Vitamin D Toxicity (Hypervitaminosis D): Nausea and Confusion
When vitamin D climbs to genuinely toxic levels — almost always from too many high-dose supplements, never from sunshine and only very rarely from food — two of the earliest and most telling symptoms are stomach upset (nausea, vomiting, poor appetite, constipation) and a fuzzy, confused head. Here is the key to understanding both: vitamin D itself does not poison the gut or the brain directly. Instead, an overdose drives blood calcium too high — a state called hypercalcemia — and it is the excess calcium that turns the stomach and clouds the mind. That single fact explains the symptoms, links this page to its siblings, and points to why a blood test, not guesswork, is what settles the question. This page is about the nausea and confusion specifically: how they feel, why high calcium causes them, the many far more common reasons a person feels sick and foggy, and when these symptoms mean you should be checked promptly.
Table of Contents
- What the Nausea and Confusion Feel Like
- The Mechanism: How Vitamin D Excess Reaches the Gut and Brain
- Honesty: These Symptoms Have Many Causes
- Clues That Point Toward Vitamin D Toxicity
- How People End Up With Too Much Vitamin D
- Getting Checked
- How Vitamin D Toxicity Is Treated
- When to Seek Care / Red Flags
- Key Research Papers
- Connections
- Featured Videos
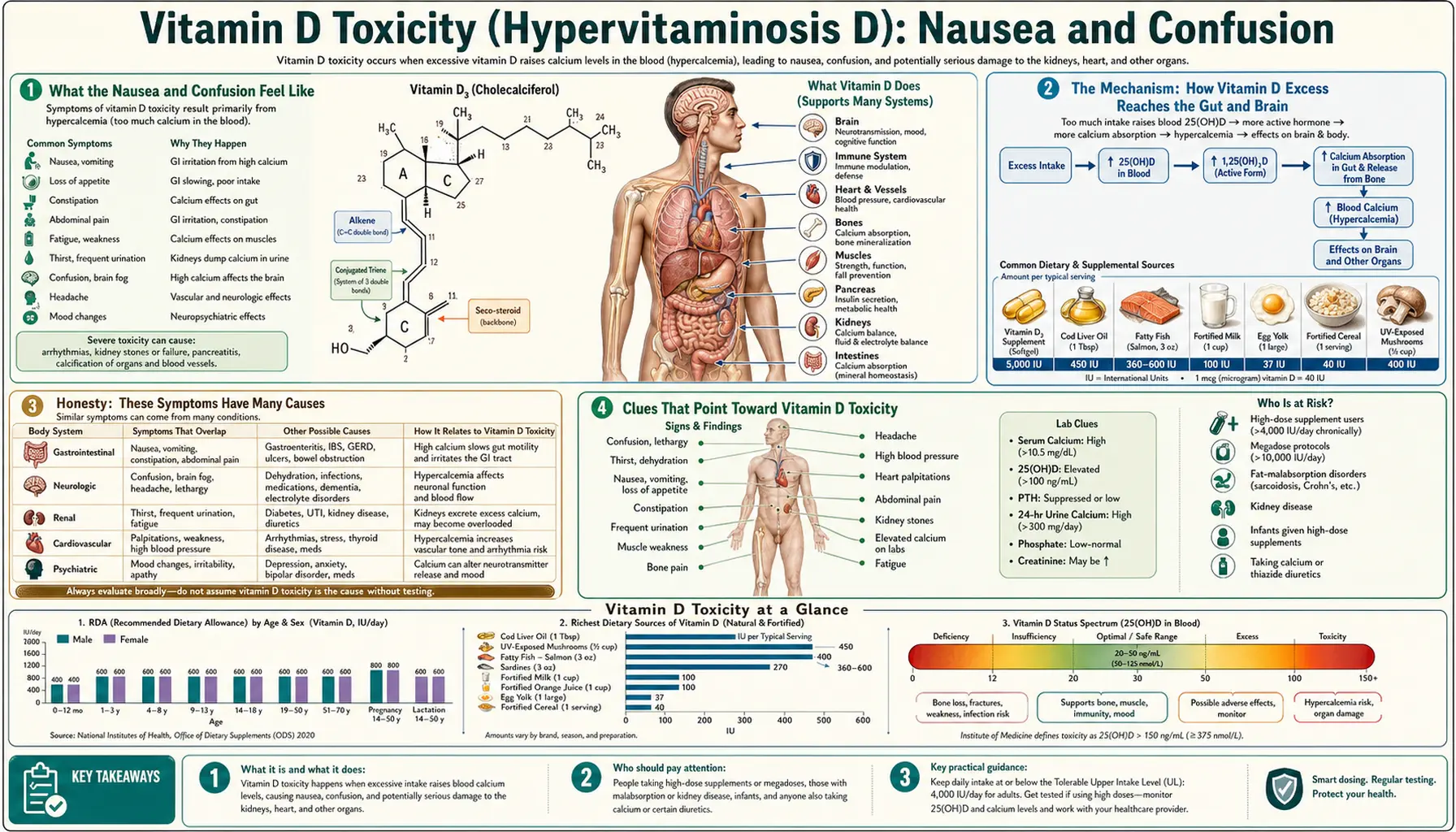
What the Nausea and Confusion Feel Like
Vitamin D toxicity tends to announce itself first in the digestive system, and the picture is usually a cluster rather than a single complaint. People describe:
- Nausea and vomiting. A queasy, off-food feeling that can build into repeated vomiting. It often comes without the fever or diarrhea you would expect from a stomach bug.
- Loss of appetite. Food simply stops appealing, and meals get skipped — an early, easily dismissed sign.
- Constipation. Counter-intuitively, high calcium slows the gut, so constipation — not diarrhea — is the typical bowel change, sometimes with vague stomach-ache or bloating.
- Excessive thirst and a dry mouth. Often the stomach upset travels alongside relentless thirst and frequent urination, because high calcium also disturbs how the kidneys handle water (covered on the companion page, Thirst & Frequent Urination).
