CoQ10 for Fertility (Male & Female)
Both sperm and oocytes are exceptionally mitochondria-rich cells whose function declines with age in significant part through accumulated mitochondrial dysfunction. CoQ10 supports the rate-limiting electron-transport step that powers sperm tail motility and oocyte meiotic spindle formation — the two energy-intensive cellular events that determine fertilization success and chromosomal segregation fidelity. The Italian Balercia trials (2004, 2009) randomized men with idiopathic asthenozoospermia to CoQ10 200-300 mg/day for 6 months and showed significant improvements in sperm motility, density, and pregnancy rates. The Bentov & Casper trials at the University of Toronto demonstrated that ubiquinol 200 mg three times daily for 60 days before IVF cycle start improved ovarian response and increased high-quality embryo yield in women of advanced reproductive age. This deep-dive walks through both bodies of evidence, the oocyte and sperm mitochondrial mechanisms, and the combination protocols (CoQ10 + zinc + selenium for male; CoQ10 + DHEA + vitamin D for female) used in modern reproductive endocrinology.
Interactive Visualization Free Radicals & Your Antioxidant Network Follow one superoxide radical down the whole relay — SOD, catalase, glutathione, vitamin E, vitamin C, NADPH — then release free iron and watch a membrane tear itself apart. Launch →
Table of Contents
- Why Reproductive Cells Are Uniquely Mitochondria-Dependent
- Sperm Mitochondria & Motility
- Oocyte Mitochondria & Reproductive Aging
- The Balercia Male-Fertility Trials
- Lafuente 2013 Male-Fertility Meta-Analysis
- The Bentov & Casper IVF Trials
- Xu 2018 — Poor Ovarian Responders
- Male Fertility Protocol
- Female Fertility Protocol
- Combination Therapy (Zinc, Selenium, DHEA, Vitamin D)
- IVF-Specific Protocols (Pretreatment Timing)
- Patient FAQ
- Cautions
- Key Research Papers
- Connections
- Featured Videos
Why Reproductive Cells Are Uniquely Mitochondria-Dependent
Both sperm and oocytes are among the most mitochondria-rich cells in the human body, but for very different reasons.
Sperm
The mature sperm cell is essentially a delivery vehicle for paternal DNA, with three functional regions: the head (carrying the chromosomal payload and the acrosome enzyme cap), the midpiece (containing 70-100 mitochondria coiled tightly around the proximal flagellum), and the tail (the flagellum that provides motility). The mitochondria in the midpiece are the sole ATP source for the dynein-driven flagellar bending that produces forward propulsion. Without continuous mitochondrial ATP supply, sperm cannot swim, and swimming is required for both natural conception (through the cervical mucus and reproductive tract) and many forms of assisted reproduction.
Sperm mitochondria are also unusual in that they encode some of their own electron-transport-chain components in mtDNA, and they generate substantial reactive oxygen species (ROS) during normal function. The membrane-bound antioxidants — particularly ubiquinol — are essential for protecting sperm membrane integrity and DNA from oxidative damage. When CoQ10 supply is inadequate, sperm motility declines and DNA fragmentation increases.
Oocytes
The mature oocyte is roughly 1000-fold larger than the average somatic cell and contains 100,000-600,000 mitochondria — orders of magnitude more than any other cell type. This massive mitochondrial endowment is necessary because the early embryo, after fertilization, inherits all of its mitochondria from the mother (paternal mitochondria are tagged for elimination shortly after fertilization). The maternal mitochondria must therefore support the first several cell divisions of the developing embryo from existing stores until the embryonic genome activates and mitochondrial biogenesis can resume.
Oocyte mitochondria face an extraordinary challenge: they must remain functional for decades. Unlike sperm, which are continuously produced from spermatogonial stem cells throughout adult male life, oocytes are formed in the female fetus before birth and remain in meiotic arrest until they are ovulated — meaning the mitochondria in a 40-year-old woman's oocytes are 40 years old. The accumulated mitochondrial DNA mutations, reduced membrane potential, and impaired ATP synthesis capacity that come with age are major contributors to the well-documented decline in oocyte quality, fertilization rates, embryo development, and live birth rates after age 35.
