Vitamin D Toxicity (Hypervitaminosis D): Hypercalcemia
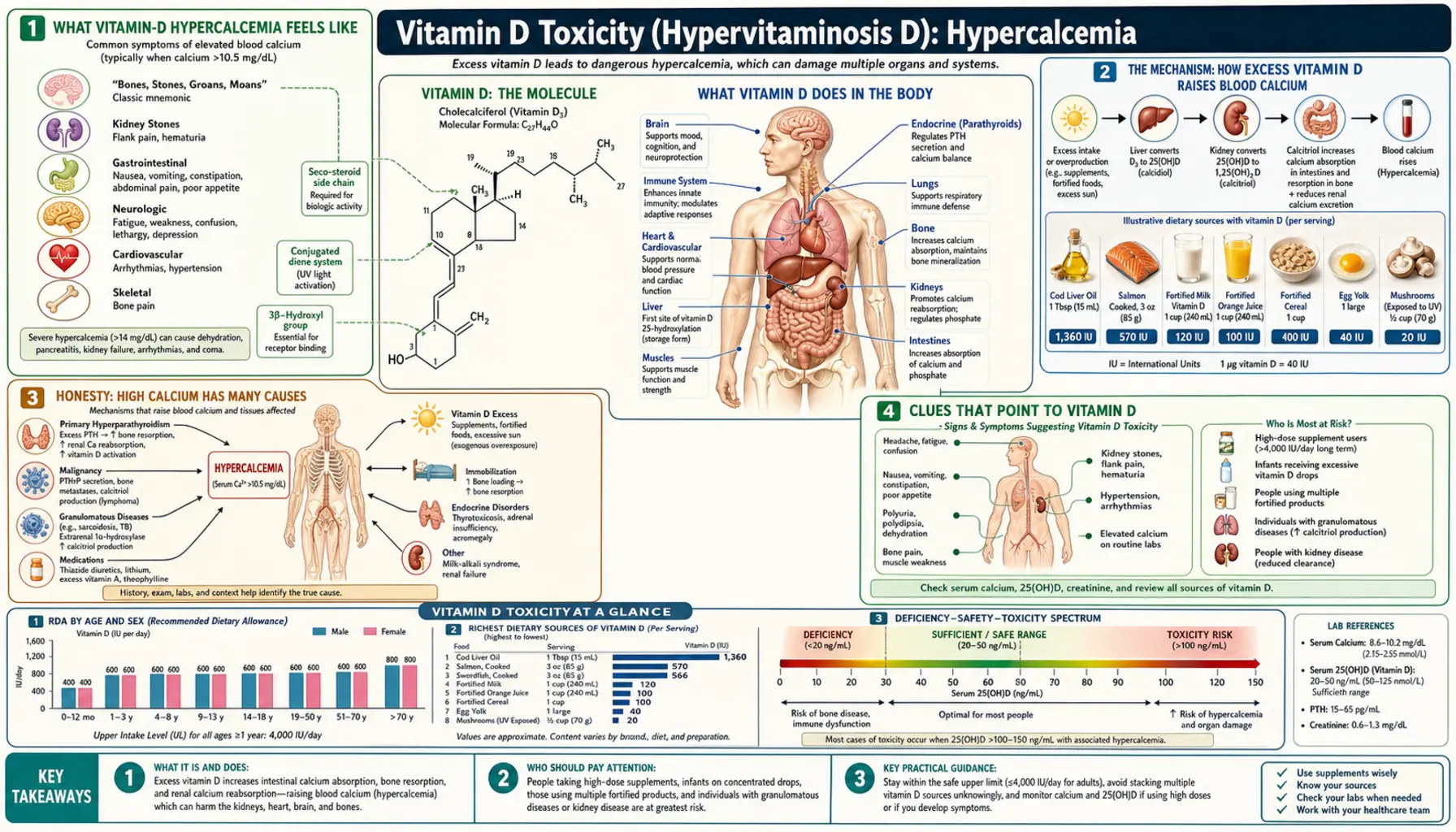
Vitamin D toxicity — doctors call it hypervitaminosis D — almost never causes harm through the vitamin itself. The damage is done by calcium. Too much vitamin D pulls more calcium out of food and out of bone than the body can manage, and blood calcium climbs into a state called hypercalcemia. That single chemistry change is what drives nearly every symptom of vitamin D poisoning: the thirst, the nausea, the confusion, the kidney damage. The reassuring part is that this is genuinely rare, and when it happens it is almost always from high-dose supplements or a manufacturing error — never from sunshine, and effectively never from food. This page explains the one chemistry change at the center of it all: how excess vitamin D raises blood calcium, what high calcium feels like, why the symptoms are vague and easy to miss, and when a high level needs urgent attention.