The mental changes usually come a little later, or alongside more severe cases, and they are easy to mistake for ordinary tiredness at first:
- Mental fog and trouble concentrating. Thoughts feel slow and effortful; people lose the thread of conversations or struggle with simple tasks they normally breeze through.
- Confusion and disorientation. In more pronounced cases there is genuine confusion — muddled about time or place, repeating questions, not quite making sense.
- Drowsiness and apathy. An unusual sleepiness, low mood, or flat, “can’t be bothered” feeling. Clinicians sometimes capture this and the queasiness together in the old teaching mnemonic for hypercalcemia: “stones, bones, abdominal groans, and psychiatric moans.”
- At the extreme, severe confusion or stupor. When calcium climbs very high, the confusion can deepen toward profound drowsiness or unresponsiveness — a medical emergency, dealt with in the red-flags section below.
What ties the queasiness and the mental fog together is that both are downstream of the same problem — a rising blood calcium — rather than two unrelated things going wrong. That is also why they so often appear in the same person at the same time, which the next section explains.
The Mechanism: How Vitamin D Excess Reaches the Gut and Brain
To make sense of these symptoms it helps to remember what vitamin D normally does. Its central job is to raise blood calcium: it switches on genes in the intestine that build calcium-absorbing machinery, so more calcium is pulled from food into the blood, and it helps mobilize calcium from bone. In normal amounts this is tightly regulated and entirely beneficial. The trouble in toxicity is that the regulation is overwhelmed.
When someone takes far too much vitamin D for long enough, the body becomes loaded with the storage form, 25-hydroxyvitamin D (the same form a blood test measures). At very high concentrations this flood of vitamin D metabolites drives calcium absorption far beyond what the body needs, and bone releases calcium too. The result is hypercalcemia — too much calcium circulating in the blood. The full account of how that happens lives on the companion page Hypercalcemia; here the point is simply that calcium is the messenger that carries the harm to the gut and the brain.