The most energy-intensive event in the oocyte life cycle is meiotic spindle formation during the second meiotic division at ovulation. The spindle is constructed entirely from mitochondrial ATP supply over hours; if ATP supply is inadequate, the spindle assembles improperly, chromosomes segregate incorrectly, and aneuploidy results. The age-related rise in aneuploidy (trisomies, monosomies, triploidies) that drives reduced live birth rates and increased Down syndrome risk after age 35 traces in large part to inadequate mitochondrial ATP during spindle formation.
Sperm Mitochondria & Motility
Asthenozoospermia (reduced sperm motility) accounts for 20-40% of male infertility cases. The WHO defines asthenozoospermia as <40% total motility or <32% progressive motility in a semen analysis. Idiopathic asthenozoospermia — the form without obvious anatomical, hormonal, or infectious cause — appears to involve mitochondrial dysfunction in a substantial fraction of cases.
Sperm motility depends on:
- ATP supply — the flagellum consumes ATP at high rates to power dynein arm sliding
- Membrane integrity — the midpiece mitochondrial membrane must maintain proton gradient and prevent ROS-driven membrane peroxidation
- DNA integrity — oxidative DNA damage to the paternal chromosomes reduces fertilization success and increases miscarriage risk
- Acrosome function — the enzyme cap that enables penetration of the egg's zona pellucida requires intact membrane structure to release contents at the right moment
CoQ10 supports all four through its dual role as electron carrier (driving ATP synthesis) and lipid-phase antioxidant (protecting membranes and DNA). The Italian seminal-fluid CoQ10 measurements consistently show that infertile men have lower seminal CoQ10 concentrations than fertile men, and that CoQ10 supplementation raises both seminal-fluid CoQ10 and the ratio of motile to immotile sperm.
The age decline in sperm parameters — modest compared to oocyte decline, but real — appears in part mitochondrially mediated. Men over 40 show measurable reductions in sperm motility, DNA integrity, and seminal antioxidant capacity, all consistent with cumulative mitochondrial damage. CoQ10 supplementation is therefore relevant for both younger men with idiopathic asthenozoospermia and older men experiencing age-related decline.
Oocyte Mitochondria & Reproductive Aging
The decline in oocyte quality with female age is one of the most striking biological aging phenomena in human reproduction. Live birth rates per IVF cycle fall from approximately 40% in women under 35 to 5-10% in women over 42. Spontaneous miscarriage rates rise from 15% in younger women to 50%+ in women over 42. Embryo aneuploidy rates rise from 30-40% in younger women to 70-90% in women over 42.
The majority of this decline is now attributed to oocyte mitochondrial aging. Evidence:
- Mitochondrial DNA mutations accumulate in oocytes over decades of meiotic arrest; mtDNA from oocytes of older women shows characteristic deletion patterns and heteroplasmy
- Mitochondrial membrane potential in oocytes from women over 38 is measurably reduced compared to younger women, and the reduction correlates with fertilization rates and embryo quality
- ATP content of mature oocytes correlates with subsequent embryo quality — oocytes with low ATP tend to produce slower-developing, more-fragmented embryos
- Spindle morphology in oocytes from older women shows higher rates of disorganized spindle formation, consistent with inadequate ATP supply during meiosis II
- The "mitochondrial transfer" experiments — in which cytoplasm (containing mitochondria) from younger oocytes was injected into oocytes from older women — produced clinically meaningful improvements in IVF outcomes, providing direct experimental evidence for the mitochondrial-aging hypothesis
The "ovotoxin" framework similarly identifies environmental and chemotherapy exposures that damage oocyte mitochondria as contributors to premature ovarian aging. Cigarette smoking, BPA, phthalates, and certain chemotherapeutics all show ovotoxic effects mediated in part through mitochondrial damage.
The therapeutic implication is that any intervention that improves oocyte mitochondrial function should improve reproductive outcomes — particularly in older women where mitochondrial dysfunction is the dominant cause of declining fertility. CoQ10 is the best-studied intervention with this rationale.
