Tinnitus — Sound Therapy and Habituation
No drug has ever been FDA-approved for tinnitus. The interventions with the largest documented effect sizes in randomized trials and Cochrane reviews are not pharmacologic at all — they are sound-based and behavioral. Hearing-aid amplification, Tinnitus Retraining Therapy, sound masking, notched-music therapy, and cognitive-behavioral therapy each address a distinct component of the tinnitus experience. Their combination addresses the central neural plasticity that generates the phantom percept, the limbic-prefrontal filtering circuit that determines how distressing it feels, and the comorbid hearing loss that drives much of the underlying cortical hypersensitivity. This page walks through each modality, the Jastreboff neurophysiologic model that explains why they work, the AAO-HNS guideline recommendations, and a practical staged approach to building a personalized sound-and-behavior protocol.
Table of Contents
- The Jastreboff Neurophysiologic Model
- Hearing Aids — The Most Underused Intervention
- Tinnitus Retraining Therapy (TRT)
- Sound Masking (Bedside and Wearable)
- Notched-Music Therapy — Targeted Cortical Reorganization
- Cognitive-Behavioral Therapy (CBT)
- Bimodal Neuromodulation (Sound + Tongue Stimulation)
- The AAO-HNS Clinical Practice Guideline
- A Practical Staged Approach
- What Not to Do
- Key Research Papers
- Connections
- Featured Videos
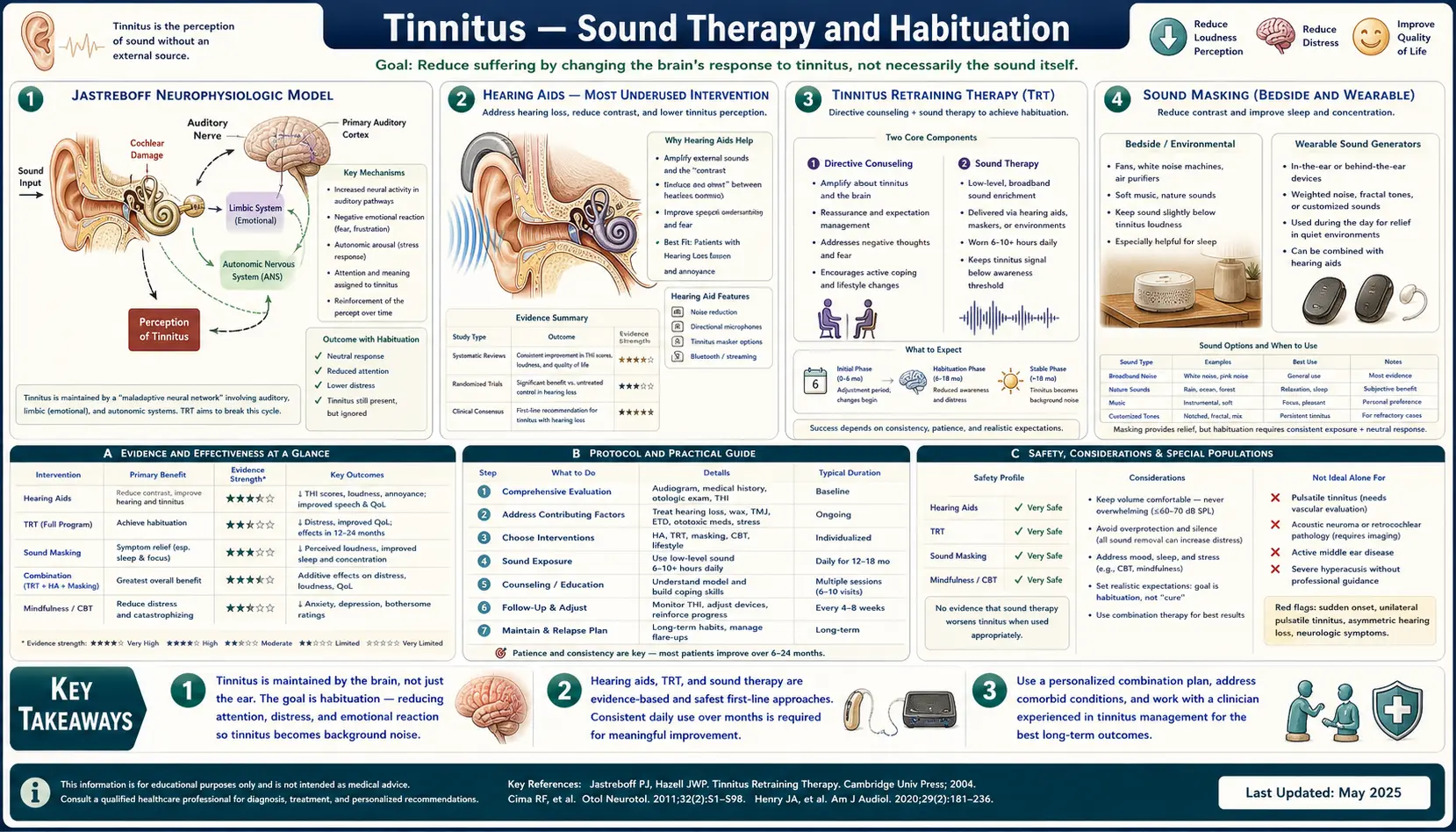
The Jastreboff Neurophysiologic Model
Pawel Jastreboff's 1990 paper in Neuroscience Research reframed tinnitus from an "ear problem" to a "brain problem," and that conceptual shift is the foundation of every sound-and-behavior intervention now in clinical use. The neurophysiologic model has three core claims:
- The phantom signal originates in the central auditory pathway, not in the cochlea, even when the inciting event was peripheral (noise injury, ototoxin, presbycusis). The cochlear damage triggers central plasticity; the plasticity then generates the phantom percept regardless of ongoing peripheral activity.
- The distress generated by tinnitus is a function of limbic-system involvement, not of the perceived loudness of the phantom signal itself. Two patients with identical audiometric tinnitus matching can have radically different functional impact — one is barely bothered, the other suicidal — depending on how much limbic activation the phantom signal generates and how the prefrontal cortex evaluates its threat significance.
- Habituation, not suppression, is the therapeutic target. The phantom signal cannot reliably be eliminated. The achievable goal is to retrain the limbic-prefrontal circuit to demote the phantom signal to background noise — to learn to ignore it the way one learns to ignore the steady hum of a refrigerator or a fan. Healthy humans habituate to thousands of irrelevant background signals every day; the tinnitus patient's limbic system has failed to do so for this particular signal, and the therapeutic task is to re-establish that habituation.
