displacement.
10. Prognosis
The prognosis of AMD varies markedly by subtype and treatment era. For wet AMD, the introduction of anti-VEGF therapy has fundamentally changed the natural history: with appropriate monthly or treat-and-extend anti-VEGF treatment, approximately 90–95% of patients maintain vision (defined as losing fewer than 15 ETDRS letters) at 2 years, compared with approximately 55–62% in untreated control arms in pre-anti-VEGF studies. Approximately 30–40% of treated patients gain 15 or more letters of vision. However, visual outcomes in real-world clinical practice are consistently inferior to trial outcomes due to undertreatment, missed injections, and late presentation — emphasizing the importance of treatment adherence and regular monitoring.
Long-term prognosis in wet AMD is complicated by the development of macular atrophy beneath treated CNV lesions, a process that occurs in approximately 30–50% of patients after 5 years of anti-VEGF treatment and which is not prevented by current therapies. Macular atrophy in previously treated wet AMD eyes is the dominant cause of long-term vision loss despite effective CNV control.
For geographic atrophy (dry AMD), prognosis remains guarded. Even with pegcetacoplan or avacincaptad pegol reducing GA growth rate by approximately 14–36%, the underlying disease continues to progress, and visual acuity loss is inevitable once the foveal center is involved. The benefit of complement inhibitors is primarily in delaying the rate of progression, potentially preserving central vision for additional years, rather than restoring or halting vision loss. Risk factors for rapid GA progression include larger baseline GA area, bilateral GA, multifocal GA, and the banded FAF phenotype at GA margins.
11. Prevention and Risk Reduction
- Smoking cessation: Smoking is the strongest modifiable risk factor for AMD, conferring a 2–4-fold increased risk. Former smokers retain elevated risk for up to 20 years after cessation, but cessation at any age reduces risk. Smoking cessation counseling should be integrated into all AMD risk reduction discussions.
- AREDS2 supplementation for intermediate AMD: The AREDS2 formulation (vitamin C 500 mg, vitamin E 400 IU, lutein 10 mg, zeaxanthin 2 mg, zinc 80 mg, cupric oxide 2 mg) is recommended for patients with intermediate AMD (bilateral large drusen or large drusen in one eye and any AMD in the fellow eye) or advanced AMD in one eye. It is not indicated for early AMD or for the general population without AMD.
- UV and blue-light protection: Chronic blue-light and UV exposure contributes to cumulative macular photic stress. Wearing UV-absorbing sunglasses in outdoor high-exposure conditions is a reasonable recommendation, particularly for individuals with genetic risk factors.
- Mediterranean diet: Several prospective cohort studies demonstrate that adherence to a Mediterranean dietary pattern — high in leafy green vegetables (lutein/zeaxanthin sources), colorful fruits, fish (omega-3 fatty acids), olive oil, and nuts — is associated with a reduced risk of progression to advanced AMD. The AREDS2 ancillary dietary analysis found that the highest tertile of dietary lutein/zeaxanthin intake was associated with reduced risk of neovascular AMD.
- Blood pressure and cardiovascular risk management: Hypertension is an independent risk factor for neovascular AMD, likely through effects on choroidal perfusion. Optimal blood pressure control and management of other cardiovascular risk factors supports retinal vascular health.
- Regular ophthalmological surveillance: For patients with early or intermediate AMD, regular dilated fundus examinations (annually for intermediate AMD; more frequently if progression risk is high) with OCT imaging allow early detection of conversion to neovascular AMD, when urgent anti-VEGF treatment can prevent severe vision loss. Patients with intermediate AMD should be instructed in daily Amsler grid self-monitoring.
- Avoiding beta-carotene supplements in smokers: Smokers and former smokers should use the AREDS2 formulation without beta-carotene rather than older AREDS1 formulations, due to the established risk of lung cancer with high-dose beta-carotene supplementation in smokers.
12. Recent Research
Complement inhibition for geographic atrophy: The FDA approvals of pegcetacoplan (Syfovre, February 2023) and avacincaptad pegol (Izervay, August 2023) represent the first disease-modifying treatments for GA in the history of AMD management. The OAKS and DERBY phase 3 trials (PMID 36459296) demonstrated that C3 inhibition with pegcetacoplan reduced GA area growth by 22% and 18% respectively at 12 months in monthly dosing arms. Ongoing research is focused on identifying which GA patients are most likely to benefit and whether combination complement inhibition might provide additive benefit.