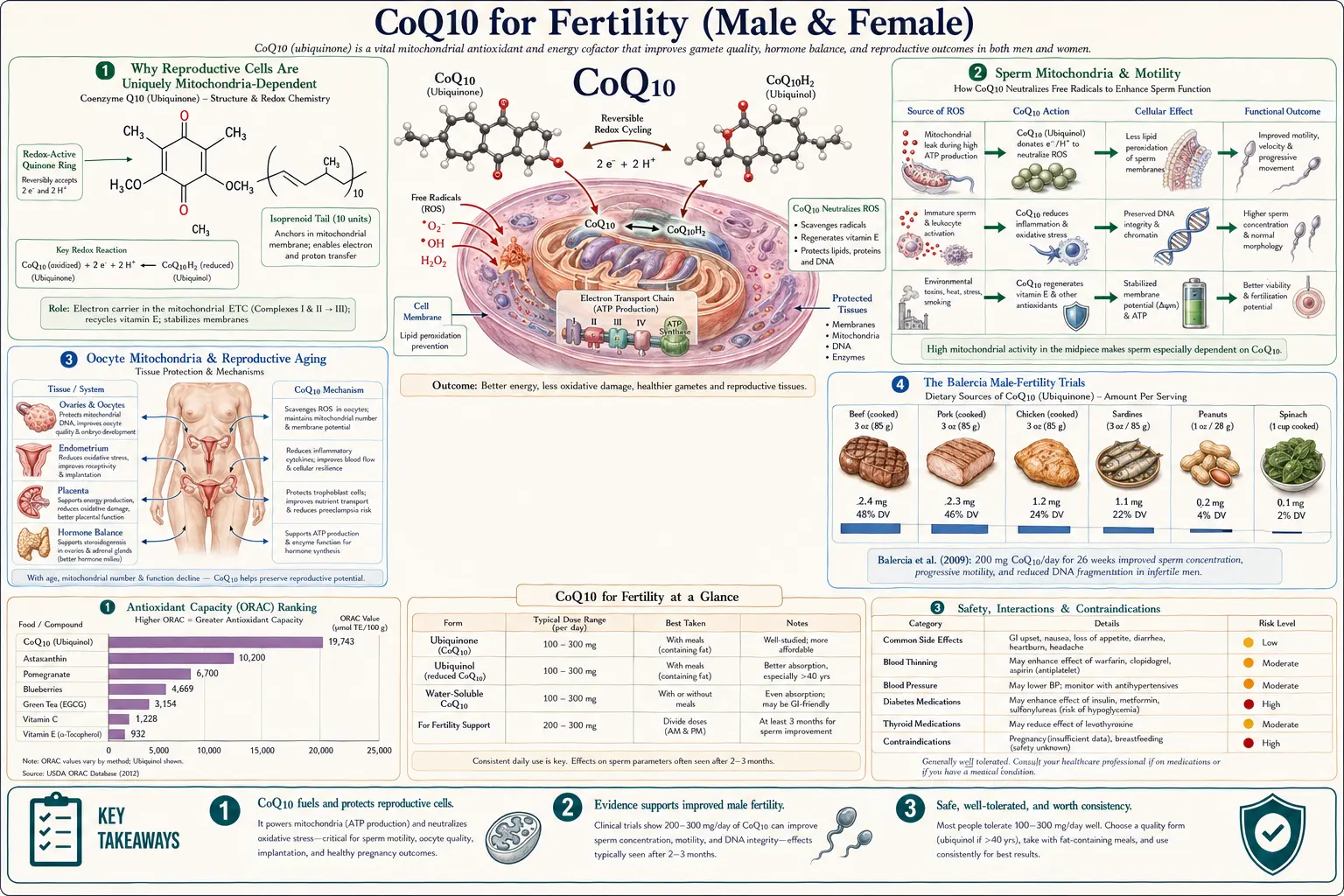
The Balercia Male-Fertility Trials
Giancarlo Balercia and colleagues at the Università Politecnica delle Marche in Ancona, Italy, published the seminal randomized trials of CoQ10 for male infertility.
