Scabies
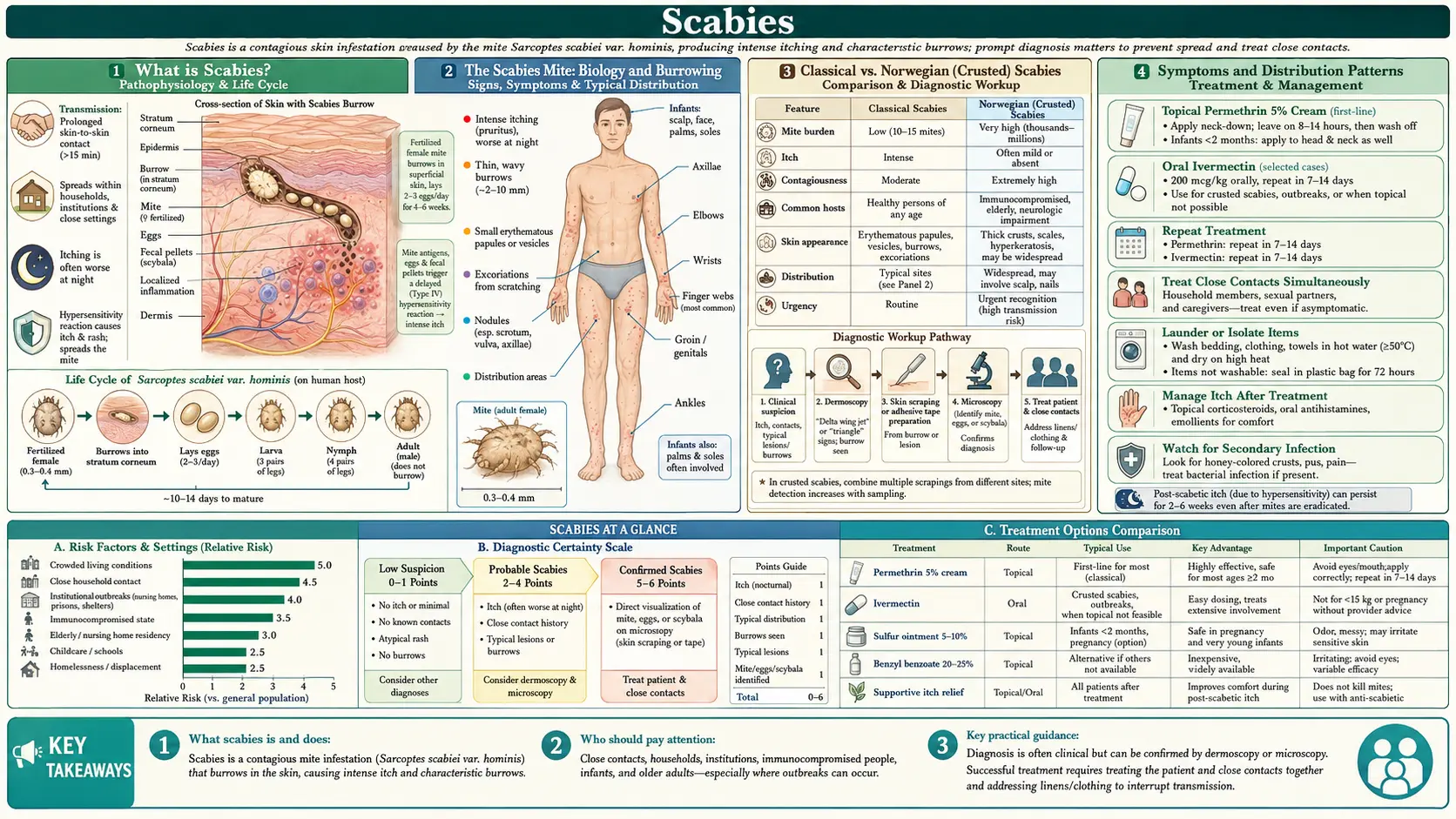
Table of Contents
- What is Scabies?
- The Scabies Mite: Biology and Burrowing
- Classical vs. Norwegian (Crusted) Scabies
- Symptoms and Distribution Patterns
- Diagnosis: Dermoscopy and Skin Scraping
- Treatment: Permethrin and Ivermectin
- Treating Household Members and Environment
- Natural and Supportive Approaches
- Complications
- Prevention and Contagion Control
- Key Research Papers
- PubMed Searches
- Connections
- Featured Videos
What is Scabies?
