Vitamin D Toxicity (Hypervitaminosis D): Thirst and Frequent Urination
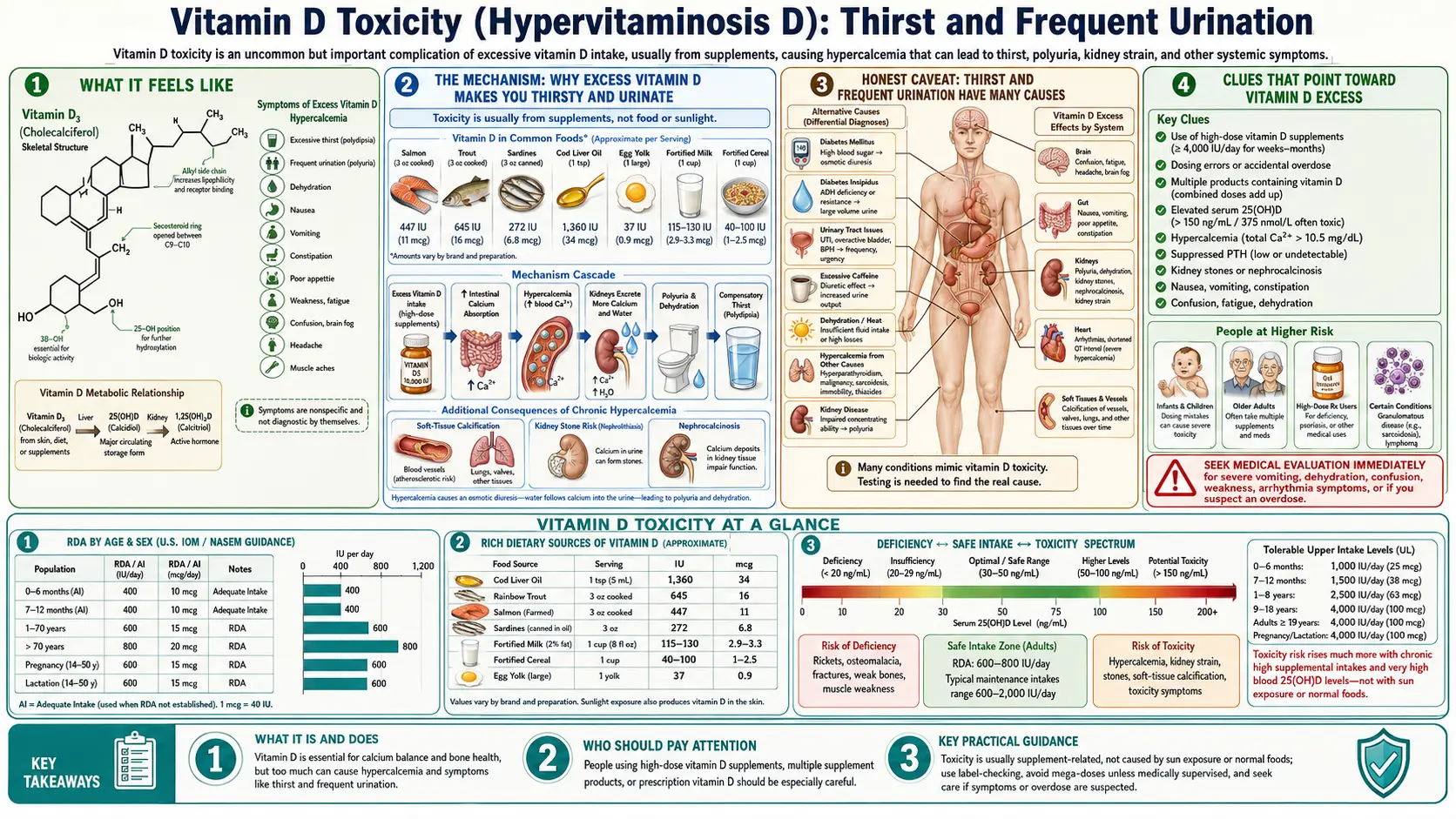
When too much vitamin D builds up in the body — almost always from over-the-counter or prescribed supplements taken in very large doses — one of the earliest and most reliable warning signs is a sudden, relentless thirst paired with passing large volumes of urine, including waking repeatedly at night to do so. You drink, yet you stay thirsty; you urinate, yet the bottle of water never seems to last. It feels like the thirst of poorly controlled diabetes, and that resemblance is no accident — but here the cause is not sugar. It is too much calcium in the blood, driven up by excess vitamin D, interfering with how the kidneys concentrate urine. This page explains exactly how that happens, why thirst and frequent urination are common to many conditions (so they are a clue, not a diagnosis), when they should make you suspect vitamin D excess specifically, and the red flags that mean you should be checked without delay.