Balercia 2004 (Fertility and Sterility)
- 22 men with idiopathic asthenozoospermia treated open-label with CoQ10 200 mg/day for 6 months
- Semen analyses at baseline, 3 months, and 6 months
- Results: Total motility increased from 27% to 35%; progressive motility increased from 17% to 24%; both improvements significant (p < 0.05)
- Seminal CoQ10 concentration rose proportionally with motility improvement, supporting a direct mechanism
- 3 of 22 couples achieved spontaneous pregnancy during treatment (an unusually high rate in this population)
Balercia 2009 (Fertility and Sterility)
The pivotal randomized trial:
- 60 men with idiopathic asthenozoospermia randomized to CoQ10 200 mg/day or placebo for 6 months, followed by 3 months washout
- Primary outcomes: sperm density, total motility, progressive motility, morphology
- Pregnancy outcomes monitored over 12 months
Results:
- Sperm density increased significantly in CoQ10 group (mean +6.2 × 10&sup6;/mL) vs no change in placebo
- Total motility increased by 5.4 percentage points in CoQ10 group vs 1.1 in placebo (p < 0.05)
- Progressive motility increased by 4.6 percentage points vs 0.8 (p < 0.05)
- Seminal CoQ10 and ubiquinol concentrations rose 2-3× in active group
- Spontaneous pregnancy rate: 21% (CoQ10) vs 6% (placebo) over 12-month follow-up
- Benefits regressed during the 3-month washout, supporting causal attribution
Balercia's results have been replicated in subsequent trials by Safarinejad, Nadjarzadeh, and others, all using similar protocols (200-300 mg/day CoQ10 for 3-6 months). The cumulative evidence base places CoQ10 among the best-supported nutraceutical interventions for male factor infertility.
Lafuente 2013 Male-Fertility Meta-Analysis
Rocio Lafuente and colleagues published a meta-analysis in 2013 (Journal of Assisted Reproduction and Genetics) pooling 3 randomized trials with 149 patients on CoQ10 200-300 mg/day for 3-6 months. Outcomes:
- Total sperm motility: significant improvement (mean increase +4.5%, 95% CI 1.4-7.7)
- Progressive motility: significant improvement (mean +3.7%, 95% CI 1.8-5.6)
- Sperm concentration: improvement borderline-significant
- Pregnancy rates: too few events for meta-analytic estimate but trend toward improvement
The Lafuente meta-analysis concluded that CoQ10 supplementation produces clinically meaningful improvements in motility and concentration in men with idiopathic infertility, supporting routine clinical use.
The 2019 Cochrane review on antioxidants for male subfertility (which included CoQ10 among other interventions) found that antioxidant therapy modestly increased live birth rates and clinical pregnancy rates in subfertile men, with moderate-quality evidence. CoQ10 was identified as one of the best-individually-supported antioxidants in the analysis.
The Bentov & Casper IVF Trials
Yaakov Bentov and Robert Casper at Mount Sinai Hospital / Toronto Centre for Advanced Reproductive Technology (TCART) led the pivotal female-fertility CoQ10 work.
Bentov & Casper 2013 (Fertility and Sterility review)
The conceptual framework paper laying out the mitochondrial-aging hypothesis of female reproductive decline and the therapeutic rationale for CoQ10 supplementation in older women undergoing IVF. The paper cited:
- Animal evidence that CoQ10 administration restored ovarian responsiveness and oocyte quality in aged mice
- Theoretical pharmacokinetic calculations showing that 60-90 days of ubiquinol supplementation would saturate oocyte mitochondria during the relevant antral-to-pre-ovulatory follicle development window
- Initial clinical observations of improved IVF outcomes with CoQ10 pretreatment
Bentov 2014 (Antioxidants & Redox Signaling)
Randomized controlled trial:
- 39 women ages 35-43 undergoing IVF, randomized to ubiquinol 200 mg three times daily (600 mg/day total) for 60 days before cycle start, or no supplement (open-label control)
- Primary outcomes: ovarian response (number of mature oocytes retrieved), high-quality blastocyst rate, fertilization rate, aneuploidy rate by preimplantation genetic testing
Results:
- Ovarian response: 6.7 mature oocytes (CoQ10) vs 4.1 (control), p = 0.03
- High-quality blastocyst rate: significantly higher in CoQ10 group
- Fertilization rate: significantly higher in CoQ10 group
- Aneuploidy rate: 46% (CoQ10) vs 63% (control), trending toward significance
- No serious adverse events
The Bentov 2014 trial was small but provided proof of concept that ubiquinol pretreatment could improve IVF outcomes in women of advanced reproductive age. Several subsequent trials have replicated the finding with various dose and duration protocols.
