Brugada Syndrome
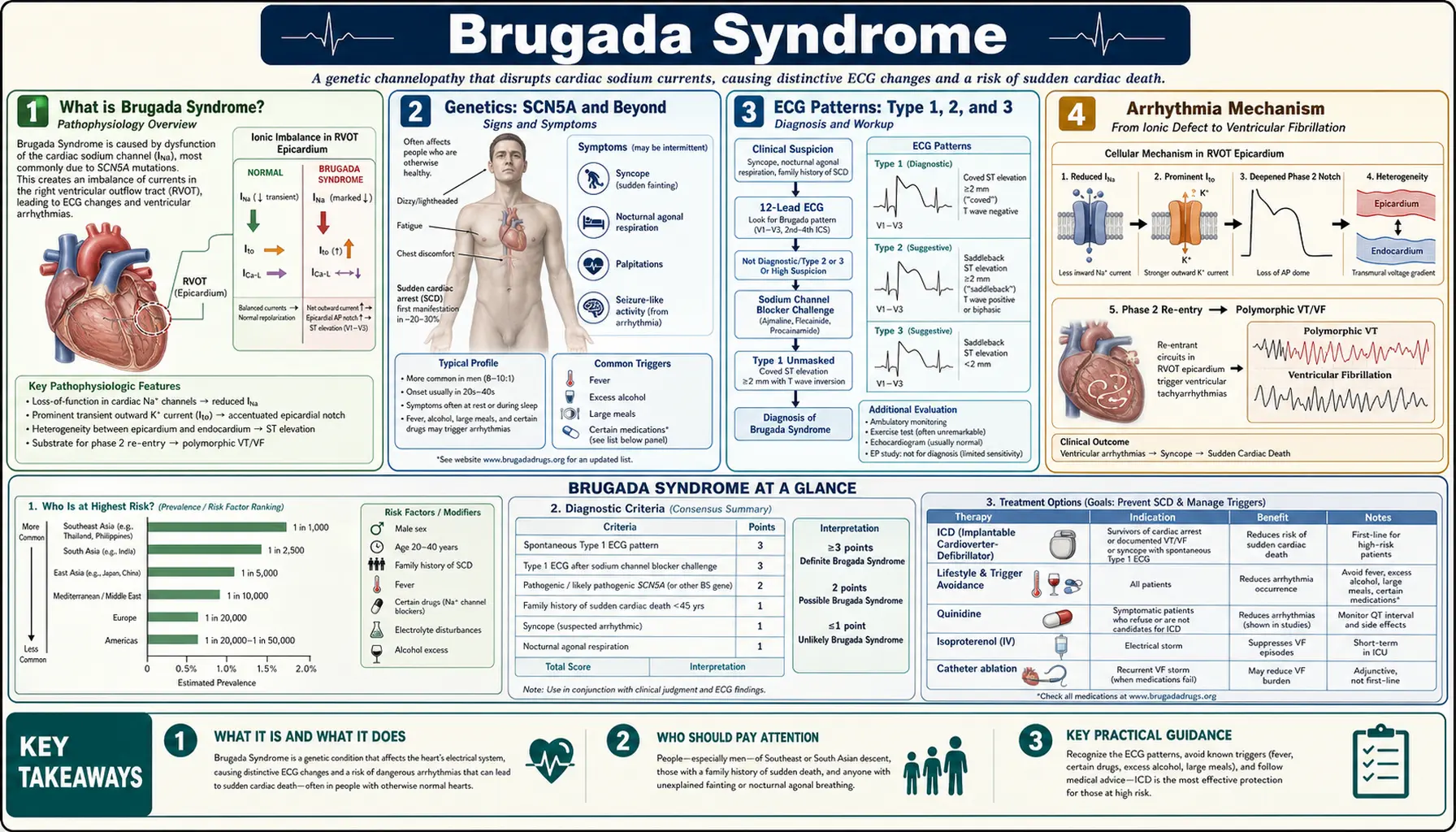
Table of Contents
- What is Brugada Syndrome?