Scabies is a highly contagious parasitic skin infestation caused by the microscopic mite Sarcoptes scabiei var. hominis. The female mite burrows into the outermost layer of skin (stratum corneum) to lay eggs, triggering an immune reaction that causes intense, often unbearable itching. Scabies affects people of all ages, races, and socioeconomic groups and is considered a Neglected Tropical Disease by the World Health Organization, with an estimated 200–300 million cases worldwide annually.
The condition is not a sign of poor hygiene. Scabies spreads through prolonged skin-to-skin contact — it is common in households, nursing homes, prisons, and schools. Sexual transmission is a significant route in adults. The mite cannot jump or fly; it crawls at approximately 2.5 cm per minute on warm skin.
The Scabies Mite: Biology and Burrowing
- Taxonomy: Sarcoptes scabiei var. hominis; an obligate human parasite in the family Sarcoptidae. About 0.3–0.4 mm long (barely visible to the naked eye as a white dot).
- Female mite behavior: The fertilized female burrows into the stratum corneum at a rate of approximately 2 mm per day, creating a characteristic S-shaped tunnel. She lays 2–3 eggs per day and lives for 4–6 weeks on a human host.
- Eggs and lifecycle: Eggs hatch in 3–4 days into six-legged larvae, which migrate to the skin surface and molt through two nymph stages into adults within 10–15 days. Total lifecycle from egg to adult: approximately 10–17 days.
- Mite burden in typical scabies: Surprisingly low — only 10–15 mites on average in an immunocompetent person. The itching is caused largely by the host's immune response to mite saliva, feces (scybala), and shed cuticle, not by mite numbers per se.
- Survival off-host: Mites survive 24–72 hours in room-temperature conditions without human contact. Higher temperatures and lower humidity shorten survival. Mites die within 1 hour at 50°C (122°F).
- Sensitization lag: On first-ever exposure, the immune system takes 2–6 weeks to mount a response — the incubation period. During this symptom-free window, an infected person is fully contagious. On re-exposure (reinfestation in someone who has had scabies before), sensitization occurs within 1–3 days, and symptoms appear much more rapidly.
Classical vs. Norwegian (Crusted) Scabies
Classical Scabies
- Occurs in immunocompetent individuals; limited to 10–15 mites total.
- Intensely itchy; transmitted mainly by sustained skin-to-skin contact (typically >15–20 minutes).
- Responds well to standard topical treatment.
Norwegian (Crusted) Scabies
- Occurs in immunocompromised or debilitated individuals: HIV/AIDS, organ transplant recipients on immunosuppressants, elderly with dementia, leprosy patients, individuals with Down syndrome, malnutrition.
- Mite burden is massively amplified: Thousands to millions of mites (as many as 2 million reported) due to failure of the normal immune response to limit infestation.
- Appearance: Thick, gray-white, fissured hyperkeratotic crusts — particularly on hands, feet, scalp, elbows, and buttocks. Itching may paradoxically be less intense than classic scabies despite the enormous mite load.
- Extremely contagious: Even brief contact with the patient or their environment (bedding, furniture, clothing) can transmit scabies because of the massive mite shedding. Can trigger institutional outbreaks.
- Treatment: Requires combination therapy — oral ivermectin PLUS topical permethrin or benzyl benzoate, repeated over multiple weeks; keratolytic agents to remove crusts.
Symptoms and Distribution Patterns
- Intense pruritus: The hallmark symptom. Characteristically worse at night (warmth of bed increases mite activity and histamine release) and so severe it disrupts sleep. Described by patients as a "crawling" or "biting" sensation inside the skin.
- Burrows (pathognomonic sign): Small, grayish-white, slightly raised, thread-like lines 2–10 mm long. Best seen on the finger webs, wrists, and the sides of fingers. A dark dot (the mite) may be visible at the leading end with magnification.
- Papules, vesicles, and nodules: Inflammatory papules appear at burrow sites and in sensitized areas. Vesicles (tiny fluid-filled blisters) occur on palms and soles. Scabietic nodules (firm, red-brown, 5–20 mm) appear on the penis, scrotum, areolae, and axillae — these represent a hypersensitivity reaction and may persist for months after successful treatment.
