Tinnitus — Benefits Deep Dive
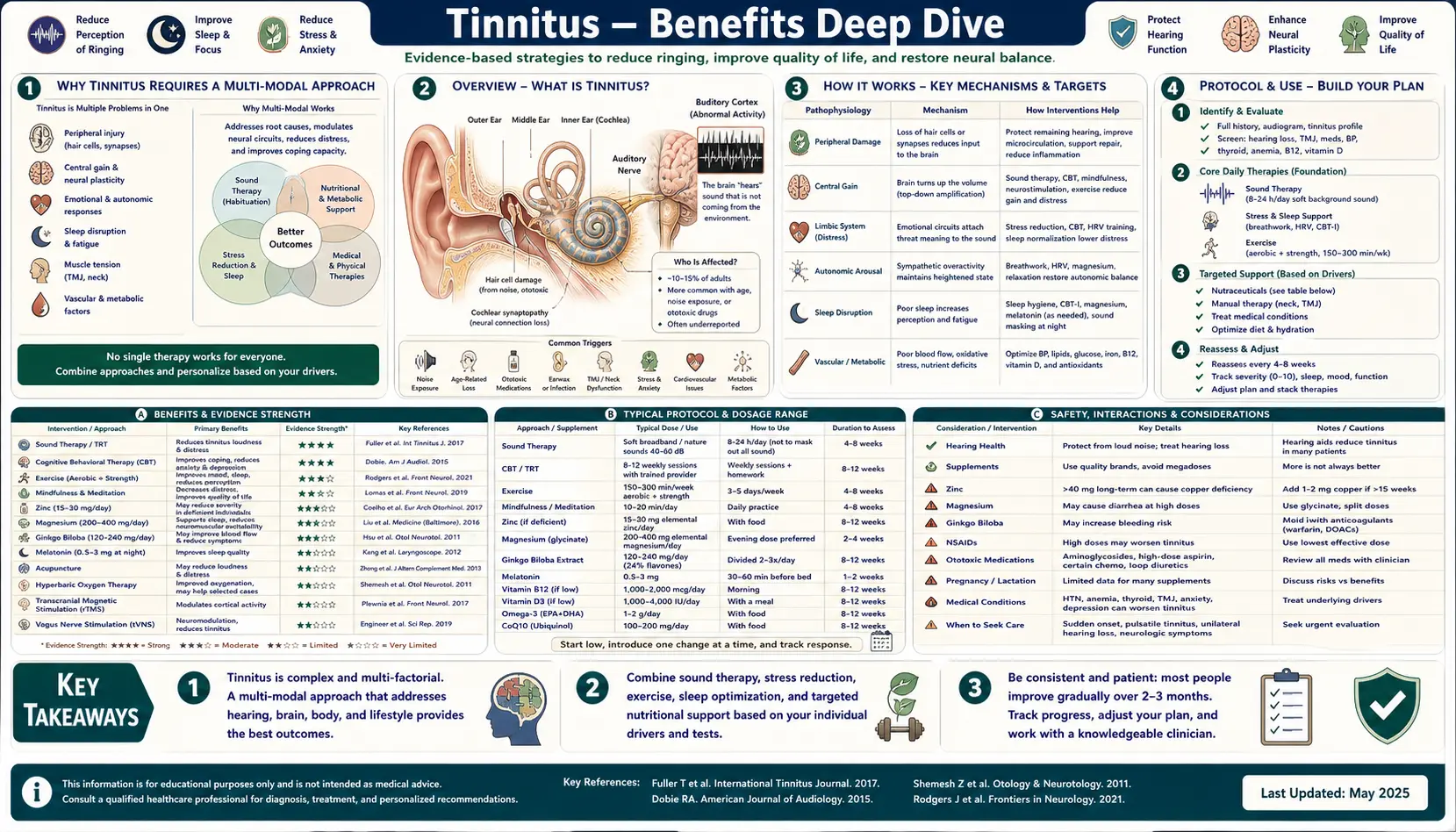
Tinnitus — the phantom perception of ringing, buzzing, hissing, or pulsing sound in the absence of an external acoustic source — affects roughly 10–15% of the global adult population and produces moderate-to-severe distress in approximately 1–2%. Despite its prevalence, tinnitus is not a disease in itself but a symptom, generated by central auditory-cortex hyperactivity that follows cochlear injury, ototoxic exposure, vascular dysfunction, cervical-spine misalignment, temporomandibular-joint dysfunction, or metabolic deficiency. The four deep-dive pages below cover the conditions and interventions where the evidence base is strongest: identifying the mechanistic cause and modifiable trigger profile, the specific micronutrient deficiencies (B12, magnesium, zinc) that produce reversible tinnitus, the sound-therapy and habituation paradigm that constitutes the gold-standard non-pharmacologic management, and the role of N-acetylcysteine and antioxidants in protecting cochlear hair cells from oxidative injury that initiates and perpetuates the phantom percept.