The Bentov / Casper laboratory continued research demonstrating that CoQ10 supplementation in aged mice restored ovarian responsiveness, increased mitochondrial membrane potential in oocytes, and reduced aneuploidy — providing strong mechanistic support for the clinical findings.
Xu 2018 — Poor Ovarian Responders
Yan Xu and colleagues published a randomized controlled trial in 2018 (Reproductive Biology and Endocrinology) of CoQ10 in women classified as "poor ovarian responders" by Bologna Criteria — women who failed to develop adequate follicles in previous IVF cycles despite high gonadotropin doses, typically older or with diminished ovarian reserve.
Design
- 169 women with previous poor IVF response randomized to CoQ10 600 mg/day for 60 days before next IVF cycle, or no supplement
- Primary outcomes: number of oocytes retrieved, fertilization rate, embryo quality, clinical pregnancy rate
Results
- Number of oocytes retrieved: 4.0 (CoQ10) vs 2.1 (control), p < 0.001
- Fertilization rate: 67.5% vs 45.1%, p < 0.001
- High-quality embryo rate: significantly higher in CoQ10 group
- Clinical pregnancy rate: 32.5% vs 13.7%, p = 0.008
- Cancellation rate (failure to retrieve any oocytes): 8.3% vs 23.5%, p = 0.008
The Xu trial produced larger effect sizes than Bentov 2014, likely because the poor-responder population had more room for improvement. The 2× increase in clinical pregnancy rate is striking and has motivated wider adoption of CoQ10 pretreatment in poor-responder IVF protocols.
Male Fertility Protocol
Standard protocol for idiopathic asthenozoospermia
- CoQ10 form: Ubiquinol preferred for age >35; ubiquinone acceptable for younger men (cost-effective)
- Dose: 200-300 mg/day in divided doses with meals containing fat
- Duration: 3 months minimum (the duration of spermatogenesis); 6 months for optimal effect
- Reassessment: Repeat semen analysis at 3 months and again at 6 months
- Continuation: If response achieved, continue until conception or until couple completes family
Adjunctive nutrients (the "male fertility stack")
- Zinc 30-50 mg/day — essential for spermatogenesis; well-documented effect on sperm count and quality
- Selenium 100-200 µg/day — required for glutathione peroxidase activity in the testis and for selenoprotein P (involved in selenium delivery to sperm)
- L-carnitine 1-2 g/day + acetyl-L-carnitine 1-2 g/day — supports sperm membrane integrity and energy metabolism; supported by multiple meta-analyses
- Vitamin C 500-1000 mg/day — antioxidant in seminal plasma; particularly relevant for smokers (who have lower seminal vitamin C)
- Vitamin E 200-400 IU/day — lipid-soluble antioxidant that protects sperm membranes
- Folate 800-1000 mcg/day (as methylfolate) — supports DNA synthesis during spermatogenesis
- Omega-3 fatty acids 2-3 g EPA+DHA/day — supports sperm membrane fluidity
Lifestyle interventions
- Maintain testicular temperature — avoid hot tubs, prolonged sauna, tight underwear, laptops directly on lap
- Eliminate smoking and reduce alcohol
- Optimize sleep (7-9 hours nightly)
- Weight loss if BMI >30 (obesity reduces sperm quality)
- Reduce exposure to environmental endocrine disruptors (BPA, phthalates, pesticides)
Female Fertility Protocol
Trying to conceive naturally, age <35
- Ubiquinol 100-200 mg/day with breakfast (fatty meal)
- Start at least 3 months before attempting conception
- Continue through pregnancy attempts
Trying to conceive naturally, age 35-42
- Ubiquinol 200-400 mg/day in divided doses (e.g., 200 mg morning + 200 mg evening)
- Start at least 90-120 days before active conception attempts (the antral follicle development window)
- Continue indefinitely until pregnancy or discontinuation of trying
IVF pretreatment, any age