- Distribution in adults: Finger webs (most specific location), wrists, elbows, axillae, periareolar area (women), genitalia (men), waistline, buttocks, and ankles. The face, neck, and scalp are usually spared in immunocompetent adults.
- Distribution in infants and young children: Different from adults — palms and soles commonly affected (vesicles and pustules); face, scalp, and neck may be involved. Nodular lesions common in diaper area.
- Excoriations and secondary changes: Intense scratching leads to crusting, lichenification, and secondary bacterial infection (impetigo, cellulitis). Postinflammatory hyperpigmentation in darker skin tones.
Diagnosis: Dermoscopy and Skin Scraping
Clinical Diagnosis
- High clinical suspicion in anyone with intractable nocturnal pruritus, characteristic distribution, and a household contact with similar symptoms. "Itch that spreads through families" is a strong historical clue.
- The burrow is pathognomonic but may be obscured by excoriations, eczematization, and secondary infection.
Dermoscopy (Dermatoscopy)
- Preferred non-invasive diagnostic tool: A handheld dermoscope (10× or higher magnification) allows visualization of the mite and burrow through the skin without sampling.
- "Delta-wing jet with contrails" sign: The darkly pigmented body and front legs of the mite (the "delta-wing") at the leading end of a white curvilinear burrow (the "contrail") is the dermoscopic signature of scabies. Sensitivity ~83%, specificity ~95% in experienced hands.
- Can be performed in seconds at the bedside — now recommended as the first-line confirmatory tool in clinical practice.
Microscopic Skin Scraping
- A mineral oil–moistened blade scrapes the roof of a burrow or papule; the material is transferred to a glass slide and examined under light microscopy (×10–40).
- Positive finding: mites, eggs, or fecal pellets (scybala) — brown oval pellets about 0.1 mm long.
- Sensitivity ~50% (many scrapes are negative even in confirmed cases); remains the gold standard for Norwegian scabies where mite density is very high.
Differential Diagnosis
- Atopic dermatitis: Similar itch distribution but lacks burrows; family history; responds to corticosteroids.
- Contact dermatitis: Localized to exposure site; dermatographism negative.
- Psoriasis: Well-demarcated plaques; silvery scale; Auspitz sign (pinpoint bleeding on scale removal).
- Lichen planus: Violaceous flat-topped papules; Wickham's striae.
- Delusions of parasitosis: Somatic symptom disorder with no mites, eggs, or burrows found on examination.
Treatment: Permethrin and Ivermectin
Permethrin 5% Cream (First-Line Topical)
- Applied from neck to toes (in children and Norwegian scabies: include face, scalp, and behind ears), left on for 8–12 hours (typically overnight), then washed off.
- Mechanism: pyrethroid insecticide that disrupts sodium channel function in mite nerve cells, causing paralysis and death.
- Repeat application in 7–14 days to kill mites that hatch from eggs laid before the first treatment (permethrin is not ovicidal).
- Cure rate: approximately 89–95% with two applications.
- Side effects: mild transient burning, stinging, or itch at application — not a sign of treatment failure. Wash hands after application.
- Safe in pregnancy and children ≥2 months old.
Oral Ivermectin (Preferred When Topicals Are Impractical or for Norwegian Scabies)
- Dose: 200 micrograms per kilogram of body weight (mcg/kg), taken on an empty stomach. Two doses, 2 weeks apart — the second dose is essential to kill mites that were eggs during the first treatment.
- Example: 70 kg adult → 14 mg (two 6 mg tablets on Day 1, repeat on Day 14).
- Mechanism: potentiates glutamate-gated chloride channels in mite neurons, causing hyperpolarization, paralysis, and death. Does not cross the human blood-brain barrier at therapeutic doses.
- Cure rate comparable to permethrin in classical scabies; combination therapy (ivermectin + permethrin) is superior for Norwegian scabies.
- Not approved for children <15 kg or pregnant women (insufficient safety data); permethrin 5% is preferred in these groups.
- Widely used in mass drug administration (MDA) campaigns for community scabies control; highly cost-effective.
Alternative Topical Agents
- Benzyl benzoate 25% lotion: Effective and cheap; widely used in developing countries; applied for 24 hours on two consecutive days; more irritating than permethrin.