- Genetics: SCN5A and Beyond
- ECG Patterns: Type 1, 2, and 3
- Arrhythmia Mechanism
- Diagnosis and Provocative Testing
- Risk Stratification for SCD
- Triggers and Drug Avoidance
- Treatment: ICD, Quinidine, and Ablation
- Special Populations and Fever Management
- Research Papers
- Connections
- Featured Videos
What is Brugada Syndrome?
Brugada Syndrome is an inherited cardiac channelopathy characterized by a distinctive electrocardiographic (ECG) pattern — ST-segment elevation in the right precordial leads (V1–V2) in the absence of structural heart disease — and an elevated risk of sudden cardiac death (SCD) due to ventricular fibrillation (VF). It was first described as a distinct clinical entity by Pedro and Josep Brugada in 1992.
Brugada Syndrome is estimated to account for up to 12% of all sudden cardiac deaths and up to 20% of sudden deaths in patients with structurally normal hearts. It is more common in males (8:1 male-to-female ratio) and shows higher prevalence in Southeast Asia — particularly Japan, Thailand, and the Philippines — where it is linked to a clinical syndrome known as SUDS (Sudden Unexplained Death Syndrome) or "Bangungot" (death during sleep).
The global prevalence is approximately 1–5 per 1,000 individuals, though many cases go undiagnosed because the ECG pattern is often concealed and symptoms may not occur until a life-threatening arrhythmia strikes.
Genetics: SCN5A and Beyond
Brugada Syndrome is a genetically heterogeneous disorder. The most important gene is SCN5A, encoding the cardiac sodium channel Nav1.5:
- SCN5A mutations: Found in approximately 20–30% of patients with Brugada Syndrome. More than 300 pathogenic or likely pathogenic variants have been identified, distributed throughout the gene. Mutations cause loss-of-function of the sodium channel — reduced sodium current (INa) density, accelerated inactivation, or trafficking defects.
- Inheritance: Autosomal dominant with variable penetrance and expressivity. A first-degree relative with an SCN5A mutation has a 50% chance of carrying the variant but may never manifest the ECG pattern or symptoms — particularly females, who are largely protected by higher baseline Ito (transient outward potassium current) in women.
- Other genes: Approximately 70–80% of probands have no identifiable single-gene cause. Pathogenic variants in more than 20 genes have been implicated, including CACNA1C (L-type calcium channel), CACNB2, SCN1B (sodium channel beta-subunit), KCND3 (Ito), HCN4 (funny current), and others. Most confer modest effect sizes.
- Genetic testing recommendations: Genetic testing is recommended for all probands and cascade screening for first-degree relatives. A negative genetic test does NOT exclude Brugada Syndrome — the diagnosis remains clinical/ECG-based.
ECG Patterns: Type 1, 2, and 3
The Brugada ECG pattern has three described morphologies, but only the Type 1 pattern is diagnostic:
Type 1 Brugada ECG Pattern (Coved-Type) — Diagnostic
The Type 1 pattern is the only pattern that establishes the diagnosis of Brugada Syndrome (in combination with clinical criteria). Characteristics:
- J-point elevation: ≥2 mm (0.2 mV) in one or more of leads V1–V2, positioned at the 4th intercostal space (or standard 3rd–4th ICS position).
- ST-segment morphology: Coved — the J wave forms the apex of a peaked wave that descends gradually toward the baseline, giving it a "coved" or "tombstone" appearance.
- T-wave: Inverted (negative) in V1; may be biphasic in V2.
- No terminal R' in V1: Distinguishes it from right bundle branch block (RBBB), which has a positive terminal deflection.
Type 2 (Saddle-Back Pattern)
≥2 mm J-point elevation with a saddle-back ST morphology (concave upward) and positive or biphasic T wave. NOT diagnostic of Brugada Syndrome but may convert to Type 1 with sodium channel blocker provocation. Found in healthy individuals and athletes; requires evaluation in context.