- Ubiquinol 600 mg/day (typically 200 mg three times daily with meals)
- Start 60-90 days before IVF cycle start — this covers the full antral-to-pre-ovulatory follicle development window during which mitochondrial restoration can occur
- Continue through stimulation and retrieval
- Discontinue after embryo transfer (no benefit to continued high-dose ubiquinol once pregnancy established)
Diminished ovarian reserve or recurrent IVF failure
- Ubiquinol 600 mg/day as above
- Plus DHEA 25 mg three times daily for 8-12 weeks
- Plus vitamin D supplementation to maintain 25-OH vitamin D >40 ng/mL
- Plus methylfolate, B12, omega-3, and standard prenatal vitamin
Adjunctive nutrients (the "female fertility stack")
- Methylfolate 1 mg/day — for DNA synthesis and neural tube defect prevention
- Vitamin D 2000-5000 IU/day — corrected if 25-OH below 40 ng/mL; vitamin D deficiency associates with reduced IVF success
- DHEA 25 mg three times daily — for women with diminished ovarian reserve; controversial but with some supportive RCT evidence (Casson, Wiser)
- Vitamin E 200-400 IU/day — lipid-soluble antioxidant
- Inositol (myo-inositol 2 g + D-chiro-inositol 50 mg) twice daily — supports oocyte quality, particularly in PCOS
- N-acetylcysteine 600 mg twice daily — glutathione precursor; supportive evidence in PCOS-related infertility
- Melatonin 3 mg at bedtime — antioxidant; supportive evidence for IVF outcomes in some trials
Combination Therapy (Zinc, Selenium, DHEA, Vitamin D)
Real-world fertility practice rarely uses CoQ10 in isolation. Reproductive endocrinology and integrative fertility medicine have developed combination protocols that address multiple mechanisms simultaneously.
Male combination (CoQ10 + Zinc + Selenium + L-carnitine)
The "ProXeed Plus" formulation and its generic equivalents combine:
- L-carnitine 2 g + acetyl-L-carnitine 1 g
- CoQ10 20 mg (low dose; usually augmented with additional CoQ10 supplementation)
- Vitamin C 90 mg, vitamin E 30 mg, folate 200 mcg, zinc 10 mg, selenium 50 mcg
The Lipovetsky trial and subsequent meta-analyses suggest that combination supplementation produces somewhat larger effects on sperm parameters than CoQ10 monotherapy, particularly for total motility and DNA fragmentation index.
Female combination (CoQ10 + DHEA + Vitamin D for diminished ovarian reserve)
The Wiser / Casper protocol for poor responders combines:
- Ubiquinol 600 mg/day for 60-90 days before IVF
- DHEA 25 mg three times daily for 8-12 weeks
- Vitamin D supplemented to 25-OH vitamin D >40 ng/mL
- Standard prenatal multivitamin
The combination has supported some of the largest reported improvements in IVF outcomes in poor-responder populations, though the relative contribution of each component is difficult to disentangle without factorial trials.
The PCOS subprotocol
For PCOS-related fertility issues:
- Ubiquinol 200-400 mg/day
- Myo-inositol 2 g + D-chiro-inositol 50 mg twice daily (a 40:1 ratio)
- NAC 600 mg twice daily
- Vitamin D supplementation as above
- Berberine 500 mg three times daily as metformin alternative or adjunct for insulin resistance
IVF-Specific Protocols (Pretreatment Timing)
Timing of CoQ10 supplementation relative to IVF cycle start matters because of the biology of follicle development.
Why 60-90 days before cycle start?
Ovarian follicles develop through a multi-month process. The earliest recognized stage is the primordial follicle (containing a single oocyte arrested in prophase I). Selection for ovulation begins approximately 85 days before the cycle in which the oocyte will be retrieved. During this 85-day window, the antral follicle develops, granulosa cells proliferate, and the oocyte's metabolic machinery (mitochondria, ribosomes, transcripts) is rebuilt and reorganized.