This model produces immediate clinical predictions that have been borne out:
- Sound therapy works not by drowning out the tinnitus but by providing competing stimuli that the limbic system can learn to filter alongside the phantom signal
- Counseling about the benign nature of the signal directly reduces limbic activation by removing the threat interpretation
- Stress, anxiety, and depression worsen tinnitus because they impair the prefrontal filtering circuit
- Restoring hearing through amplification reduces central gain and the underlying drive for the phantom signal
- Most patients improve substantially over 12–18 months with appropriate intervention, even when the peripheral driver of the tinnitus cannot be reversed
Hearing Aids — The Most Underused Intervention
Approximately 80% of chronic tinnitus patients have some degree of sensorineural hearing loss on audiometry, and the frequency profile of the hearing loss typically matches the perceived pitch of the tinnitus. Hearing-aid amplification — treating the underlying hearing loss — is the single most underused effective intervention in tinnitus management.
The mechanism is straightforward in the Schaette-McAlpine central-gain model. The deafferented auditory cortex turns up its gain to compensate for reduced peripheral input from the damaged frequency region; the upregulated central gain amplifies spontaneous neural activity into the phantom signal. Hearing aids restore afferent input at the deafferented frequencies, allowing the central gain to normalize downward, and the phantom signal becomes quieter and easier to ignore.
Quantitative outcomes: in the Searchfield 2017 review and subsequent meta-analyses, properly-fit hearing aids produced clinically meaningful reduction in tinnitus distress (on validated questionnaires such as the Tinnitus Handicap Inventory) in approximately 60–70% of tinnitus patients with concurrent hearing loss. Modern "combination devices" (hearing aids with integrated tinnitus-masking sound generators) extend this benefit, providing both amplification of environmental sound and a customizable low-level masking signal at the tinnitus pitch.
The crucial clinical pearl: any tinnitus patient with audiometric hearing loss should be trialed with hearing aids, even if the loss is mild and the patient does not subjectively notice impaired hearing. Insurance coverage of hearing aids has improved substantially in the US with the FDA over-the-counter hearing-aid rule (2022) allowing direct purchase for mild-to-moderate loss at much lower price points than the historical $5,000–$7,000 audiologist-channel devices.