Type 3
Similar saddle-back pattern with <2 mm J-point elevation. Considered non-specific; rarely clinically relevant. No longer formally listed in current consensus recommendations as it is difficult to distinguish from normal variants.
Lead Placement
The diagnostic yield increases substantially when high right precordial leads (V1–V2 placed at the 2nd or 3rd intercostal space, one intercostal space higher than standard) are used. This modification can unmask a concealed Type 1 pattern in up to 20% of additional cases where standard placement is negative.
Arrhythmia Mechanism
Two competing but not mutually exclusive theories explain the Brugada arrhythmia mechanism:
Phase 2 Reentry (Repolarization Disorder)
The dominant hypothesis. In the right ventricular epicardium, the transient outward potassium current (Ito) is particularly prominent. Normally, the sodium current (INa) counterbalances Ito during the action potential plateau (Phase 2). When INa is reduced (by SCN5A mutation, drugs, fever, or ischemia), Ito dominates and causes early repolarization at the RV epicardium — creating a voltage gradient between epicardium (early repolarization) and endocardium (still in plateau). This transmural gradient produces the ST-segment elevation. Under certain conditions, this gradient is sufficient to re-excite the epicardium from the endocardium, generating a "Phase 2 reentry" extrasystole that can degenerate into VF.
Depolarization Disorder
An alternative hypothesis proposes that delayed conduction in the right ventricular outflow tract (RVOT) — due to reduced Na current — creates the ECG pattern and a substrate for reentrant arrhythmia. Late potentials in the RVOT seen on signal-averaged ECG and late activation on epicardial mapping support this view. The two mechanisms likely coexist.
Why Males are at Higher Risk
Males have significantly higher Ito density in the RV epicardium than females, due to androgen effects on KCND3 expression. This makes the Phase 2 repolarization imbalance more pronounced in men, explaining the 8:1 male predominance in symptomatic Brugada Syndrome.
Diagnosis and Provocative Testing
Brugada Syndrome is diagnosed when a spontaneous or drug-induced Type 1 ECG pattern is identified in a patient who:
- Has survived a resuscitated cardiac arrest (most definitive), OR
- Has documented spontaneous VT/VF, OR
- Has a first-degree relative with confirmed Brugada Syndrome or sudden death <45 years in a structurally normal heart, OR
- Has a coved-type Type 1 ECG spontaneously (without drugs) — even asymptomatic.
Structural heart disease must be excluded by echocardiography and/or cardiac MRI before attributing the pattern to Brugada Syndrome (ARVC, Brugada phenocopy from myocarditis, hyperkalemia, and other conditions can mimic the ECG).
Provocative Testing with Sodium Channel Blockers
When the baseline ECG shows a Type 2 or equivocal pattern, sodium channel blocker challenge unmasks the Type 1 Brugada pattern in susceptible individuals. Available agents:
- Ajmaline 1 mg/kg IV over 10 minutes: Highest sensitivity (~80%) and preferred in Europe. Fast onset and offset; most experience in European centers. Must be performed under continuous ECG monitoring with crash cart available.
- Flecainide 2 mg/kg IV (max 150 mg) over 10 minutes: Alternative; slightly lower sensitivity than ajmaline; longer duration of action increases monitoring period required.
- Procainamide 10 mg/kg IV: Used in some centers; lower sensitivity than ajmaline.
- Pilsicainide (Japan only): Oral sodium channel blocker used for outpatient challenge.
Contraindications to provocative testing: Spontaneous Type 1 pattern (test is not needed), QRS duration >120 ms at baseline, severe cardiac conduction disease, sinus node dysfunction, or known prior VF with induced Type 1 already documented.
A positive test (induction of Type 1 pattern) confirms Brugada Syndrome. A negative test does not exclude it — up to 20% of genotype-positive individuals have a negative ajmaline test.