Why high calcium upsets the stomach. Calcium is not a passive bystander in the digestive tract — it helps set the pace of the smooth muscle that moves food along and tunes the nerves of the gut. When blood calcium rises too high, that machinery is thrown off: stomach emptying slows, the gut’s muscular waves (peristalsis) become sluggish, and stomach-acid–driving hormones such as gastrin can be stimulated. The felt result is exactly the cluster above — nausea, vomiting, a appetite that vanishes, and a constipated, slowed-down bowel. High calcium can also, less often, inflame the pancreas (pancreatitis), which causes more severe abdominal pain.
Why high calcium clouds the mind. Calcium is one of the ions that govern how readily nerve cells fire. Inside a narrow range, the right calcium level keeps neurons appropriately excitable. Push calcium too high and it has a dampening effect on nerve and brain-cell signaling — messages travel less crisply, networks that normally hum along get muffled. Felt from the inside, that muffling is the mental fog, the slowed thinking, the drowsiness, and, when calcium is very high, frank confusion. Severe hypercalcemia can also cause a degree of dehydration (the kidneys spill water trying to clear the calcium load), and dehydration worsens confusion on its own — so the two mechanisms compound each other.
An analogy. Think of calcium as the dimmer switch on the body’s electrical and muscular systems. At the correct setting the lights are bright and steady and the motors run smoothly. Turn the dimmer up too far — too much calcium — and instead of getting brighter, the circuits start to brown out: the gut’s motors stall (nausea, constipation) and the brain’s lights flicker and dim (fog, confusion, drowsiness). Bring the dimmer back to its proper setting — lower the calcium — and both systems steady again. Crucially, you cannot fix a browned-out circuit by adding more vitamin D; that only pushes the dimmer further the wrong way.
Honesty: These Symptoms Have Many Causes
It would be a serious mistake — and this page will not make it — to treat nausea and confusion as proof of vitamin D toxicity. They are two of the most non-specific symptoms in all of medicine. Nearly everyone has felt queasy, off their food, or mentally foggy at some point, and the overwhelming majority of the time it has nothing whatever to do with vitamin D. Genuine vitamin D toxicity is, in fact, uncommon; it essentially never comes from sunlight or ordinary food and arises only from sustained, very high-dose supplementation or a dosing error.
The ordinary, far more likely explanations for nausea and confusion include:
- Infections — from a simple stomach bug or urinary infection to more serious illness; in older adults a urinary or chest infection is a classic cause of sudden confusion (delirium) with little else to show for it.
- Medications — opioids, sedatives, many chemotherapy drugs, and dozens of others routinely cause nausea, and many can cloud thinking, especially in combination.
- Dehydration and other electrolyte problems — low sodium, high or low blood sugar, and dehydration itself all produce nausea and confusion.
- Migraine, motion sickness, pregnancy, and gut disorders — common, everyday sources of nausea.
- Kidney or liver problems, thyroid disease, and many neurological conditions — all can present with a foggy, confused mind.
- Other causes of high calcium. Even when hypercalcemia is the culprit, vitamin D toxicity is not the usual reason for it. By far the most common cause of a raised calcium is an overactive parathyroid gland (primary hyperparathyroidism); cancer is the next most common, particularly in someone who is unwell in hospital. Vitamin D toxicity sits well down that list.
So the honest framing is this: if you feel sick and foggy, vitamin D toxicity is a possible but unlikely explanation unless something in your history points to it. The value of this page is helping you recognize the specific situation in which it becomes a real consideration — which is the subject of the next section — and steering you toward the simple blood test that can confirm or dismiss it.
Clues That Point Toward Vitamin D Toxicity
Vitamin D toxicity moves from “unlikely” to “worth checking now” when the nausea and confusion sit alongside the right context. The strongest clue, by a wide margin, is the supplement history:
- High-dose vitamin D over weeks or months. The classic setup is someone taking very large daily doses — commonly tens of thousands of international units (IU) a day — for an extended period, often in the mistaken belief that “more is better.” Toxicity from the modest doses in a standard multivitamin is not a realistic concern.