Deep-Dive Articles
Causes & Triggers
The mechanistic taxonomy of tinnitus — noise-induced cochlear damage, presbycusis, ototoxic medication (salicylates, aminoglycosides, loop diuretics, cisplatin), Meniere's disease, otosclerosis, vestibular schwannoma, temporomandibular joint dysfunction, cervical-spine misalignment, vascular and pulsatile causes, and the central plasticity that converts peripheral cochlear injury into chronic auditory-cortex hyperactivity. Includes the modifiable trigger list: caffeine, sodium, nicotine, alcohol, sleep deprivation, and stress.
B12, Magnesium & Zinc Status
The three micronutrient deficiencies most consistently associated with tinnitus in case-control studies. Vitamin B12 deficiency damages the myelin sheath of the cochlear nerve and produces reversible tinnitus in approximately 40% of B12-deficient cases. Magnesium attenuates noise-induced cochlear hair-cell injury through NMDA-receptor antagonism. Zinc deficiency is documented in 30% of severe-tinnitus patients in NHANES analyses, and zinc-replete patients have reduced tinnitus loudness on validated questionnaires.
Sound Therapy & Habituation
Tinnitus Retraining Therapy (TRT), masking devices, notched-music therapy, hearing-aid amplification for the most common comorbid condition (sensorineural hearing loss), and cognitive-behavioral therapy — the four interventions with the largest effect sizes in Cochrane reviews. The Jastreboff neurophysiologic model explains why habituation rather than suppression is the therapeutic target, and why most patients ultimately learn to ignore the phantom signal even when its peripheral driver cannot be cured.
NAC & Antioxidants
N-acetylcysteine (NAC) as a glutathione precursor that protects cochlear hair cells from the oxidative burst produced by acoustic overexposure, ototoxic chemotherapy, and aminoglycoside antibiotics. Reviews the military trials of pre-exposure NAC for impulse-noise injury, the cisplatin-otoprotection trials, and the role of alpha-lipoic acid, coenzyme Q10, idebenone, and Vitamin E in maintaining cochlear redox balance. Also covers Ginkgo biloba (EGb 761) and the equivocal Cochrane verdict.
Table of Contents
- Deep-Dive Articles
- Why Tinnitus Requires a Multi-Modal Approach
- Research Papers: Causes and Mechanism
- Research Papers: Nutritional Status (B12, Mg, Zn)
- Research Papers: Sound Therapy and Habituation
- Research Papers: NAC and Antioxidants
- Research Papers: Cross-Cutting (Epidemiology, Comorbidities)
- External Authoritative Resources
- Connections
- Featured Videos
Why Tinnitus Requires a Multi-Modal Approach
Tinnitus is unusual in clinical medicine because it is a symptom rather than a disease, the perceived signal originates in the brain rather than the ear, and the most effective management strategies are non-pharmacologic. No FDA-approved drug specifically treats tinnitus. The combinations of interventions that work best for any given patient depend on identifying which causal pathway is dominant in that individual.
- Peripheral cochlear injury — noise exposure, ototoxic medication, presbycusis, and Meniere's disease all damage the cochlear hair cells, reducing afferent auditory nerve input to the central auditory cortex. The cortex responds with maladaptive plasticity (similar to phantom-limb pain) that generates the phantom signal. Once the central process is established, eliminating the peripheral driver does not always resolve the phantom percept — the cortical reorganization persists. This is why prevention is more effective than treatment, and why otoprotectant antioxidants during predictable noise or ototoxic exposure have the largest mechanistic footprint.
- Central auditory-cortex hyperactivity — once established, the phantom signal can be modulated by training the brain to filter it out of conscious awareness. The Jastreboff neurophysiologic model frames tinnitus as a failure of the limbic system to demote the phantom signal to background noise. Sound therapy, Tinnitus Retraining Therapy, and cognitive-behavioral therapy all work by retraining the limbic-prefrontal filtering loop rather than by suppressing the signal itself.