CoQ10 supplementation that begins 60-90 days before IVF cycle start covers this entire antral-to-pre-ovulatory follicle development window, giving CoQ10 time to incorporate into the developing oocyte mitochondria. Starting CoQ10 just a few weeks before cycle start (the typical convenient timing) misses most of this window and produces smaller effects.
Standard IVF pretreatment timeline
- Day −90 to −60: Start ubiquinol 200 mg three times daily (600 mg/day)
- Day −60 to −30: Continue ubiquinol; add other targeted nutrients (DHEA if poor responder, vitamin D as needed)
- Day −30 to 0 (cycle start): Continue ubiquinol through baseline ultrasound and start of stimulation
- Day 0 to retrieval: Continue ubiquinol through stimulation; discontinue all other supplements per IVF center protocol
- After retrieval through embryo transfer: Resume standard prenatal vitamin; may continue ubiquinol per personal preference
- After embryo transfer / pregnancy confirmation: Discontinue high-dose ubiquinol; transition to standard prenatal regimen
Frozen embryo transfer protocols
For frozen embryo transfer (FET) cycles, CoQ10 is less relevant because the oocyte has already been retrieved and the embryo's metabolic fate is largely determined. CoQ10 may have modest endometrial-receptivity benefits but the dramatic oocyte-quality effects do not apply to FET. Standard prenatal vitamins are sufficient.
Patient FAQ
Q: I'm 38 and trying to conceive. Should I take CoQ10?
Yes — at age 38, mitochondrial aging is already affecting oocyte quality and is a major factor in declining fertility. Ubiquinol 200-400 mg/day in divided doses with fatty meals, started 3 months before active conception attempts and continued indefinitely until pregnancy, is supported by reasonable evidence.
Q: My husband has low sperm motility. Will CoQ10 help?
Yes, if the cause is idiopathic asthenozoospermia (no obvious anatomical, hormonal, or infectious cause). The Balercia trials and Lafuente meta-analysis support 200-300 mg/day of ubiquinol or ubiquinone for 3-6 months. Add zinc, selenium, L-carnitine, and antioxidants for the full "male fertility stack."
Q: How long before IVF should I start CoQ10?
At least 60 days, ideally 90 days. This timing covers the full antral follicle development window during which mitochondrial restoration can occur. Starting just a few weeks before retrieval misses most of the relevant window.
Q: Ubiquinol or ubiquinone for fertility?
Ubiquinol for women over 35 and for men over 40 because of impaired conversion in older patients. Ubiquinone is acceptable for younger patients and is substantially cheaper. The Bentov and Xu trials specifically used ubiquinol; the Balercia trials used ubiquinone with positive results.
Q: Is 600 mg/day safe?
Yes — the Xu and Bentov IVF trials used 600 mg/day for 60-90 days without significant adverse events. CoQ10 has one of the cleanest safety profiles of any supplement, with no documented serious adverse events at doses up to 3000 mg/day in primary CoQ10 deficiency.
Q: Can I take CoQ10 during pregnancy?
Standard prenatal vitamins are generally sufficient once pregnancy is established. High-dose ubiquinol can be continued but the dramatic mitochondrial-restoration benefit applies primarily to the pre-conception oocyte and is largely irrelevant to the developing embryo and fetus. CoQ10 is occasionally used during pregnancy for pre-eclampsia prevention (small trials suggest benefit), but discuss with your obstetrician.
Q: What if I'm doing donor egg IVF?
The oocyte mitochondrial-aging mechanism doesn't apply — the donor's oocytes are young. CoQ10 has minimal expected benefit in donor egg cycles. Standard prenatal supplementation is sufficient.
Q: What about PCOS-related infertility?
CoQ10 has supportive evidence in PCOS, particularly when combined with myo-inositol, NAC, and vitamin D. The combined protocol addresses both ovulation induction (through inositol's insulin-sensitizing effect) and oocyte quality (through CoQ10's mitochondrial support).