- A dosing or manufacturing mistake. Several documented poisonings have come from mislabeled products, compounding errors, or confusing micrograms with international units. A surprisingly common error is taking a weekly or monthly prescription dose every day.
- Megadose “immune” or “wellness” regimens. Some people self-prescribe enormous amounts after reading online claims. This is the most common real-world route to toxicity today.
Beyond the supplement bottle, certain patterns make the diagnosis more compelling:
- The full hypercalcemia cluster appearing together. Nausea and confusion plus intense thirst, frequent urination, constipation, and bone or muscle aches is a far more coherent picture than nausea alone. The companion pages cover thirst and frequent urination and the kidney effects that can accompany them.
- A gradual build-up rather than a sudden onset. Toxicity from accumulating vitamin D tends to creep in over days to weeks, unlike the abrupt arrival of a stomach virus.
- Symptoms that persist and worsen while a high-dose supplement is continued, and that have no other obvious explanation.
If those clues are present, the next step is not more internet reading or stopping and hoping — it is a blood test for calcium and vitamin D, described below. And one practical move can be made immediately: stop taking the vitamin D supplement while you arrange to be checked. Two closely related conditions that high calcium can cause — deep fatigue and confusion, and digestive upset — are also explored from the calcium side on Hypercalcemia and Fatigue & Confusion, which is well worth reading because the symptoms overlap almost completely.
How People End Up With Too Much Vitamin D
Understanding the routes to toxicity also reassures you about the routes that don’t cause it. The body has a natural brake on vitamin D made in the skin from sunlight — excess pre-vitamin D is simply broken down — so you cannot give yourself vitamin D toxicity by spending time in the sun. Food is almost never the cause either, with rare historical exceptions such as an over-fortified product. Toxicity is, in practice, a supplement phenomenon. The recognized routes are:
- Sustained megadosing. The single most common cause: taking very large daily doses for weeks to months. Case reports of toxicity typically involve intakes far above the levels any guideline recommends, maintained long enough for vitamin D and then calcium to accumulate.
- Errors with prescription or compounded products. Mislabeled bottles, pharmacy compounding mistakes that deliver a far higher dose than intended, and confusion between dosing units have all caused poisonings. So has the “daily instead of weekly” mix-up with high-strength prescription capsules.
- Stacking multiple supplements unknowingly. A standalone vitamin D pill, a multivitamin, a calcium-plus-D bone supplement, and a fortified shake can add up to far more than a person realizes — especially when a calcium supplement is taken at the same time, which adds calcium directly on top of the vitamin D–driven absorption.
- Conditions that make the body extra-sensitive to vitamin D. Certain illnesses — particularly granulomatous diseases such as sarcoidosis and some tuberculosis, and a few lymphomas — let the body convert vitamin D to its active form in an unregulated way. People with these conditions can develop hypercalcemia from amounts of vitamin D that would be perfectly safe in anyone else, which is why vitamin D is given cautiously and monitored in that setting.
The reassuring through-line: toxicity requires a large, sustained artificial dose (or an unusual underlying sensitivity). It is a problem of overzealous supplementation, not of normal living. The Vitamin D3 overview covers sensible intake ranges; the gap between a helpful dose and a harmful one is wide, which is precisely why most people never come anywhere near toxicity.
Getting Checked
Because nausea and confusion are so non-specific, the diagnosis is never made on symptoms alone — it rests on a couple of inexpensive blood tests that take the guesswork out entirely.
The first and most important is blood calcium. A Comprehensive Metabolic Panel — a routine blood draw — reports calcium directly, along with kidney function (creatinine) and other electrolytes that help explain the symptoms. If the calcium is high, that confirms hypercalcemia is present; the question then becomes why. Because albumin (a blood protein) affects the measured value, a clinician may check an ionized (free) calcium or correct the calcium for albumin to be sure the elevation is real.