Tinnitus Retraining Therapy (TRT)
Tinnitus Retraining Therapy is the structured clinical program built around the Jastreboff model. It has two components delivered in parallel over 12–24 months:
- Directive counseling — structured education about the neurophysiology of tinnitus, the benign nature of the signal, the habituation mechanism, and the expected timecourse. The goal is to defuse the threat interpretation that drives limbic activation. This typically involves 3–5 sessions with a TRT-trained audiologist or otolaryngologist over the first three months.
- Sound enrichment — bilateral wearable sound generators (or hearing aids with sound-generator capability) producing low-level broadband noise just below the tinnitus loudness, worn 6–8 hours per day for 12–24 months. The noise should be set at the "mixing point" where it is perceptible but does not mask the tinnitus completely — the goal is to provide a continuous background of competing auditory input for the limbic system to habituate to alongside the phantom signal.
The Henry 2005 multicenter trial documented that TRT produced significantly greater reduction in tinnitus distress than counseling-only or standard care, with effect sizes that persisted at 12-month follow-up. The intervention is intensive (typical course is 12–24 months) but the durability of benefit is substantially better than most pharmacologic approaches.
Sound Masking (Bedside and Wearable)
Sound masking is simpler than TRT — it does not require structured counseling or a specific device protocol. The principle is to provide environmental sound that reduces the perceived loudness of the tinnitus by providing competing auditory input.
The most common forms:
- Bedside sound machines — white noise, pink noise, ocean waves, rain, or fan sounds at low level throughout the sleep period. Tinnitus is most distressing at night when ambient sound drops and the phantom signal stands out against silence. A bedside masking sound reduces sleep-onset latency and night-waking frequency in most tinnitus patients with insomnia.
- Wearable sound generators — behind-the-ear or in-ear devices providing continuous low-level broadband noise during waking hours. Similar to TRT sound generators but without the formal counseling protocol.
- Smartphone-based masking apps — the modern accessible alternative; many free or low-cost apps provide customizable masking sounds. Quality varies; clinical research has been limited.
- Environmental sound enrichment — keeping a low-volume radio or background music on throughout the day; opening windows for outdoor sound; using a soft-running fan or air purifier. This is the no-cost intervention every tinnitus patient should try.
The Hobson 2012 and Sereda 2018 Cochrane reviews concluded that sound masking has favorable benefit-to-burden ratio and should be considered for any tinnitus patient. The evidence for any single device or sound type being superior to others is weak — patient preference and adherence are the dominant factors in outcomes.
Notched-Music Therapy — Targeted Cortical Reorganization
Notched-music therapy is a newer, mechanism-targeted intervention developed by Okamoto and colleagues at the University of Münster. The therapy is based on the observation that the auditory cortex demonstrates use-dependent reorganization — the cortical regions corresponding to frequently-heard frequencies expand at the expense of regions corresponding to rarely-heard frequencies. The notched-music protocol exploits this plasticity in reverse:
- The patient's individual tinnitus pitch is measured precisely with audiometric matching
- The patient's preferred music is digitally filtered to remove a one-octave-wide band of frequencies centered on the tinnitus pitch (the "notch")
- The patient listens to the notched music 1–2 hours per day for several months
- The deprivation of input at the tinnitus frequency, combined with normal input at adjacent frequencies, drives lateral-inhibition-mediated reorganization of the auditory cortex that reduces representation of the tinnitus frequency and reduces the phantom signal
Okamoto et al. (2010) demonstrated in a randomized controlled trial that 12 months of notched-music therapy produced significantly greater reduction in tinnitus loudness than control music listening, with corresponding objective changes in auditory-cortex activity measured by magnetoencephalography. The effect was specific to the notched frequency and did not occur with placebo (unfiltered) music.
The intervention is appealing because it is targeted, evidence-supported, and can be delivered through inexpensive smartphone apps. Several commercial implementations now exist. The main limitation is the requirement for precise tinnitus-pitch measurement to set the notch correctly, and the relatively long treatment duration needed to see meaningful effect.
Cognitive-Behavioral Therapy (CBT)
Cognitive-behavioral therapy is the behavioral intervention with the strongest evidence base for tinnitus — the 2020 Cochrane review (Fuller et al.) of 28 trials totaling 2,733 participants concluded that CBT produces "probable benefit" in tinnitus-related distress and quality of life with moderate-quality evidence, the highest grade among any behavioral intervention reviewed.