Table of Contents
- What It Feels Like
- The Mechanism: Why Excess Vitamin D Makes You Thirsty and Urinate
- Honest Caveat: Thirst and Frequent Urination Have Many Causes
- Clues That Point Toward Vitamin D Excess
- What Causes Vitamin D to Build Up This High
- Getting Checked
- How It Is Treated
- When to Seek Care / Red Flags
- Key Research Papers
- Connections
- Featured Videos
What It Feels Like
The medical names are tidy: polydipsia for excessive thirst and polyuria for passing abnormally large amounts of urine. What they describe is anything but tidy to live with. People who develop this from vitamin D excess tend to notice a cluster of changes that build over days to a few weeks:
- Thirst that water doesn’t fix. You drink a full glass, and within minutes your mouth feels dry again. The thirst is driving and persistent rather than the ordinary thirst of a hot afternoon.
- Large-volume urine, not just frequent trips. The key feature is volume — copious, pale, watery urine each time — rather than the small, urgent, sometimes stinging passes of a bladder infection. Some people produce several liters a day.
- Waking at night to urinate (nocturia). Needing to get up two, three, or more times a night is one of the most disruptive and noticeable parts, and often the first thing people mention.
- A dry mouth and dehydration despite drinking. Because the kidneys are pouring out water faster than drinking can keep up, the mouth and lips stay dry, the skin loses its spring, and lightheadedness on standing can appear.
Crucially, with vitamin D toxicity these symptoms rarely arrive alone. They usually travel with the wider picture of high blood calcium (hypercalcemia) — nausea, poor appetite, constipation, fatigue, muscle weakness, and in worse cases confusion. Clinicians summarize the classic hypercalcemia syndrome with a rhyme: “stones, bones, abdominal groans, and psychiatric moans” — kidney stones, bone pain, abdominal upset, and mood or thinking changes. Thirst and frequent urination are part of that same story, and the companion pages on hypercalcemia and nausea and confusion cover the rest of it.
The Mechanism: Why Excess Vitamin D Makes You Thirsty and Urinate
To see why too much vitamin D ends in raging thirst, it helps to follow the chain one link at a time. Vitamin D’s main job is to raise calcium: it increases calcium absorbed from food in the gut, and in excess it also pulls calcium out of bone. When vitamin D is present in enormous amounts, this calcium-raising machinery runs without a brake, and blood calcium climbs — the condition called hypercalcemia. Almost every symptom of vitamin D toxicity, including thirst and frequent urination, flows from that high calcium rather than from the vitamin itself.
The kidney is where high calcium turns into thirst. Normally, when your body needs to conserve water, the brain releases a hormone called antidiuretic hormone (ADH, also called vasopressin). ADH tells the kidney’s collecting ducts to insert tiny water channels (called aquaporin-2) into their walls, so water is reabsorbed back into the body and urine becomes concentrated. High blood calcium jams this system in two ways:
- It makes the kidney deaf to ADH. Excess calcium activates a sensor in the collecting duct — the calcium-sensing receptor — which down-regulates those aquaporin-2 water channels. Even when ADH is shouting “hold onto water,” the kidney can no longer respond. This is a textbook example of nephrogenic diabetes insipidus: the hormone is present, but the kidney is resistant to it. The result is dilute urine pouring out and the body steadily losing water.
- It impairs the kidney’s concentrating gradient. High calcium also interferes with the salt-pumping machinery in the loop of Henle that builds the deep osmotic gradient the kidney relies on to draw water back. Without that gradient, the kidney cannot concentrate urine even when it “wants” to.
Now the thirst makes sense. As the kidneys dump water, the blood becomes more concentrated and the body is heading toward dehydration. The brain’s thirst center detects this and demands water — hence the unquenchable drinking. The polyuria comes first; the polydipsia is the body chasing it. And there is a vicious cycle: dehydration concentrates the blood calcium even further, which worsens the kidney resistance, which drives still more urination. Left unchecked, this spiral can tip into dangerous dehydration and acute kidney injury.
An analogy. Think of ADH as a manager phoning the kidney’s “water-recovery department” with the order, “close the drains, save the water.” High calcium is like static on the line that drowns out the call — the order is being given, but the department never hears it, so the drains stay wide open. You keep pouring water into the top of the system (drinking), and it keeps running straight out the bottom (urinating). The fix is not to shout louder down the phone; it is to clear the static — bring the calcium, and the vitamin D driving it, back down.
