Seed Oils: Canola, Soybean, Sunflower, Corn — What the Evidence Actually Says

Few topics in modern nutrition have generated as much heated public debate as seed oils — industrial vegetable oils extracted from seeds and grains including soybean, canola (rapeseed), corn, sunflower, safflower, cottonseed, grapeseed, and rice bran. Proponents of avoidance argue that the high linoleic-acid (omega-6) content, industrial extraction with hexane, oxidation during high-heat cooking, and their pervasive presence in ultra-processed foods make them a major driver of chronic inflammation and metabolic disease. Defenders cite long-term randomized trials of linoleic acid reducing cholesterol and cardiovascular risk. The truth, as usual, is considerably more nuanced than either camp acknowledges.
This article sorts through what is well-established, what is contested, and what the practical takeaway should be for someone trying to eat well without getting lost in social-media shouting matches.
Table of Contents
- What Seed Oils Are
- The Linoleic Acid Debate
- Omega-6 to Omega-3 Ratio
- Heating, Oxidation, and Aldehydes
- Industrial Processing
- The Ultra-Processed-Food Confounder
- The Randomized-Trial Evidence
- Practical Recommendations
- Connections
- Featured Videos
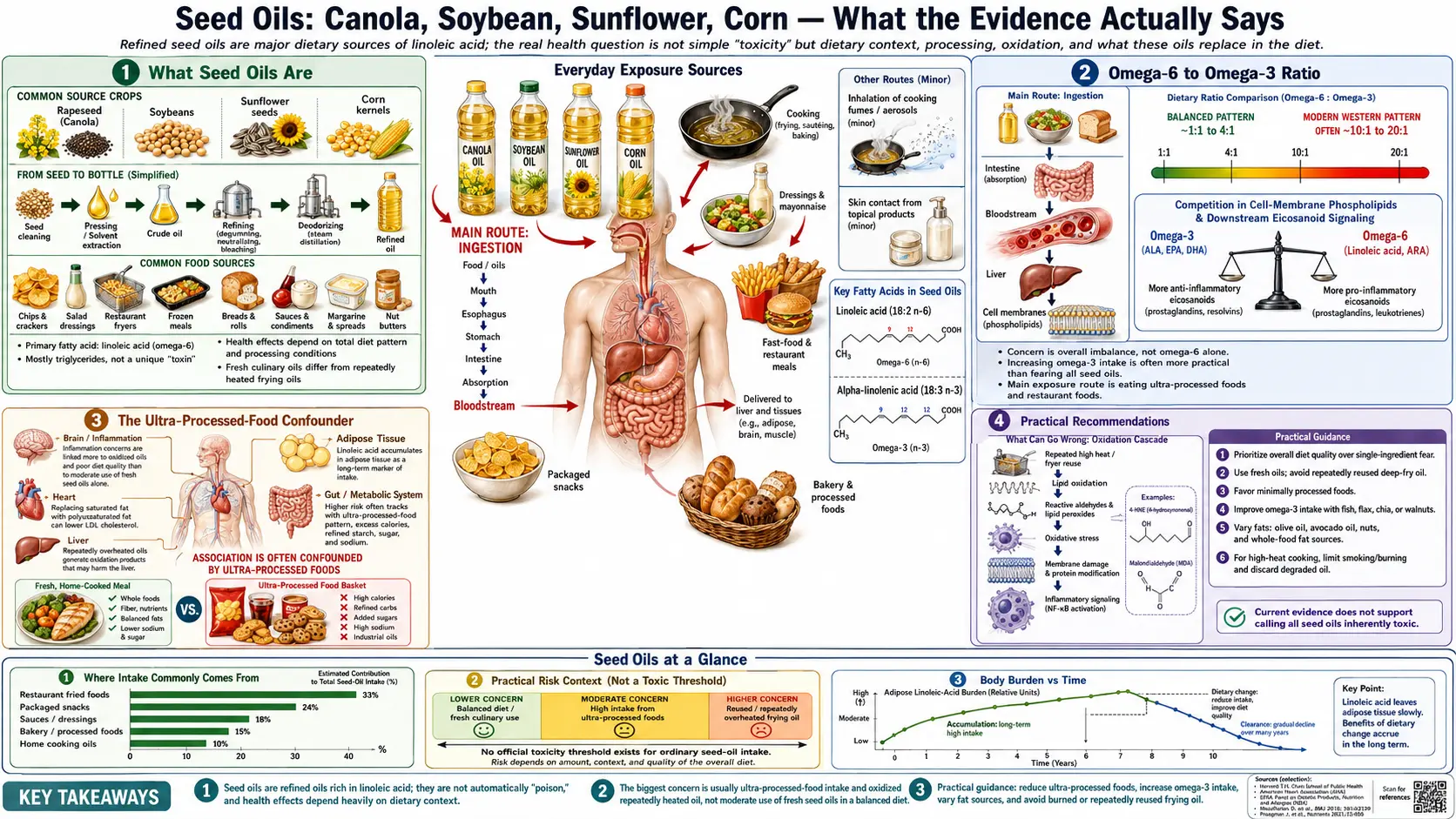
What Seed Oils Are
“Seed oils” in contemporary discourse usually refers to eight industrial oils — soybean, canola, corn, cottonseed, sunflower, safflower, grapeseed, and rice bran — that share high polyunsaturated (mostly linoleic-acid) content and industrial solvent-extraction processes. They are inexpensive, have neutral flavor, and tolerate high-heat cooking adequately, which is why they dominate restaurant fryers, shelf-stable salad dressings, and virtually all ultra-processed food production.