CBT does not aim to reduce the loudness or character of the phantom signal — that target is unrealistic. Instead, CBT targets the cognitive and emotional response to the signal:
- Cognitive restructuring — identifying and challenging catastrophic thoughts about tinnitus ("I will never have a moment of peace again," "I cannot live with this"), replacing them with more accurate appraisals ("This is a benign signal that fluctuates and that most people learn to ignore over time")
- Behavioral activation — restoring engagement with previously enjoyable activities that the patient may have abandoned because of tinnitus-related distress
- Relaxation and stress-reduction training — progressive muscle relaxation, diaphragmatic breathing, mindfulness; these directly reduce the limbic activation that amplifies tinnitus perception
- Sleep-hygiene optimization — addressing the bidirectional relationship between tinnitus and insomnia
- Attention-modification training — structured exercises that practice shifting attention away from the tinnitus signal
CBT is delivered in 6–12 weekly sessions, individually or in group format. Internet-delivered CBT for tinnitus (iCBT) has shown effect sizes comparable to face-to-face CBT in several randomized trials, making it accessible to patients who cannot easily access a tinnitus-experienced therapist.
Bimodal Neuromodulation (Sound + Tongue Stimulation)
Bimodal neuromodulation is the most promising emerging intervention. The Conlon et al. (2020) Science Translational Medicine trial of the Lenire device tested a paired-stimulation paradigm in which patients received synchronized auditory tones (matched to their tinnitus frequency) plus mild electrical stimulation of the tongue surface for 60 minutes daily over 12 weeks. The pairing exploits cross-modal cortical plasticity to drive directed reorganization of the dorsal cochlear nucleus and auditory cortex.
Results in the pivotal trial of 326 tinnitus patients:
- 86% of treated patients showed clinically meaningful reduction in Tinnitus Handicap Inventory scores
- The mean THI reduction was 14 points (well above the 7-point minimum clinically important difference)
- Benefits persisted at 12-month follow-up
- Adverse events were minor (mild tongue discomfort during stimulation in a minority)
The Lenire device received FDA De Novo authorization in 2023 for tinnitus treatment and is commercially available, though insurance coverage in the US is still developing. Cost is approximately $4,000–$5,000 for the device and protocol. Other bimodal devices using different cross-modal pairings (auditory + cervical stimulation, auditory + transcranial stimulation) are in development.
The AAO-HNS Clinical Practice Guideline
The 2014 Tunkel et al. AAO-HNS clinical practice guideline (updated several times since) is the US-consensus reference for tinnitus management. Its key recommendations, ranked by strength of recommendation:
- Strong recommendation: Hearing-aid evaluation for patients with persistent bothersome tinnitus and documented hearing loss
- Strong recommendation: Cognitive-behavioral therapy for patients with persistent bothersome tinnitus
- Strong recommendation against: Routine use of medications, dietary supplements, transcranial magnetic stimulation, or acupuncture for chronic tinnitus — not because they are dangerous but because the evidence base does not support generalized use
- Recommendation: Sound therapy for patients with persistent bothersome tinnitus
- Recommendation: Comprehensive audiologic exam at initial evaluation; MRI for unilateral or pulsatile tinnitus
- Option: Tinnitus Retraining Therapy for patients meeting selection criteria and willing to commit to the long course
Notably absent from the recommendations: any specific pharmacologic agent. Benzodiazepines, SSRIs, gabapentin, and other drugs are sometimes prescribed for tinnitus but the AAO-HNS guideline does not endorse routine use. Their role is limited to treating the comorbid anxiety, depression, and insomnia that often accompany severe tinnitus, not the phantom signal itself.