Table of Contents
- What Vitamin-D Hypercalcemia Feels Like
- The Mechanism: How Excess D Raises Blood Calcium
- Honesty: High Calcium Has Many Causes
- Clues That Point to Vitamin D
- How People Get Too Much Vitamin D
- How Much Is Too Much?
- Getting Checked
- How Vitamin-D Hypercalcemia Is Treated
- When to Seek Care / Red Flags
- Key Research Papers
- Connections
- Featured Videos
What Vitamin-D Hypercalcemia Feels Like
The most important thing to understand first is that mildly high calcium often causes nothing at all. Many people with early hypercalcemia feel completely normal, and the problem turns up only because someone happened to check a blood test. When symptoms do appear, they are notoriously vague — the kind of complaints that could be blamed on stress, aging, a virus, or simply a bad week — which is exactly why vitamin-D toxicity is so easy to miss.
An old medical mnemonic captures the classic picture of hypercalcemia: “stones, bones, groans, thrones, and psychiatric overtones.” Translated into plain language, that is:
- Stones — kidney stones and, over time, kidney damage from calcium depositing in the kidneys. (Covered in detail on the sibling page, Kidney Stones & Damage.)
- Bones — deep, aching bone pain, and paradoxically a weakening of bone as calcium is leached out of it.
- Groans — the gut slows down: nausea, vomiting, poor appetite, constipation, and vague abdominal pain. (See Nausea & Confusion.)
- Thrones — a reference to the toilet: high calcium makes the kidneys spill water, causing relentless thirst and heavy urination, which then drives dehydration. (See Thirst & Frequent Urination.)
- Psychiatric overtones — the brain feels the calcium too: fatigue, low mood, difficulty concentrating, irritability, and in severe cases confusion or drowsiness.
Two themes run through that whole list. First, the severity tracks roughly with how high the calcium is and how fast it rose — a calcium that climbs quickly causes more trouble than the same number reached slowly. Second, none of these symptoms is unique to vitamin D, or even unique to high calcium. That honesty matters enough to deserve its own section below. What ties them together is a single underlying fault, and the next section explains it.
The Mechanism: How Excess Vitamin D Raises Blood Calcium
To see why too much vitamin D is really a calcium problem, it helps to know what vitamin D normally does. Its main job is to keep blood calcium in a narrow, healthy range. It does this by acting like a permit office for calcium — deciding how much calcium the body lets in from food and how much it pulls from its reserves.
Vitamin D works in two steps. The vitamin D you swallow or make in skin is not active yet; it is a storage form measured on blood tests as 25-hydroxyvitamin D (25-OH-D). The body converts a small amount of that, as needed, into the truly active hormone, 1,25-dihydroxyvitamin D (calcitriol). Calcitriol then does three things that all raise blood calcium:
- It opens the gut to calcium. Its single most powerful effect is to increase how much calcium the intestine absorbs from food. Without enough vitamin D, you absorb only a small fraction of dietary calcium; with too much, the gut soaks up far more than the body needs.
- It releases calcium from bone. Working with parathyroid hormone, calcitriol prompts bone to give up some of its stored calcium into the blood — which is why vitamin-D toxicity can weaken bone even as it raises blood calcium.
- It nudges the kidney to hold onto calcium. It reduces how much calcium the kidney discards in urine, keeping more in circulation.