Risk Stratification for SCD
Risk stratification in Brugada Syndrome — particularly for asymptomatic patients — remains one of the most challenging areas in electrophysiology. Key determinants:
Highest Risk: Prior Resuscitated Cardiac Arrest or Syncope
- Survived VF or documented VT: Annual SCD/VF recurrence rate ~10–15%/year. ICD implantation is unequivocally indicated.
- Unexplained syncope + spontaneous Type 1 ECG: Syncope is presumed arrhythmic until proven otherwise; annual event rate ~2–3%/year. ICD strongly indicated.
Intermediate Risk: Asymptomatic with Spontaneous Type 1 ECG
- Annual SCD risk approximately 0.5–1%/year in multiple registry studies.
- Electrophysiology study (EPS) with programmed electrical stimulation: inducibility of VF at EPS predicts future events in some (but not all) studies. Current guidelines suggest EPS can be considered to help guide decision-making, but it is not universally recommended.
- ICD is generally recommended for symptomatic patients with spontaneous pattern; for asymptomatic patients with spontaneous Type 1, shared decision-making is required.
Lower Risk: Drug-Induced Type 1 ECG Only (No Spontaneous Pattern)
- Annual SCD risk <0.5%/year. ICD is generally not indicated for asymptomatic drug-induced Brugada without other risk factors.
- Family history of sudden death, early repolarization on ECG in inferior leads, fragmented QRS, and SCN5A-positive status may increase risk estimates modestly.
Risk Scores
The Shanghai Score (2016 Expert Consensus) integrates ECG features, clinical history, family history, and genetic results into a points-based risk tool to guide diagnosis and management decisions. Scores ≥3.5 confirm Brugada Syndrome; lower scores classify as probable or possible.
Triggers and Drug Avoidance
Several factors unmask or exacerbate Brugada Syndrome by further reducing sodium channel function or augmenting Ito. Patients and their families must be educated about these triggers:
Fever — The Most Common Trigger
Fever is the most frequently reported trigger for Brugada-related VF events. High body temperature directly impairs Nav1.5 kinetics — accelerating inactivation and reducing peak sodium current — in a manner that synergizes with SCN5A loss-of-function mutations. Even a temperature of 38.5°C can unmask a Brugada Type 1 pattern on ECG and precipitate arrhythmia. Management: aggressive fever control with antipyretics (acetaminophen/paracetamol) for any febrile illness. Patients should go to the emergency department for ECG monitoring if they cannot control fever.
Sodium Channel Blockers (Must Avoid)
- Antiarrhythmics: Flecainide, propafenone, ajmaline, procainamide, quinidine (paradoxically, high-dose quinidine is used for treatment — see below), disopyramide.
- Tricyclic antidepressants: Amitriptyline, nortriptyline, imipramine, clomipramine — carry significant arrhythmic risk in Brugada.
- Certain antihistamines: Dimenhydrinate, promethazine.
- Local anesthetics: Bupivacaine (particularly); lidocaine (lower risk). Dentists and anesthesiologists must be informed.
- Cocaine: Strong sodium channel blocking properties; recreational use has precipitated VF in Brugada patients.
Other Triggers
- Alcohol intoxication and large meals (vagal tone increase).
- Sleep and rest states — most events occur at night during sleep, consistent with heightened vagal tone predominance.
- Hypokalemia and hyponatremia (electrolyte disturbances worsen sodium channel function).
A curated list of drugs to avoid in Brugada Syndrome is maintained at BrugadaDrugs.org — patients should consult this resource before taking any new medication and inform all healthcare providers of their diagnosis.
Treatment: ICD, Quinidine, and Ablation
Implantable Cardioverter-Defibrillator (ICD)
The ICD is the only proven intervention to reduce mortality in high-risk Brugada Syndrome. It terminates VF with an internal shock if arrhythmia occurs. Indications:
- Class I (strongly indicated): Resuscitated cardiac arrest or spontaneous sustained VT.