Cautions
- Discuss with reproductive endocrinologist or fertility specialist before starting — high-dose ubiquinol fits into broader pre-conception or IVF protocols that should be coordinated
- Discontinue high-dose ubiquinol after embryo transfer — transition to standard prenatal vitamin once pregnancy is established; the dramatic mitochondrial-restoration benefit is for the pre-fertilization oocyte
- Take with fatty meals — CoQ10 absorption increases 3-4× with dietary fat >10 grams
- Allow 60-90 days before IVF cycle — for full benefit on oocyte mitochondrial function
- DHEA cautions for women — DHEA supplementation can cause acne, mild hirsutism, hair thinning, and mood changes. Discontinue if these emerge. Not appropriate for women with hormone-sensitive cancers.
- Continue rather than restart prenatal vitamin — prenatal vitamins should overlap with the CoQ10 protocol, not replace it
- Warfarin interaction — CoQ10 may reduce INR modestly; relevant for the rare patient on chronic anticoagulation during fertility treatment
- Address modifiable factors — smoking, alcohol, weight, and stress all affect fertility independently of CoQ10. Supplementation is most effective when combined with comprehensive lifestyle optimization.
Key Research Papers
- Balercia G et al. (2004). Coenzyme Q10 supplementation in infertile men with idiopathic asthenozoospermia: an open, uncontrolled pilot study. Fertility and Sterility 81(1):93-98. — PubMed
- Balercia G et al. (2009). Coenzyme Q10 treatment in infertile men with idiopathic asthenozoospermia: a placebo-controlled, double-blind randomized trial. Fertility and Sterility 91(5):1785-1792. — PubMed
- Lafuente R et al. (2013). Coenzyme Q10 and male infertility: a meta-analysis. Journal of Assisted Reproduction and Genetics 30(9):1147-1156. — PubMed
- Safarinejad MR et al. (2009). Efficacy of coenzyme Q10 on semen parameters, sperm function and reproductive hormones in infertile men. Journal of Urology 182(1):237-248. — PubMed
- Bentov Y & Casper RF (2013). The aging oocyte: can mitochondrial function be improved? Fertility and Sterility 99(1):18-22. — PubMed
- Bentov Y et al. (2014). Coenzyme Q10 supplementation and oocyte aneuploidy in women undergoing IVF-ICSI treatment. Antioxidants & Redox Signaling. — PubMed
- Xu Y et al. (2018). Pretreatment with coenzyme Q10 improves ovarian response and embryo quality in low-prognosis young women with decreased ovarian reserve: a randomized controlled trial. Reproductive Biology and Endocrinology 16(1):29. — PubMed
- Ben-Meir A et al. (2015). Coenzyme Q10 restores oocyte mitochondrial function and fertility during reproductive aging. Aging Cell 14(5):887-895. — PubMed
- Nadjarzadeh A et al. (2014). Coenzyme Q10 improves seminal oxidative defense but does not affect on semen parameters in idiopathic oligoasthenoteratozoospermia: a randomized double-blind placebo-controlled trial. Andrology 2(5):797-803. — PubMed
- Smits RM et al. (2019). Antioxidants for male subfertility. Cochrane Database of Systematic Reviews 3:CD007411. — PubMed
- Showell MG et al. (2017). Antioxidants for female subfertility. Cochrane Database of Systematic Reviews 7:CD007807. — PubMed
- Wang Y et al. (2010). The reproductive effects of beta-cypermethrin on zebrafish: an example of oocyte oxidative damage. Aquatic Toxicology. — PubMed: oocyte mitochondrial ATP meiotic spindle
PubMed Topic Searches
- PubMed: CoQ10 male fertility sperm motility
- PubMed: CoQ10 IVF oocyte quality
- PubMed: ubiquinol IVF pretreatment
- PubMed: oocyte mitochondria aneuploidy
- PubMed: poor ovarian responder CoQ10 DHEA
- PubMed: male fertility antioxidant stack
Connections
- Free Radicals & Your Antioxidant Network — interactive animation
- CoQ10 Overview
- CoQ10 Benefits Hub
- CoQ10 for Heart Failure
- CoQ10 for Statin Myopathy
- CoQ10 for Migraine
- Reproductive Medicine
- Zinc
- Selenium
- Magnesium
- Vitamin D
- Vitamin E
- Folate (B9)
- L-Carnitine
- NAC
- Alpha Lipoic Acid
- All Antioxidants
- Omega-3 Fatty Acids
- Oxidative Stress
- Longevity Protocols