In normal life this permit office is tightly regulated. Crucially, the body strictly limits the second step — it makes only as much active calcitriol as it needs, and it shuts that conversion down when calcium is already adequate. That built-in brake is the reason ordinary, sensible doses of vitamin D do not cause toxicity. Sunshine cannot cause it at all, because the skin self-limits how much vitamin D it makes.
So how does toxicity happen? When someone takes enormously more vitamin D than the body can handle — over weeks or months — the storage form, 25-OH-D, piles up to extreme levels. At those concentrations the normal brakes are overwhelmed in two ways. The flood of 25-OH-D can directly stimulate the gut's calcium machinery, and it spills over the protein that normally carries vitamin D in the blood, freeing active vitamin D to flood tissues. The permit office, in effect, stops checking permits. Calcium pours in from the gut and out of bone faster than the kidneys can dump it, and blood calcium rises — hypercalcemia.
An analogy. Picture vitamin D as the thermostat for a building's heat (calcium). At a normal setting the thermostat keeps the rooms comfortable, switching the furnace on and off as needed. Vitamin-D toxicity is like jamming the thermostat to its maximum and snapping off the safety cutoff: the furnace runs flat out, the building overheats, and every room suffers — not because heat is bad, but because there is far too much of it with nothing to shut it down. Lower the setting — stop the excess vitamin D — and, slowly, the building cools.
That “slowly” is a defining feature of vitamin D, and it explains why this toxicity is so stubborn. Vitamin D is fat-soluble: the body stores it in fat and releases it gradually, so 25-OH-D has a half-life of weeks. Once it has built up, it can keep calcium high for weeks to months even after every supplement is stopped — the opposite of a water-soluble vitamin, where excess simply washes out in urine within hours.
Honesty: High Calcium Has Many Causes
This section is the heart of an honest page. High blood calcium is a real and sometimes serious finding — but vitamin D excess is an uncommon cause of it. Far more often, a high calcium has nothing to do with vitamin D at all. If your calcium comes back high, vitamin D is one possibility a clinician will consider, but it is rarely the first.
By a wide margin, the two leading causes of high calcium are:
- Primary hyperparathyroidism — an overactive parathyroid gland (usually a small benign growth) that releases too much parathyroid hormone, which drives calcium up. This is the single most common cause of high calcium in otherwise healthy outpatients, and it is treatable. See Hyperparathyroidism.
- Cancer. Several cancers raise calcium — some by secreting a hormone-like protein, others by spreading to bone. Hypercalcemia of malignancy is the most common cause of high calcium in hospitalized patients and usually points to advanced disease.
Beyond those two, other causes a doctor weighs include certain granulomatous diseases — notably sarcoidosis and tuberculosis — in which inflamed tissue makes its own active vitamin D and raises calcium (a vitamin-D-related but very different process from swallowing too much); some medications such as thiazide diuretics and lithium; an overactive thyroid; prolonged immobilization; and, historically, the “milk-alkali” pattern from swallowing large amounts of calcium with antacids.
The practical message: a high calcium is a clue, not a diagnosis. Do not assume your vitamin D supplement is the culprit, and equally, do not assume it is innocent. The job of the workup — described in the diagnosis section below — is to sort these causes apart, because the treatment for an overactive parathyroid gland is nothing like the treatment for vitamin-D overdose.
Clues That Point to Vitamin D
If hypercalcemia is found, a few features make vitamin D a more likely explanation and help separate it from the common causes above:
- A history of high-dose supplements. This is the biggest clue by far. Vitamin-D toxicity essentially always involves someone taking large amounts — often tens of thousands of international units (IU) a day for weeks or months, sometimes from a single “mega-dose” product, a compounding error, or a mislabeled supplement. Honest disclosure of everything in the supplement cabinet is the fastest route to the answer.
- A very high 25-OH-D level. In vitamin-D toxicity the storage form, 25-hydroxyvitamin D, is strikingly elevated — typically well above 150 ng/mL (375 nmol/L), and often far higher. This is the fingerprint that distinguishes vitamin-D toxicity from the other causes, in which 25-OH-D is normal or only modestly raised.