- Sulfur 6–33% in petrolatum: Oldest treatment; safe in neonates and pregnancy; applied for 3 nights consecutively; messy and malodorous.
- Crotamiton 10% cream: Antipruritic and scabicidal; lower cure rate (~60%); used mainly for symptom relief post-treatment.
- Lindane 1% (gamma-benzene hexachloride): Effective but neurotoxic — banned or restricted in many countries (not recommended).
Treating Household Members and Environment
- Simultaneous treatment of all household members and close contacts is mandatory, regardless of whether they have symptoms — asymptomatic contacts in the 2–6 week incubation window are still infectious and will reinfect treated individuals if not treated at the same time.
- Clothing and bedding: Machine-wash in hot water (≥60°C/140°F) and machine-dry on high heat on the day of treatment. This kills mites that have been shed onto fabrics.
- Items that cannot be washed: Seal in a plastic bag for at least 72 hours (off-host survival time is typically <72 hours at room temperature). Leather items, stuffed animals, pillows — bag and seal for 1 week to be safe.
- Vacuuming: Vacuum upholstered furniture, car seats, and carpets to remove shed mites and skin scales. Dispose of vacuum bag immediately.
- No fumigation required for ordinary scabies; extensive environmental decontamination IS required for Norwegian scabies cases because of massive mite shedding from crusts.
- Institutional outbreaks: Notify facility management; coordinate simultaneous mass treatment of residents, staff, and family members; environmental decontamination of common areas.
Natural and Supportive Approaches
- Tea tree oil (Melaleuca alternifolia): Laboratory studies show terpinen-4-ol (the active constituent) has in vitro acaricidal and ovicidal activity against Sarcoptes scabiei. A small pilot RCT (Walton et al., 2004, PMID 15300723) found tea tree oil 5% body wash significantly reduced mite burden in a pig model of scabies and showed promise in Norwegian scabies patients. Not a replacement for permethrin or ivermectin; used as adjunct.
- Neem oil (Azadirachta indica): Traditional Ayurvedic remedy; contains azadirachtin, a limonoid with insecticidal properties. Small studies suggest potential; insufficient RCT evidence for standalone scabicidal efficacy. Used in combination with turmeric paste in some traditional settings.
- Colloidal oatmeal baths: Anti-inflammatory and anti-pruritic; provides relief from intense itching as adjunct during and after treatment. Does not kill mites.
- Antihistamines for itch relief: Oral cetirizine or loratadine reduce histamine-mediated itch during treatment. First-generation antihistamines (hydroxyzine, diphenhydramine) at night help with sleep disruption.
- Topical corticosteroids (post-treatment): Mild-potency corticosteroids (hydrocortisone 1%) help reduce post-scabetic eczematous dermatitis and nodule inflammation after mites are eradicated. Do not use before confirming successful mite eradication.
- Zinc oxide paste: Soothes excoriated skin, provides barrier protection, and has mild antiseptic properties. Useful for secondary skin breakdown from scratching.
Complications
- Secondary bacterial infection (impetigo): Staphylococcus aureus and Streptococcus pyogenes enter through excoriated skin, causing impetiginized scabies — yellow crusted lesions with purulent discharge. Requires topical mupirocin or systemic antibiotics alongside scabicidal treatment.
- Post-streptococcal glomerulonephritis: Group A Streptococcus secondary infection of scabies lesions can trigger post-infectious glomerulonephritis — a serious kidney complication with hematuria, proteinuria, and hypertension. Most prevalent in children in tropical settings with high scabies burden.
- Post-scabetic itch (post-treatment pruritus): Itch can persist for 2–4 weeks after successful mite eradication because dead mite antigens continue to stimulate the immune response. This is NOT treatment failure. Patients need reassurance and symptomatic management.
- Scabetic nodules: Firm, itchy, reddish-brown nodules on the genitalia, axillae, and areolae represent a persistent hypersensitivity reaction. May last 2–12 months post-treatment. Treated with intralesional corticosteroids (triamcinolone acetonide) if distressing.
- Treatment failure: Common reasons include under-treatment (single application of permethrin instead of two), failure to treat all contacts simultaneously, inadequate environmental decontamination, resistant mites (emerging permethrin resistance documented in some populations), and misdiagnosis.