A Practical Staged Approach
For a new patient with chronic bothersome tinnitus, a reasonable staged approach:
- Month 1 — complete workup (history, otoscopy, audiometry, MRI if indicated, nutrient labs per the nutrient deep-dive); modifiable trigger inventory per the causes and triggers page; introduce bedside sound masking for sleep; provide directive counseling about the benign nature of tinnitus and the habituation process
- Months 2–3 — correct any documented nutrient deficiencies; trial hearing aids if audiometric loss documented (the FDA OTC hearing-aid pathway makes a 30-day trial low-cost); add environmental sound enrichment during the day; begin CBT or iCBT (6–12 sessions)
- Months 4–6 — reassess response to first-line interventions; if substantial distress persists, consider TRT enrollment with a trained audiologist or notched-music therapy as an alternative sound-based approach
- Months 6–12 — if refractory to above, consider bimodal neuromodulation (Lenire) or trial of off-label pharmacologic options for comorbid distress (low-dose nortriptyline, SSRI, gabapentin for sleep); maintain the foundation of sound enrichment and CBT throughout
- Beyond 12 months — expect substantial habituation in most patients regardless of specific intervention; the natural history of tinnitus is toward gradual improvement in distress (even when loudness does not change) over 18–24 months with consistent management
What Not to Do
- Do not advise the patient that "nothing can be done" — this is both inaccurate and clinically harmful. Even patients who do not respond to specific interventions habituate substantially over time with appropriate framing and support.
- Do not start chronic benzodiazepines — while clonazepam acutely reduces tinnitus perception in some patients, chronic use produces dependence, cognitive impairment, and rebound worsening of tinnitus on attempted discontinuation. Use only short-term for acute distress.
- Do not promote silence — patients often cope with tinnitus by avoiding loud environments and seeking silence; this worsens the tinnitus by reducing the competing auditory input the limbic system needs for habituation. Encourage environmental sound enrichment instead.
- Do not over-investigate stable bilateral tinnitus — repeated MRI and extensive vestibular testing in a patient with symmetric audiometric tinnitus is rarely productive and reinforces the threat interpretation
- Do not use experimental devices without evidence — the tinnitus marketplace is full of expensive devices and supplements with little or no evidence base; direct patients to the AAO-HNS guideline and ATA recommendations for evidence-grounded options
Key Research Papers
- Jastreboff PJ (1990). Phantom auditory perception (tinnitus): mechanisms of generation and perception. Neuroscience Research. — Search PubMed
- Jastreboff PJ, Hazell JW (1993). A neurophysiological approach to tinnitus: clinical implications. British Journal of Audiology. — Search PubMed
- Tunkel DE et al. (2014). Clinical practice guideline: tinnitus. Otolaryngol Head Neck Surg. — PubMed 25273878
- Fuller T et al. (2020). Cognitive behavioural therapy for tinnitus. Cochrane Database. — Search PubMed
- Sereda M et al. (2018). Sound therapy (using amplification devices and/or sound generators) for tinnitus. Cochrane Database. — PubMed 30589445
- Hobson J et al. (2012). Sound therapy (masking) in the management of tinnitus in adults. Cochrane Database. — Search PubMed
- Okamoto H et al. (2010). Listening to tailor-made notched music reduces tinnitus loudness and tinnitus-related auditory cortex activity. PNAS. — Search PubMed
- Conlon B et al. (2020). Bimodal neuromodulation combining sound and tongue stimulation reduces tinnitus symptoms. Science Translational Medicine. — PubMed 33028707
- Hoare DJ et al. (2014). Sound therapy for tinnitus management: practicable options. J Am Acad Audiol. — PubMed 24622858
- Searchfield GD et al. (2017). Sound therapy options for tinnitus. Frontiers in Aging Neuroscience. — Search PubMed
- Hesser H et al. (2011). A systematic review and meta-analysis of randomized controlled trials of CBT for tinnitus distress. Clinical Psychology Review. — Search PubMed
- Henry JA et al. (2005). Comparison of tinnitus masking and tinnitus retraining therapy. J Am Acad Audiol. — Search PubMed
PubMed Topic Searches
- PubMed: Tinnitus Retraining Therapy / Jastreboff
- PubMed: Hearing aids for tinnitus
- PubMed: CBT for tinnitus
- PubMed: Notched-music therapy
- PubMed: Bimodal neuromodulation / Lenire
Connections
- Tinnitus Hub
- Benefits Deep-Dive Hub
- Causes and Triggers
- Nutrient Status (B12, Mg, Zn)
- NAC and Antioxidants
- Ginkgo Biloba for Tinnitus
- Glycine for Tinnitus
- Taurine for Tinnitus
- Neurology
- Anxiety
- Depression
- Insomnia
- Meditation
- All Remedies
- Ginkgo Biloba
- Tinnitus — the ENT clinical overview, including the hearing loss and audiometry findings that decide whether hearing aids or masking come first.