- Modifiable triggers — even when the underlying cause cannot be reversed, tinnitus loudness fluctuates day-to-day in response to caffeine, sodium, alcohol, nicotine, sleep deprivation, stress, and certain medications. Identifying and eliminating individual triggers can reduce symptom burden substantially without addressing the root cause. The trigger inventory is the first step in conservative management.
- Reversible nutritional deficiencies — vitamin B12 deficiency, magnesium depletion, and zinc deficiency are each documented to cause or worsen tinnitus in repletion-responsive subsets of patients. Checking these inexpensive labs and correcting any deficiency is one of the few mechanistically-grounded interventions with the potential to eliminate tinnitus entirely in a small but real fraction of cases. See the nutrient-status deep-dive for testing protocols and dosing.
The clinical reality is that most patients with chronic tinnitus benefit from a stacked approach: trigger elimination plus nutrient repletion plus hearing-aid amplification (when sensorineural hearing loss is present) plus sound therapy plus cognitive-behavioral therapy for the distress component. No single intervention works for everyone, but the combined effect across modalities is meaningful for most.
Research Papers: Causes and Mechanism
- Eggermont JJ, Roberts LE. The neuroscience of tinnitus (Trends in Neurosciences 2004) — PubMed 15474168
- Jastreboff PJ. Phantom auditory perception (tinnitus): mechanisms of generation and perception (1990) — Search PubMed
- Henry JA et al. General review of tinnitus: prevalence, mechanisms, effects, and management (2005) — PubMed 16411806
- Bauer CA. Tinnitus (New England Journal of Medicine 2018) — Search PubMed
- Noreña AJ. An integrative model of tinnitus based on a central gain controlling neural sensitivity (2011) — Search PubMed
- Roberts LE et al. Ringing ears: the neuroscience of tinnitus (Journal of Neuroscience 2010) — Search PubMed
- Cima RFF et al. A multidisciplinary European guideline for tinnitus (HNO 2019) — Search PubMed
- De Ridder D et al. Phantom percepts: tinnitus and pain as persisting aversive memory networks (PNAS 2011) — Search PubMed
- Schaette R, McAlpine D. Tinnitus with a normal audiogram: physiological evidence for hidden hearing loss (Journal of Neuroscience 2011) — Search PubMed
- Bhatt JM et al. Prevalence, severity, exposures, and treatment patterns of tinnitus in the US (JAMA Otolaryngol 2016) — PubMed 27441392
Research Papers: Nutritional Status (B12, Mg, Zn)
- Shemesh Z et al. Vitamin B12 deficiency in patients with chronic-tinnitus and noise-induced hearing loss (1993) — Search PubMed
- Singh C et al. Role of vitamin B12 in tinnitus (Indian Journal of Otolaryngology 2016) — Search PubMed
- Cevette MJ et al. Magnesium and hearing (Journal of the American Academy of Audiology 2003) — PubMed 14655953
- Attias J et al. Oral magnesium intake reduces permanent hearing loss induced by noise exposure (1994) — Search PubMed
- Coelho CB et al. Zinc as a possible treatment for tinnitus (Progress in Brain Research 2007) — PubMed 17956802
- Person OC et al. Zinc supplementation for tinnitus (Cochrane 2016) — Search PubMed
- Berkiten G et al. Influence of vitamin B12 deficiency on the auditory brainstem response in young women (2013) — Search PubMed
- Lasisi AO et al. Plasma levels of micronutrients in tinnitus patients in a developing country (2010) — Search PubMed
- Yetiser S et al. The role of zinc in management of tinnitus (Auris Nasus Larynx 2002) — Search PubMed
- Joachims HZ et al. Oral magnesium supplementation as prophylaxis for noise-induced hearing loss in young adults (2003) — Search PubMed
Research Papers: Sound Therapy and Habituation
- Jastreboff PJ, Hazell JW. A neurophysiological approach to tinnitus: clinical implications (British Journal of Audiology 1993) — Search PubMed
- Hoare DJ et al. Sound therapy for tinnitus management: practicable options (Journal of the American Academy of Audiology 2014) — PubMed 24622858
- Sereda M et al. Sound therapy for tinnitus (Cochrane 2018) — PubMed 30589445