The second is the vitamin D level, measured as 25-hydroxyvitamin D. In genuine vitamin D toxicity this is strikingly high — far above the range seen with sensible supplementation. A markedly elevated 25-hydroxyvitamin D together with a high calcium and a fitting supplement history makes the diagnosis straightforward.
Just as important, these tests distinguish vitamin D toxicity from its mimics. To separate it from the most common cause of high calcium — an overactive parathyroid gland — a doctor checks the parathyroid hormone (PTH) level: in vitamin D toxicity the high calcium suppresses PTH (it is appropriately low), whereas in primary hyperparathyroidism PTH is high or inappropriately normal. Depending on the picture, kidney-function tests, a phosphate level, and sometimes imaging are added to gauge any harm and rule out other causes such as cancer. The reassuring bottom line: a few millilitres of blood usually settle whether vitamin D is the culprit or an innocent bystander.
How Vitamin D Toxicity Is Treated
Treatment follows directly from the mechanism: the harm is being done by high calcium driven by an overload of vitamin D, so the plan is to stop the source, bring the calcium down, and let the body clear the stored vitamin D over time. As calcium returns toward normal, the nausea and the mental fog lift — though, because vitamin D is stored in fat and released slowly, recovery can take weeks, and monitoring continues until levels are safely down.
- Stop all vitamin D — and calcium — immediately. The first and non-negotiable step is to discontinue every vitamin D and calcium supplement, and to review the diet for hidden sources. This alone resolves milder cases over time.
- Rehydrate. Because high calcium causes water loss and dehydration (which itself worsens nausea and confusion), generous fluids — oral in mild cases, intravenous saline in significant hypercalcemia — both treat the dehydration and help the kidneys flush calcium out. This is the cornerstone of treating symptomatic high calcium.
- Lower the calcium with medication when needed. For more pronounced hypercalcemia, doctors may add drugs that pull calcium down: bisphosphonates (which block calcium release from bone), calcitonin (a faster-acting but temporary measure), and, specifically useful in vitamin D–driven and granulomatous hypercalcemia, corticosteroids such as prednisone, which reduce vitamin D–mediated calcium absorption.
- Hospital care for severe cases. Very high calcium with marked confusion, persistent vomiting, kidney injury, or heart-rhythm changes is treated in hospital, occasionally with dialysis in the most extreme situations.
- Protect against a recurrence. Once recovered, the practical lesson is to take vitamin D only at sensible doses, to avoid stacking multiple supplements, and — for anyone on high-dose vitamin D for a medical reason — to have calcium and vitamin D monitored as advised. Avoiding sun is never the answer; the body cannot overdose on sunlight.
The encouraging news is that, caught in time, vitamin D toxicity is treatable and the nausea and confusion are reversible once calcium is corrected. The danger lies in not recognizing it — in continuing the offending supplement while blaming a stomach bug or stress — which is exactly why the supplement history and a simple calcium test matter so much.
When to Seek Care / Red Flags
Most nausea and fogginess is benign and passes on its own. But the following features mean you should be evaluated promptly — and the ones marked urgent warrant emergency care, not a wait-and-see at home:
- Nausea or fog while taking high-dose vitamin D. If you have been taking large doses of vitamin D (well beyond a standard multivitamin) and feel persistently queasy, off your food, constipated, or foggy, stop the supplement and arrange a calcium and vitamin D blood test.
- Marked confusion, disorientation, or unusual drowsiness — urgent. A genuinely confused, hard-to-rouse, or disoriented person needs same-day medical assessment, because severe hypercalcemia (from any cause) is a medical emergency — and so are many of its mimics, such as infection or a stroke.
- Persistent vomiting or signs of dehydration — inability to keep fluids down, very little urine, dizziness on standing — especially alongside intense thirst and frequent urination.