- Class IIa (reasonable): Spontaneous Type 1 ECG + unexplained syncope.
- Class IIb (may be considered): Asymptomatic with spontaneous Type 1 ECG + inducible VF at EPS.
The subcutaneous ICD (S-ICD) is an attractive alternative in younger patients — it avoids transvenous leads (and their long-term complications) and is preferred when pacing is not required. However, S-ICD requires careful programming to avoid T-wave oversensing on the Brugada ST pattern.
Quinidine for Electrical Storm and Prophylaxis
Quinidine is the pharmacological treatment of choice when ICD is contraindicated, declined, or supplementary therapy is needed. Mechanism: quinidine inhibits Ito (the potassium current that drives the Phase 2 repolarization imbalance), restoring the action potential plateau gradient that prevents VF.
- Electrical storm: Repeated VF episodes requiring multiple ICD shocks. IV or oral quinidine is the most effective acute pharmacological treatment for Brugada-related electrical storm (isoproterenol is also used acutely to increase heart rate and reduce Ito-mediated heterogeneity).
- Dose: Quinidine gluconate 324–648 mg twice or three times daily. QT-interval monitoring required; can cause QT prolongation and GI side effects (diarrhea, nausea).
- Availability concern: Quinidine has been intermittently subject to supply shortages in the United States — patients should maintain an adequate supply and work with their electrophysiologist if access becomes limited.
Epicardial Catheter Ablation
For patients with recurrent VF or electrical storm refractory to quinidine and/or repeated ICD shocks, epicardial ablation of the right ventricular outflow tract (RVOT) substrate has emerged as a potentially curative strategy. Targeted ablation of the abnormal fractionated late potentials in the epicardial RVOT normalizes the ECG pattern and reduces VF recurrence in experienced centers. Evidence is from case series and registries; no randomized trial data yet. Recommended at specialized electrophysiology centers with epicardial mapping expertise.
Special Populations and Fever Management
Children and Adolescents
Brugada Syndrome is rare in children but can cause unexplained sudden cardiac death in pediatric patients, particularly infants (where it may overlap with SIDS) and adolescents. Children with SCN5A-positive Brugada or spontaneous Type 1 ECG warrant cardiology referral. ICD implantation decisions are individualized; wearable defibrillator vests are an option as a bridge.
Pregnancy
Hormonal changes during pregnancy can alter sodium channel expression. Brugada Syndrome patients can have safe pregnancies with appropriate monitoring. Epidural anesthesia is generally preferred over general anesthesia to minimize sodium-channel-blocking local anesthetic exposure. Fever during delivery must be aggressively treated.
Athletes
Participation in competitive sports is controversial. Vigorous exercise can increase vagal tone post-exertion, and exercise-induced fever can unmask Brugada. Current consensus recommends individualized evaluation rather than blanket restriction. Asymptomatic patients with drug-induced pattern only may participate; those with spontaneous Type 1 pattern or ICD require multidisciplinary risk assessment.
Family Screening
All first-degree relatives (parents, siblings, children) of a proband should undergo 12-lead ECG screening, including high right precordial lead placement. Genetic counseling and testing for the proband's identified variant (if any) should be offered. Cascade screening identifies additional affected family members who may be at risk even if asymptomatic.
Research Papers
The following PubMed links return current peer-reviewed literature on Brugada Syndrome. Each opens a live reference or search.
- Search PubMed
- Search PubMed
- Search PubMed
- Search PubMed
- Search PubMed
- Search PubMed
- Search PubMed
- Search PubMed
- Search PubMed
- Search PubMed
Connections
- Cardiology
- Atrial Fibrillation
- Long QT Syndrome
- Sudden Cardiac Arrest
- Heart Failure
- Cardiomyopathy
- Cardiovascular Disease
- Coronary Artery Disease
- Hypertension
- Stroke
- Aortic Stenosis
- Electrocardiogram
- Complete Blood Count
- Potassium
- Sodium
- Magnesium
- Syncope