- Fuller T et al. Cognitive behavioural therapy for tinnitus (Cochrane 2020) — Search PubMed
- Okamoto H et al. Listening to tailor-made notched music reduces tinnitus loudness and tinnitus-related auditory cortex activity (PNAS 2010) — Search PubMed
- Tunkel DE et al. Clinical practice guideline: tinnitus (AAO-HNS 2014) — PubMed 25273878
- Hesser H et al. A systematic review and meta-analysis of randomized controlled trials of cognitive-behavioral therapy for tinnitus distress (2011) — Search PubMed
- Hobson J et al. Sound therapy (masking) in the management of tinnitus in adults (Cochrane 2012) — Search PubMed
- Searchfield GD et al. Sound therapy options for tinnitus (Frontiers in Aging Neuroscience 2017) — Search PubMed
- Conlon B et al. Bimodal neuromodulation combining sound and tongue stimulation reduces tinnitus symptoms (Science Translational Medicine 2020) — PubMed 33028707
Research Papers: NAC and Antioxidants
- Kopke RD et al. NAC for prevention of noise-induced hearing loss (Hearing Research 2007) — Search PubMed
- Lin CY et al. N-acetylcysteine against noise-induced temporary threshold shift in male workers (Hearing Research 2010) — Search PubMed
- Riga MG et al. Transtympanic injections of N-acetylcysteine for the prevention of cisplatin-induced ototoxicity (2013) — Search PubMed
- Le Prell CG et al. Free radical scavengers vitamins A, C, and E plus magnesium reduce noise trauma (Free Radical Biology 2007) — Search PubMed
- Hilton M, Stuart E. Ginkgo biloba for tinnitus (Cochrane 2013) — PubMed 23543524
- Salami A et al. Effect of EGb 761 on tinnitus and hearing loss (2010) — Search PubMed
- Henderson D et al. The role of oxidative stress in noise-induced hearing loss (Ear and Hearing 2006) — Search PubMed
- Choi CH et al. Effects of NAC on noise-induced hearing loss in chinchillas (Hearing Research 2008) — Search PubMed
- Doosti A et al. Comparison of the effects of N-acetyl-cysteine and ginseng in prevention of noise-induced hearing loss (2014) — Search PubMed
- Petersen L et al. Antioxidants and idebenone for the treatment of tinnitus: a systematic review (2019) — Search PubMed
Research Papers: Cross-Cutting (Epidemiology, Comorbidities)
- McCormack A et al. A systematic review of the reporting of tinnitus prevalence and severity (Hearing Research 2016) — PubMed 27246985
- Langguth B et al. Tinnitus: causes and clinical management (Lancet Neurology 2013) — Search PubMed
- Baguley D et al. Tinnitus (Lancet 2013) — PubMed 23827090
- Folmer RL et al. Tinnitus and insomnia (American Journal of Otolaryngology 2000) — Search PubMed
- Bhatt JM et al. Relationships between tinnitus and the prevalence of anxiety and depression (Laryngoscope 2017) — PubMed 27301552
- Bisht M, Bist SS. Ototoxicity: the hidden menace (Indian J Otolaryngol 2011) — Search PubMed
- Reavis KM et al. Noise-induced hearing loss in the military (Hearing Research 2017) — Search PubMed
- Kreuzer PM et al. Trauma-associated tinnitus (Journal of Head Trauma Rehabilitation 2014) — Search PubMed
- Levine RA. Somatic (craniocervical) tinnitus and the dorsal cochlear nucleus hypothesis (Am J Otolaryngol 1999) — PubMed 10609479
- Manche SK et al. Association of tinnitus and hearing loss in otological disorders (Indian J Otolaryngol 2016) — Search PubMed
External Authoritative Resources
- American Tinnitus Association — the primary US patient-advocacy and research-funding organization, comprehensive evidence-based resources
- NIH/NIDCD — Tinnitus (federal evidence summary and research portfolio)
- AAO-HNS Clinical Practice Guideline: Tinnitus (Tunkel 2014) — the US clinical guideline
- NICE Guideline NG155 — Tinnitus: assessment and management (UK clinical guideline)
- PubMed — All research on tinnitus treatment (50,000+ papers)
Connections
- Tinnitus Hub (Main Page)
- Causes and Triggers
- B12, Magnesium and Zinc Status
- Sound Therapy and Habituation
- NAC and Antioxidants
- Ginkgo Biloba for Tinnitus
- Glycine for Tinnitus
- Taurine for Tinnitus
- Vitamin B12
- Magnesium
- Zinc
- N-Acetyl-Cysteine
- Ginkgo Biloba
- All Remedies
- Neurology
- Tinnitus — the ENT clinical overview: symptoms, diagnostic workup, and conventional treatment these deep dives build on.