- A suppressed parathyroid hormone. When high calcium is the driver, the parathyroid glands correctly switch off, so parathyroid hormone (PTH) is low. A low PTH alongside high calcium points away from primary hyperparathyroidism (where PTH is high) and toward causes like vitamin D excess or cancer.
Put together, the signature of classic vitamin-D toxicity is: high calcium, a markedly high 25-OH-D, a suppressed PTH, and a story of large supplement doses. When some of those pieces are missing — especially a normal 25-OH-D — attention shifts to the other causes. The companion symptom pages describe how this plays out organ by organ: the kidneys, the gut and brain, and the thirst and urination of dehydration.
How People Get Too Much Vitamin D
It is worth stating plainly what does not cause vitamin-D toxicity, because the fears are usually misplaced. You cannot overdose from the sun — skin self-regulates and stops making vitamin D once it has enough. You will not develop toxicity from food; even the richest natural sources and fortified foods fall far short of toxic amounts. Standard supplement doses (the common 1,000–2,000 IU daily, or even moderately higher amounts taken under guidance) have an excellent safety record. Toxicity is a problem of large excess, and it comes from a short, recognizable list:
- High-dose over-the-counter supplements taken long-term. The most common real-world scenario is someone taking very large daily doses — far beyond what any label recommends — for weeks or months, often in a well-meaning attempt to fix a deficiency or chase an unproven benefit.
- Manufacturing and compounding errors. Several documented poisonings have come from products that contained far more vitamin D than the label claimed — sometimes hundreds of times more — or from compounding mistakes. A person can be taking a “normal” dose on paper and still be flooded with vitamin D.
- Dosing mistakes and confusion. Mixing up “daily” and “weekly” high-dose prescriptions, taking a once-a-month formulation every day, or misreading a dropper concentration can deliver a large unintended dose. This is a particular risk with very concentrated liquid drops for infants.
- Prescription metabolites. Active vitamin D drugs used for specific medical conditions (such as kidney disease) are far more potent than the storage form and can cause hypercalcemia more readily if doses are not carefully monitored. These require regular blood checks for exactly this reason.
The thread connecting all of these is amount, not the vitamin itself. Vitamin D is safe across a wide range; trouble begins only when the dose climbs far past sensible limits, usually because someone assumed — understandably but wrongly — that if a little is good, a lot must be better.
How Much Is Too Much?
Numbers help put the risk in perspective, though they are guides, not bright lines — tolerance varies from person to person.
For blood levels, sufficiency is generally considered a 25-OH-D of about 20–50 ng/mL (50–125 nmol/L). Most experts regard levels above roughly 100 ng/mL (250 nmol/L) as excessive and potentially harmful, and frank toxicity with hypercalcemia is usually seen at levels well above 150 ng/mL (375 nmol/L) — often much higher. Reaching those levels essentially requires sustained high-dose supplementation.
For intake, the U.S. Institute of Medicine set the Tolerable Upper Intake Level for most adults at 4,000 IU per day — the amount judged safe for nearly everyone over the long term, with a deliberate safety margin built in. That margin is generous: the upper level is not a poisoning threshold but a conservative ceiling, and brief or modest excursions above it under medical guidance are not the same as toxicity. Documented poisonings, by contrast, generally involve tens of thousands of IU daily sustained over time, or a contaminated product delivering a comparable load. The gap between the cautious upper level and an actually toxic dose is wide — which is both why standard doses are safe and why genuine toxicity almost always reflects a large, prolonged, or accidental overdose rather than ordinary use.
The takeaway is balance, not alarm. There is no need to fear a normal supplement; there is good reason not to self-prescribe extreme doses for months without a blood test. If you take a higher dose for any reason, it should be with a clinician who checks your 25-OH-D and calcium periodically.
Getting Checked
Sorting out high calcium is straightforward and rests on a small set of blood tests, interpreted together. The point is not just to confirm hypercalcemia but to identify why it is high — because, as the honesty section explained, the causes are treated in completely different ways.