Honest Caveat: Thirst and Frequent Urination Have Many Causes
This is the most important section to read with a level head. Excessive thirst and frequent urination are among the most common and non-specific symptoms in all of medicine, and vitamin D toxicity is a genuinely uncommon cause of them. If you have these symptoms, the odds heavily favor something other than too much vitamin D. Before assuming a supplement is to blame, an honest list of the usual suspects includes:
- Diabetes mellitus (high blood sugar) — by far the most common cause. When blood glucose is high, sugar spills into the urine and drags water with it, producing exactly this thirst-and-urination pattern. New or poorly controlled diabetes must be ruled out first, with a simple glucose or HbA1c test.
- Simply drinking a lot of fluid. High intake of water, coffee, tea, or alcohol — or a strong habit of carrying a water bottle — produces large urine volumes for an entirely benign reason. Caffeine and alcohol are mild diuretics on top of the fluid they deliver.
- Diuretic medications. “Water pills” prescribed for blood pressure or heart failure increase urination by design.
- Diabetes insipidus (unrelated to blood sugar). A problem with ADH itself — either the brain not making enough (central) or the kidney not responding (nephrogenic) — causes large-volume dilute urine. See diabetes insipidus. (Note: vitamin D excess causes a nephrogenic form of this, via calcium — so the categories overlap.)
- Urinary tract infection or an overactive bladder. These usually cause frequent, urgent, small passes rather than large volumes, and often burning — a different pattern, but a common reason people feel they are “urinating all the time.”
- Other causes of high calcium. Even when thirst is from hypercalcemia, vitamin D is not the only thing that raises calcium. An overactive parathyroid gland (primary hyperparathyroidism) and high calcium from cancer are more common causes of hypercalcemia overall.
- Anxiety and dry mouth from medications. Many drugs cause a dry mouth that feels like thirst without true water loss.
So treat thirst and frequent urination as a signal to get checked, not as a verdict. The symptom does not announce its own cause. The value of the next section is in recognizing the particular circumstances that should move “too much vitamin D” up the list of possibilities — but the diagnosis is always made by a blood test, never by the symptom alone.
Clues That Point Toward Vitamin D Excess
Given how non-specific the symptom is, what tilts suspicion toward vitamin D? A few practical clues, especially in combination:
- You take high-dose vitamin D. This is the single biggest clue. Regularly taking very high amounts — for example tens of thousands of international units (IU) per day for weeks or months, or massive one-off “mega-doses” — is the usual setup. The Endocrine Society and most authorities treat sustained intakes well above the tolerable upper limit (commonly cited around 4,000 IU/day for adults) as the territory where risk begins to climb, though true toxicity generally requires much higher, prolonged dosing.
- A new bottle, a compounded product, or a labeling error. Toxicity is repeatedly traced to manufacturing or compounding mistakes where a product contained vastly more vitamin D than the label claimed, or to confusion between micrograms and IU. A symptom that began after starting a new supplement is a meaningful clue.
- The full hypercalcemia cluster is present. Thirst and urination plus nausea, constipation, poor appetite, fatigue, and muscle weakness is a more suggestive package than thirst alone. Confusion, severe weakness, or vomiting raise the concern further.
- Normal blood sugar. If a glucose or HbA1c test is normal, the most common cause — diabetes — is off the table, which makes a calcium-driven cause (including vitamin D) more worth pursuing.
- You also take calcium, or a “bone” or “immune” combination. Vitamin D plus generous calcium supplementation raises calcium more readily than either alone.
None of these proves vitamin D toxicity, and their absence does not rule it out. But if you have unexplained thirst and frequent urination and you take large doses of vitamin D, that combination is exactly the situation in which a clinician will check a calcium level and a vitamin D level rather than stopping at a glucose test. The other symptoms of the excess are detailed on the Vitamin D toxicity hub and its companion pages.
What Causes Vitamin D to Build Up This High
An essential reassurance first: you cannot reach toxic vitamin D levels from sunshine, and you essentially cannot reach them from food. The skin self-limits how much vitamin D it makes from sun, and natural dietary amounts are small. Vitamin D toxicity is, in practice, an over-supplementation problem. The recurring scenarios are:
- Chronic high-dose self-supplementation. Taking very large daily doses for weeks to months — often in the mistaken belief that “more is better” for immunity, bones, or mood — is the most common route. Vitamin D is fat-soluble and stored in body fat and the liver, so it accumulates over time rather than being flushed out daily.