- Severe abdominal pain — could signal pancreatitis, which high calcium can trigger.
- Confusion plus a fast, pounding, or irregular heartbeat, or chest discomfort — urgent, as very high calcium can disturb the heart’s rhythm.
- New confusion in an older adult — always worth prompt assessment regardless of the suspected cause, since infection, medication, and electrolyte problems (including high calcium) are all common and treatable.
The single most useful thing you can do is to bring your supplement bottles — or a clear list of everything you take and the doses — to the appointment. The diagnosis of vitamin D toxicity often hinges on that history, and it transforms a baffling case of nausea and confusion into one quick, answerable question. When in doubt, get the calcium checked; it is a simple, decisive test.
Key Research Papers
- Galior K, Grebe S, Singh R (2018). Development of Vitamin D Toxicity from Overcorrection of Vitamin D Deficiency: A Review of Case Reports. Nutrients;10(8):953. — DOI: 10.3390/nu10080953
- Jacobus CH, Holick MF, Shao Q, et al. (1992). Hypervitaminosis D Associated with Drinking Milk. New England Journal of Medicine;326(18):1173-1177. — DOI: 10.1056/NEJM199204303261801
- Holick MF (2007). Vitamin D Deficiency. New England Journal of Medicine;357(3):266-281. — DOI: 10.1056/NEJMra070553
- Holick MF, Binkley NC, Bischoff-Ferrari HA, et al. (2011). Evaluation, Treatment, and Prevention of Vitamin D Deficiency: an Endocrine Society Clinical Practice Guideline. The Journal of Clinical Endocrinology & Metabolism;96(7):1911-1930. — DOI: 10.1210/jc.2011-0385
- Vieth R (1999). Vitamin D supplementation, 25-hydroxyvitamin D concentrations, and safety. The American Journal of Clinical Nutrition;69(5):842-856. — DOI: 10.1093/ajcn/69.5.842
- Pludowski P, Holick MF, Grant WB, et al. (2018). Vitamin D supplementation guidelines. The Journal of Steroid Biochemistry and Molecular Biology;175:125-135. — DOI: 10.1016/j.jsbmb.2017.01.021
- Holick MF (2017). The vitamin D deficiency pandemic: Approaches for diagnosis, treatment and prevention. Reviews in Endocrine and Metabolic Disorders;18(2):153-165. — DOI: 10.1007/s11154-017-9424-1
- Minisola S, Pepe J, Piemonte S, Cipriani C (2015). The diagnosis and management of hypercalcaemia. BMJ;350:h2723. — DOI: 10.1136/bmj.h2723
- Turner JJO (2017). Hypercalcaemia – presentation and management. Clinical Medicine;17(3):270-273. — DOI: 10.7861/clinmedicine.17-3-270
- Marcinowska-Suchowierska E, Kupisz-Urbańska M, Łukaszkiewicz J, et al. (2018). Vitamin D Toxicity – A Clinical Perspective. Frontiers in Endocrinology. — PubMed
PubMed Topic Searches
- PubMed — Vitamin D toxicity and hypercalcemia case reports
- PubMed — Hypercalcemia and gastrointestinal symptoms
- PubMed — Hypercalcemia and neuropsychiatric / mental status changes
- PubMed — Hypervitaminosis D from supplementation
- PubMed — Treatment and management of vitamin D toxicity
Connections
- Vitamin D Toxicity Symptom Hub
- Vitamin D Toxicity and Hypercalcemia
- Vitamin D Toxicity and Kidney Stones & Damage
- Vitamin D Toxicity and Thirst & Frequent Urination
- Vitamin D3 Overview
- Vitamin D3 Benefits
- Calcium
- Hypercalcemia (High Calcium) Hub
- Hypercalcemia and Fatigue & Confusion
- Vitamin K2
- Magnesium
- Kidney Disease
- Vitamin D Test (25-Hydroxyvitamin D)
- Comprehensive Metabolic Panel