- Psychological impact: Chronic itch, social stigma, and repeated reinfestation cause significant anxiety, embarrassment, and social isolation. Educating patients that scabies is not caused by poor hygiene is an essential part of management.
Prevention and Contagion Control
- Avoid prolonged skin-to-skin contact with an infected person until they have completed treatment. Brief handshaking carries very low transmission risk; prolonged holding of hands is a recognized route of transmission.
- Sexual partners: Always treat simultaneously; scabies is classified as a sexually transmitted infection in adults. Offer STI screening when treating scabies in sexually active adults.
- Early diagnosis: The longer scabies goes undiagnosed, the more people are exposed. Any healthcare provider evaluating an itchy rash should include scabies in the differential — especially when symptoms are bilateral and nocturnal.
- Institutional protocols: Nursing homes, prisons, refugee camps, and day-care centers should have written scabies response protocols including case identification, simultaneous mass treatment, and environmental decontamination procedures.
- Mass drug administration (MDA): WHO-endorsed ivermectin MDA in high-burden communities has dramatically reduced scabies prevalence and secondary bacterial infection rates in tropical island populations (studies from Fiji, the Solomon Islands, and northern Australia).
- Post-exposure prophylaxis: Close household contacts exposed to Norwegian scabies should receive prophylactic treatment regardless of symptoms given the massive mite burden in crusted disease.
Key Research Papers
- Chosidow O. Clinical practices. Scabies. N Engl J Med. Search PubMed
- Romani L, Steer AC, Whitfeld MJ, Kaldor JM. Prevalence of scabies and impetigo worldwide: a systematic review. Lancet Infect Dis. Search PubMed
- Strong M, Johnstone P. Interventions for treating scabies. Cochrane Database Syst Rev. Search PubMed
- Romani L, Whitfeld MJ, Koroivueta J, et al. Mass drug administration for scabies control in a population with endemic disease. N Engl J Med. 2015;373(24):2305-2313. PMID 26222556
- Walton SF, McKinnon M, Pizzutto S, et al. Acaricidal activity of Melaleuca alternifolia (tea tree) oil: in vitro sensitivity of Sarcoptes scabiei var hominis to terpinen-4-ol. Arch Dermatol. Search PubMed
- Argenziano G, Fabbrocini G, Delfino M. Epiluminescence microscopy. A new approach to in vivo detection of Sarcoptes scabiei. Arch Dermatol. Search PubMed
- Kircik LH. Ivermectin 1% cream for the treatment of head lice: now treating another parasitic infection with the same compound. J Drugs Dermatol. Search PubMed
- Aussy A, Houivet E, Hébert V, et al. Risk factors for treatment failure in scabies: a cohort study. Br J Dermatol. Search PubMed
- Johnston G, Sladden M. Scabies: diagnosis and treatment. BMJ. Search PubMed
- Hicks MI, Elston DM. Scabies. Dermatol Ther. Search PubMed
- Engelman D, Yoshizumi J, Hay RJ, et al. The 2020 International Alliance for the Control of Scabies Consensus Criteria for the Diagnosis of Scabies. Br J Dermatol. 2020;183(5):808-820. PMID 32034956
- Sunderkötter C, Aebischer A, Neufeld M, et al. Increase of scabies in Germany and development of a new fundamental principle for its control. J Dtsch Dermatol Ges. Search PubMed
PubMed Searches
Curated PubMed topic searches of peer-reviewed literature on scabies.
- PubMed: Scabies treatment permethrin vs ivermectin
- PubMed: Sarcoptes scabiei pathogenesis
- PubMed: Norwegian crusted scabies
- PubMed: Scabies mass drug administration
- PubMed: Scabies dermoscopy diagnosis
- PubMed: Scabies secondary bacterial infection
- PubMed: Scabies global epidemiology
- PubMed: Scabies tea tree oil
- PubMed: Permethrin resistance scabies
- PubMed: Scabies institutional outbreak
Connections
- Dermatology
- Eczema
- Psoriasis
- Contact Dermatitis
- Fungal Infections
- Herpes Simplex
- Urticaria (Hives)
- Warts
- Rosacea
- Zinc
- Tea Tree Oil
- Neem
- Gut Healing
- Chronic Kidney Disease
- Acne
- HIV/AIDS
- Vitamin D3
- Tea Tree Oil for Head Lice & Scabies