- Prescribing or dosing errors and megadoses. Intermittent “bolus” or megadose regimens, and outright errors (a weekly dose taken daily, a decimal-point slip), can deliver toxic totals.
- Mislabeled or contaminated products. Documented outbreaks of toxicity have come from over-the-counter or compounded supplements that contained many times the stated dose. This is a well-described and recurring cause.
- Granulomatous diseases and lymphomas. In conditions such as sarcoidosis and tuberculosis, abnormal immune cells convert vitamin D into its active form without the body’s usual brakes. In these people, even modest, ordinarily safe vitamin D doses can push calcium too high.
How long it lingers matters for recovery: because vitamin D is fat-soluble and its breakdown products have long half-lives, hypercalcemia and the thirst it drives can persist for weeks after the supplement is stopped. Recovery is not instant, which is one reason the condition deserves medical follow-up rather than simply stopping the pills and waiting.
Getting Checked
Confirming the cause is straightforward and rests on a few blood tests, interpreted together. Because thirst and frequent urination have so many causes, the workup deliberately looks beyond vitamin D.
- Blood calcium. The pivotal test. A Comprehensive Metabolic Panel reports calcium along with kidney function. Because much of the blood’s calcium is carried on albumin, the result is corrected for albumin (or an ionized calcium is measured directly) so a true high calcium is not missed or overcalled.
- Vitamin D level. The 25-hydroxyvitamin D test measures the body’s vitamin D stores. In toxicity it is strikingly high — typically well above 100–150 ng/mL — which, paired with high calcium, makes the diagnosis.
- Parathyroid hormone (PTH). This distinguishes vitamin D toxicity from the most common cause of high calcium. In vitamin-D-driven hypercalcemia, PTH is appropriately suppressed (low), because the body is trying to lower calcium. A high PTH instead points to primary hyperparathyroidism, an entirely different diagnosis.
- Blood glucose / HbA1c. To rule out diabetes — the most common cause of the symptom — before attributing it to calcium or vitamin D.
- Kidney function. Creatinine and a kidney function assessment gauge whether the high calcium and dehydration have already strained the kidneys, which guides how urgently to treat.
The diagnostic pattern that nails vitamin D toxicity is the trio: high calcium + very high 25-hydroxyvitamin D + suppressed PTH, in someone taking large vitamin D doses. A clinician will also review the supplement bottles themselves — the actual product is often the key piece of evidence.
How It Is Treated
Treatment targets the high calcium (which is what makes a person ill) and removes its source. The thirst and frequent urination ease as calcium falls and the kidneys regain their ability to concentrate urine. Depending on severity, the steps are:
- Stop all vitamin D — and calcium — immediately. The first and non-negotiable step. Stopping the supplement removes the engine driving calcium up. Because stored vitamin D lingers, this alone is not a fast fix, but it is essential.
- Rehydrate. Mild cases improve with generous fluids; significant hypercalcemia is treated in hospital with intravenous saline, which both corrects the dehydration the polyuria caused and helps the kidneys excrete calcium. This is usually the single most effective early measure.
- Medications to lower calcium. When calcium is high or symptoms are marked, doctors may add corticosteroids (which reduce vitamin-D-mediated calcium absorption and are especially useful in toxicity and granulomatous disease) and bisphosphonates (which block the release of calcium from bone). Calcitonin can lower calcium quickly for a short period.
- Reduce dietary calcium and avoid extra vitamin D during recovery, and limit sunlight to a sensible degree while levels normalize.
- Treat any underlying condition. If a granulomatous disease such as sarcoidosis is the reason ordinary doses became toxic, that condition is managed in its own right.
- Monitor until resolved. Because vitamin D stores clear slowly, calcium is rechecked over the following weeks to confirm it stays down and the kidneys recover. Severe cases may need dialysis, but that is uncommon.
The encouraging news is that vitamin D toxicity, caught and treated, generally resolves fully — and it is almost entirely preventable. Staying within recommended supplement doses, buying from reputable manufacturers, and getting a 25-hydroxyvitamin D level checked before taking high doses long-term are simple safeguards. For most people, the lesson is the boring but true one: with vitamin D, more is not better, and there is no benefit to pushing the blood level far above normal.