The core tests are:
- Serum calcium — the starting point, usually found on a routine Comprehensive Metabolic Panel. Because nearly half of blood calcium rides on the protein albumin, the result is “corrected” for the albumin level, and an ionized calcium (the free, active fraction) may be measured directly when precision matters.
- Parathyroid hormone (PTH) — the single most useful next test. A high PTH with high calcium points to primary hyperparathyroidism; a suppressed PTH points away from the parathyroid and toward causes such as vitamin D excess, cancer, or granulomatous disease.
- 25-hydroxyvitamin D — the vitamin D blood test, and the key to confirming vitamin-D toxicity specifically. A markedly elevated 25-OH-D (well above 150 ng/mL) with high calcium and low PTH is the classic toxicity pattern.
- Kidney function and related chemistries — creatinine and electrolytes show whether the high calcium has begun to injure the kidneys or cause dehydration; phosphate and, in selected cases, the active 1,25-dihydroxyvitamin D level help distinguish granulomatous causes.
If these point to vitamin D and the source is not obvious, the next step is a careful review of every supplement, drop, and prescription — including doses, frequency, and exact products — because contaminated or mis-dosed products are a recurring culprit. When the picture suggests cancer or sarcoidosis instead, imaging and other targeted tests follow.
How Vitamin-D Hypercalcemia Is Treated
Treatment depends on how high the calcium is and how sick the person feels, and it always includes finding and stopping the source. The reassuring news is that, handled properly, even severe vitamin-D hypercalcemia is usually reversible — though because vitamin D lingers in the body for weeks, recovery can be slow and needs follow-up.
- Stop the vitamin D — and the calcium. The first and essential step is to discontinue all vitamin D supplements and any active vitamin D drugs, and usually to cut dietary calcium and calcium supplements as well. On its own, in mild cases, this may be enough — but because stored vitamin D keeps releasing for weeks, the calcium can stay high for a while after stopping.
- Rehydrate. High calcium causes heavy urination and dehydration, which in turn makes the calcium climb higher. Generous fluids — oral in mild cases, intravenous saline in more serious ones — restore volume and help the kidneys flush calcium out. This is the workhorse of treatment for significant hypercalcemia.
- Medications to lower calcium. When calcium is dangerously high or symptoms are severe, hospital treatment may add drugs that pull calcium down. Glucocorticoids (steroids such as prednisone) are particularly useful in vitamin-D-mediated hypercalcemia because they reduce gut calcium absorption and the production of active vitamin D. Bisphosphonates (and, in selected cases, calcitonin) curb the release of calcium from bone. The specific combination is chosen by the medical team.
- Treat complications and monitor. Care includes protecting the kidneys, correcting other electrolytes, and — importantly — repeated calcium and 25-OH-D checks over the following weeks to months, since the stored vitamin D continues to wash out slowly.
Prevention, of course, is far easier than treatment: take vitamin D in sensible doses, treat a true deficiency under guidance with periodic blood checks rather than guesswork, buy supplements from reputable sources, and be especially careful measuring concentrated liquid drops.
When to Seek Care / Red Flags
Mild hypercalcemia is usually managed without urgency, but certain features mean a high calcium — or a suspicion of one — needs prompt or emergency attention. Seek care without delay for any of the following:
- Confusion, marked drowsiness, or a change in alertness — the brain effects of very high calcium can progress to stupor and are a medical emergency. Severe lethargy or someone who is hard to rouse warrants emergency services.
- Persistent vomiting with inability to keep fluids down — this drives dehydration, which pushes calcium higher in a dangerous spiral and may need intravenous fluids.
- Signs of significant dehydration — relentless thirst, very dark or scant urine, dizziness on standing, or fainting (see Thirst & Frequent Urination).
- Heart rhythm symptoms — palpitations, a very slow or irregular pulse, or chest discomfort, since severe hypercalcemia can disturb the heart's electrical rhythm.
- Severe bone pain, flank pain, or signs of a kidney stone — sharp pain in the back or side, or blood in the urine (see Kidney Stones & Damage).
- Knowing you have taken high-dose vitamin D — tens of thousands of IU daily, a mega-dose product, or a suspected mislabeled supplement — plus any new symptoms above. This combination warrants a prompt calcium and 25-OH-D check even if you feel only mildly off.