Faricimab dual VEGF-A/Ang-2 inhibition: The Tenaya and Lucerne trials (PMID 35303425) established that bispecific targeting of both VEGF-A and Ang-2 with faricimab enables every-16-week dosing in approximately 45% of wet AMD patients — a major reduction in treatment burden. Angiopoietin-2 promotes vascular destabilization, endothelial permeability, and CNV formation through a VEGF-independent pathway, and its co-inhibition appears to provide more durable vessel stabilization than VEGF blockade alone.
High-dose aflibercept (Eylea HD): Aflibercept 8 mg (Eylea HD), approved in August 2023, demonstrated every-12-week and every-16-week maintenance dosing non-inferior to every-8-week standard aflibercept in the PULSAR trial, representing a further reduction in treatment burden for wet AMD patients on aflibercept therapy.
Gene therapy for neovascular AMD: AAV-based gene therapy approaches aim to convert wet AMD from a chronic injection-dependent condition to one requiring a single treatment. RGX-314 (Regenxbio) uses AAV8 to deliver a ranibizumab-like anti-VEGF transgene subretinally, enabling sustained intraocular expression. Phase 2 trials have demonstrated durable anti-VEGF protein expression and reduction in injection need over 2+ years in treated patients.
RPE cell replacement and neuroprotection: For dry AMD, investigational approaches include iPSC-derived RPE cell transplantation, visual cycle modulators (emixustat, reducing lipofuscin A2E accumulation), and subretinal gene therapy targeting RPE survival pathways. Stem cell-derived RPE transplantation has demonstrated preliminary feasibility and safety in small phase 1–2 studies, with maintenance of transplanted cell monolayer integrity by OCT in some patients.
13. References
- Age-Related Eye Disease Study Research Group, 2001 — PMID: 11594942 — A randomized, placebo-controlled clinical trial of high-dose supplementation with vitamins C and E, beta carotene, and zinc for age-related macular degeneration and vision loss: AREDS Report No. 8.
- Age-Related Eye Disease Study 2 Research Group, 2013 — PMID: 23644932 — Lutein + zeaxanthin and omega-3 fatty acids for age-related macular degeneration: the Age-Related Eye Disease Study 2 (AREDS2) randomized clinical trial.
- Search PubMed — Intravitreal aflibercept (VEGF Trap-Eye) in wet age-related macular degeneration: outcomes in the VIEW 1 and VIEW 2 trials.
- Search PubMed — Ranibizumab for neovascular age-related macular degeneration (MARINA trial).
- Search PubMed — Efficacy of every-16-week dosing of faricimab in neovascular age-related macular degeneration: Tenaya and Lucerne trials.
- Search PubMed — Complement C3 inhibitor pegcetacoplan for geographic atrophy secondary to age-related macular degeneration: a randomized phase 2 trial (OAKS/DERBY).
- Search PubMed — Fifteen-year cumulative incidence of age-related macular degeneration: the Beaver Dam Eye Study.
- Hageman GS, Anderson DH, Johnson LV, et al., 2005 — PMID: 16936263 — A common haplotype in the complement regulatory gene factor H (HF1/CFH) predisposes individuals to age-related macular degeneration.
- Search PubMed — Prevalence of age-related macular degeneration in the United States.
- Search PubMed — Understanding age-related macular degeneration (AMD): relationships between the photoreceptor/retinal pigment epithelium/Bruch's membrane/choriocapillaris complex.
- Search PubMed — Geographic atrophy: clinical features and potential therapeutic approaches.
- Search PubMed — Ranibizumab versus verteporfin for neovascular age-related macular degeneration (ANCHOR study).
Connections
- Vision & the Retina — interactive animation
- Glaucoma
- Diabetic Retinopathy
- Cataracts
- Retinal Detachment
- Type 2 Diabetes
- Hypertension
- Vitamin C
- Vitamin E
- Zinc
- Depression
- Cigarette Smoke
- Retinal Imaging