When to Seek Care / Red Flags
Thirst and frequent urination always deserve evaluation, because the most common cause — diabetes — needs treating, and the rarer calcium-driven causes can be serious. Get checked promptly if these symptoms are new and persistent. Seek urgent or emergency care if you have, or develop, any of the following — particularly if you take high-dose vitamin D:
- Confusion, drowsiness, or difficulty staying awake — a sign that calcium may be dangerously high and affecting the brain (see nausea and confusion).
- Persistent vomiting or an inability to keep fluids down, which accelerates dehydration on top of the urinary water loss.
- Signs of significant dehydration — severe dizziness or fainting on standing, very dry mouth, little or no urine despite the earlier flood, or a racing heartbeat.
- Severe weakness, intense abdominal pain, or a markedly reduced urine output — which can signal kidney injury from the high calcium and dehydration.
- Flank or back pain with blood in the urine — possible kidney stones, which high calcium promotes.
If you take large doses of vitamin D and have unexplained thirst and frequent urination, tell the clinician about the supplement explicitly and bring the bottle. A single blood draw — calcium, vitamin D, PTH, and glucose — can sort out the cause quickly, and catching high calcium early prevents the slide into dehydration and kidney damage. When in doubt, be seen; the test is simple and the stakes, when calcium is the culprit, are real.
Key Research Papers
- Holick MF (2007). Vitamin D Deficiency. New England Journal of Medicine;357(3):266-281. — DOI: 10.1056/NEJMra070553
- Holick MF, Binkley NC, Bischoff-Ferrari HA, et al. (2011). Evaluation, Treatment, and Prevention of Vitamin D Deficiency: an Endocrine Society Clinical Practice Guideline. The Journal of Clinical Endocrinology & Metabolism;96(7):1911-1930. — DOI: 10.1210/jc.2011-0385
- Kennel KA, Drake MT, Hurley DL (2010). Vitamin D Deficiency in Adults: When to Test and How to Treat. Mayo Clinic Proceedings;85(8):752-758. — DOI: 10.4065/mcp.2010.0567
- Marcinowska-Suchowierska E, et al. Vitamin D Toxicity — A Clinical Perspective. Frontiers in Endocrinology (review). — PubMed search
- Galior K, Grebe S, Singh R (2018). Development of Vitamin D Toxicity from Overcorrection of Vitamin D Deficiency: A Review of Case Reports. Nutrients;10(8):953. — DOI: 10.3390/nu10080953
- Dudenkov DV, Yawn BP, Oberhelman SS, et al. (2015). Changing Incidence of Serum 25-Hydroxyvitamin D Values Above 50 ng/mL: A 10-Year Population-Based Study. Mayo Clinic Proceedings;90(5):577-586. — DOI: 10.1016/j.mayocp.2015.03.015
- Stewart AF (2005). Hypercalcemia Associated with Cancer. New England Journal of Medicine;352(4):373-379. — DOI: 10.1056/NEJMcp042806
- Bouillon R, Marcocci C, Carmeliet G, et al. (2019). Skeletal and Extraskeletal Actions of Vitamin D: Current Evidence and Outstanding Questions. Endocrine Reviews;40(4):1109-1151. — DOI: 10.1210/er.2018-00126
- Bischoff-Ferrari HA (2017). The vitamin D deficiency pandemic: Approaches for diagnosis, treatment and prevention. Reviews in Endocrine and Metabolic Disorders;18(2):153-165. — DOI: 10.1007/s11154-017-9424-1
- Hypercalcemia-induced nephrogenic diabetes insipidus — mechanisms of impaired urinary concentration (down-regulation of aquaporin-2 via the calcium-sensing receptor). Review literature. — PubMed search
PubMed Topic Searches
- PubMed — Vitamin D toxicity and hypercalcemia
- PubMed — Hypercalcemia, polyuria, and nephrogenic diabetes insipidus
- PubMed — Calcium-sensing receptor and aquaporin-2 in the collecting duct
- PubMed — Vitamin D supplement overdose case reports
- NIH Office of Dietary Supplements — Vitamin D Fact Sheet (Health Professional)
Connections
- Vitamin D Toxicity Hub
- Vitamin D Toxicity and Hypercalcemia
- Vitamin D Toxicity and Kidney Stones & Damage
- Vitamin D Toxicity and Nausea & Confusion
- Vitamin D3 Overview
- Vitamin D3 Food Sources
- Vitamin D3 and Bone Health
- Calcium
- Magnesium
- Diabetes
- Diabetes Insipidus
- Kidney Disease
- Vitamin D Test (25-Hydroxyvitamin D)
- Comprehensive Metabolic Panel
- Kidney Function