The Linoleic Acid Debate
Linoleic acid (LA) is the short-chain omega-6 polyunsaturated fatty acid. It is essential — the body cannot synthesize it — and small amounts are required for skin barrier function and arachidonic-acid synthesis. Intake in the United States has risen roughly three-fold since 1900, driven almost entirely by industrial oil consumption. Critics argue this massive dietary shift has produced unprecedented tissue LA levels that drive chronic inflammation, insulin resistance, and obesity. Defenders point to multiple randomized controlled trials (the Minnesota Coronary Experiment, the Sydney Diet Heart Study, modern meta-analyses of linoleic-acid replacement of saturated fat) showing reduced LDL cholesterol and, in most analyses, reduced cardiovascular events.
Omega-6 to Omega-3 Ratio
Traditional diets had omega-6 to omega-3 ratios of roughly 1:1 to 4:1. Modern Western diets average 15:1 to 25:1. Omega-3 and omega-6 pathways compete for the same elongation enzymes; high omega-6 intake reduces conversion of plant omega-3 (ALA) to the biologically active EPA and DHA. Whether the absolute increase in omega-6 is harmful or the relative deficit of omega-3 is the main driver is unsettled. Most integrative clinicians focus on increasing omega-3 (fatty fish, fish oil, algal EPA/DHA) while modestly reducing omega-6 intake — a strategy that is well-supported regardless of one’s position in the seed-oil debate.
Heating, Oxidation, and Aldehydes
Polyunsaturated fats are more prone to oxidation than saturated or monounsaturated fats. When repeatedly heated — as in commercial deep fryers that reuse oil for days — seed oils generate lipid peroxides, 4-hydroxynonenal (4-HNE), and other reactive aldehydes that are measurably harmful in cell and animal studies. This is a legitimate concern specifically for repeatedly reused restaurant fryer oil and for home cooking that pushes oils past their smoke point. Fresh oils used once at moderate temperatures generate much smaller quantities of these compounds.
Industrial Processing
Most industrial seed oils are extracted with hexane solvent, bleached with clay, deodorized with steam at high temperature, and stabilized with antioxidants. Trace residues of hexane remain well below regulatory limits. Mechanically expelled cold-pressed versions exist for some oils (cold-pressed sunflower, expeller-pressed canola) and avoid solvent extraction but retain the omega-6 profile.
The Ultra-Processed-Food Confounder
This is the most important point in the whole debate. Seed-oil-rich foods are overwhelmingly ultra-processed foods — packaged snacks, industrial baked goods, fast food, salad dressings, spreads. Any epidemiological association between seed-oil intake and chronic disease is badly confounded by refined carbohydrates, added sugars, emulsifiers, artificial flavors, and low fiber. The causal question “are seed oils harmful at isolation, or are they simply a marker of ultra-processed food intake?” is very hard to answer from observational data alone.
The Randomized-Trial Evidence
The largest meta-analyses of randomized trials replacing saturated fat with seed-oil polyunsaturated fat show reduced cardiovascular events and mortality. Reanalyses of the Minnesota Coronary Experiment and Sydney Diet Heart Study have been disputed but remain the strongest negative signal. The preponderance of randomized evidence does not support the strongest claims of seed-oil advocates (“seed oils are the primary cause of chronic disease”), but it also does not refute the narrower claims (“extremely high intake, especially of repeatedly heated fryer oils, is harmful”).
Practical Recommendations
- Don’t eat deep-fried restaurant food often. Recycled fryer oil is the highest-aldehyde exposure scenario by far.
- Choose olive oil, avocado oil, or butter for home cooking. Extra-virgin olive oil tolerates medium-heat cooking well.
- Reserve seed oils for occasional and moderate-heat use, not as the default kitchen oil.
- Eat fatty fish or take a quality omega-3 supplement to raise EPA/DHA and lower the effective omega-6 to omega-3 ratio.
- Reduce ultra-processed foods broadly. This alone will cut seed-oil intake substantially.
- Don’t fixate. Someone who cooks whole-food meals at home with olive oil and occasionally eats a salad at a restaurant dressed with canola oil is not sabotaging their health.
Connections
- Ultra Processed Foods
- Olive Oil
- Avocado
- Anti-Inflammatory Diet
- Processed Oils
- Cardiovascular Disease
- Inflammatory Markers
- Omega-3 Fatty Acids
- Lipid Panel
- Insulin Resistance
- Obesity
- Food Additives
- Trans Fats