The dangerous pattern is high calcium with confusion, vomiting, and dehydration together, because each worsens the others. When in doubt, be seen: confirming or ruling out significant hypercalcemia takes a simple blood test, and catching it early — before the kidneys or the brain are affected — is the entire point.
Key Research Papers
- Marcinowska-Suchowierska E, Kupisz-Urbańska M, Łukaszkiewicz J, et al. (2018). Vitamin D Toxicity—A Clinical Perspective. Frontiers in Endocrinology;9:550. — DOI: 10.3389/fendo.2018.00550
- Tebben PJ, Singh RJ, Kumar R (2016). Vitamin D-Mediated Hypercalcemia: Mechanisms, Diagnosis, and Treatment. Endocrine Reviews;37(5):521-547. — DOI: 10.1210/er.2016-1070
- Galior K, Grebe S, Singh R (2018). Development of Vitamin D Toxicity from Overcorrection of Vitamin D Deficiency: A Review of Case Reports. Nutrients;10(8):953. — DOI: 10.3390/nu10080953
- Jones G (2008). Pharmacokinetics of vitamin D toxicity. The American Journal of Clinical Nutrition;88(2):582S-586S. — DOI: 10.1093/ajcn/88.2.582S
- Vieth R (1999). Vitamin D supplementation, 25-hydroxyvitamin D concentrations, and safety. The American Journal of Clinical Nutrition;69(5):842-856. — DOI: 10.1093/ajcn/69.5.842
- Holick MF (2007). Vitamin D Deficiency. New England Journal of Medicine;357(3):266-281. — DOI: 10.1056/NEJMra070553
- Holick MF, Binkley NC, Bischoff-Ferrari HA, et al. (2011). Evaluation, Treatment, and Prevention of Vitamin D Deficiency: an Endocrine Society Clinical Practice Guideline. The Journal of Clinical Endocrinology & Metabolism;96(7):1911-1930. — DOI: 10.1210/jc.2011-0385
- Ross AC, Manson JE, Abrams SA, et al. (2011). The 2011 Report on Dietary Reference Intakes for Calcium and Vitamin D from the Institute of Medicine: What Clinicians Need to Know. The Journal of Clinical Endocrinology & Metabolism;96(1):53-58. — DOI: 10.1210/jc.2010-2704
- Rooney MR, Harnack L, Michos ED, et al. (2017). Trends in Use of High-Dose Vitamin D Supplements Exceeding 1000 or 4000 International Units Daily, 1999-2014. JAMA;317(23):2448-2450. — DOI: 10.1001/jama.2017.4392
- Stewart AF (2005). Hypercalcemia Associated with Cancer. New England Journal of Medicine;352(4):373-379. — DOI: 10.1056/NEJMcp042806
- Bilezikian JP, Bandeira L, Khan A, Cusano NE (2018). Primary hyperparathyroidism. Nature Reviews Disease Primers;2:16033. — DOI: 10.1038/nrdp.2016.33
- National Institutes of Health, Office of Dietary Supplements. Vitamin D — Health Professional Fact Sheet (safety and upper intake levels). — PubMed
PubMed Topic Searches
- PubMed — Vitamin D toxicity and hypercalcemia
- PubMed — Hypervitaminosis D case reports (supplements)
- PubMed — 25-hydroxyvitamin D toxicity thresholds
- PubMed — Hypercalcemia differential diagnosis and PTH
- PubMed — Treatment of vitamin D intoxication
Connections
- Vitamin D Toxicity Hub
- Vitamin D Toxicity and Kidney Stones & Damage
- Vitamin D Toxicity and Nausea & Confusion
- Vitamin D Toxicity and Thirst & Frequent Urination
- Vitamin D Deficiency Hub
- Vitamin D3 Overview
- Vitamin D3 and Bone Health
- Calcium
- Vitamin D Blood Test
- Comprehensive Metabolic Panel
- Hyperparathyroidism
- Sarcoidosis
- Kidney Stones
- Kidney Disease