Tinnitus Causes and Triggers
Tinnitus has no single cause — it is a final-common-pathway symptom of dozens of distinct upstream insults, ranging from peripheral cochlear hair-cell damage to central auditory-cortex maladaptive plasticity to vascular, muscular, and joint pathology in the head and neck. Identifying which upstream cause is dominant in any individual patient determines which interventions will be effective. This page walks through the major mechanistic categories with prevalence figures, the validated trigger inventory that fluctuates symptom severity, and the practical assessment that distinguishes treatable peripheral causes from intractable central tinnitus.
Table of Contents
- Two Categories: Subjective vs Objective Tinnitus
- Noise-Induced Hearing Loss — The Largest Cause
- Presbycusis (Age-Related Hearing Loss)
- Ototoxic Medications
- Otologic Conditions (Meniere's, Otosclerosis, Schwannoma)
- Somatic Tinnitus (TMJ, Cervical Spine, Whiplash)
- Pulsatile and Vascular Tinnitus
- Central Auditory Plasticity — The Phantom-Limb Analogy
- The Modifiable Trigger Inventory
- Practical Assessment for the New Tinnitus Patient
- Key Research Papers
- Connections
- Featured Videos
Two Categories: Subjective vs Objective Tinnitus
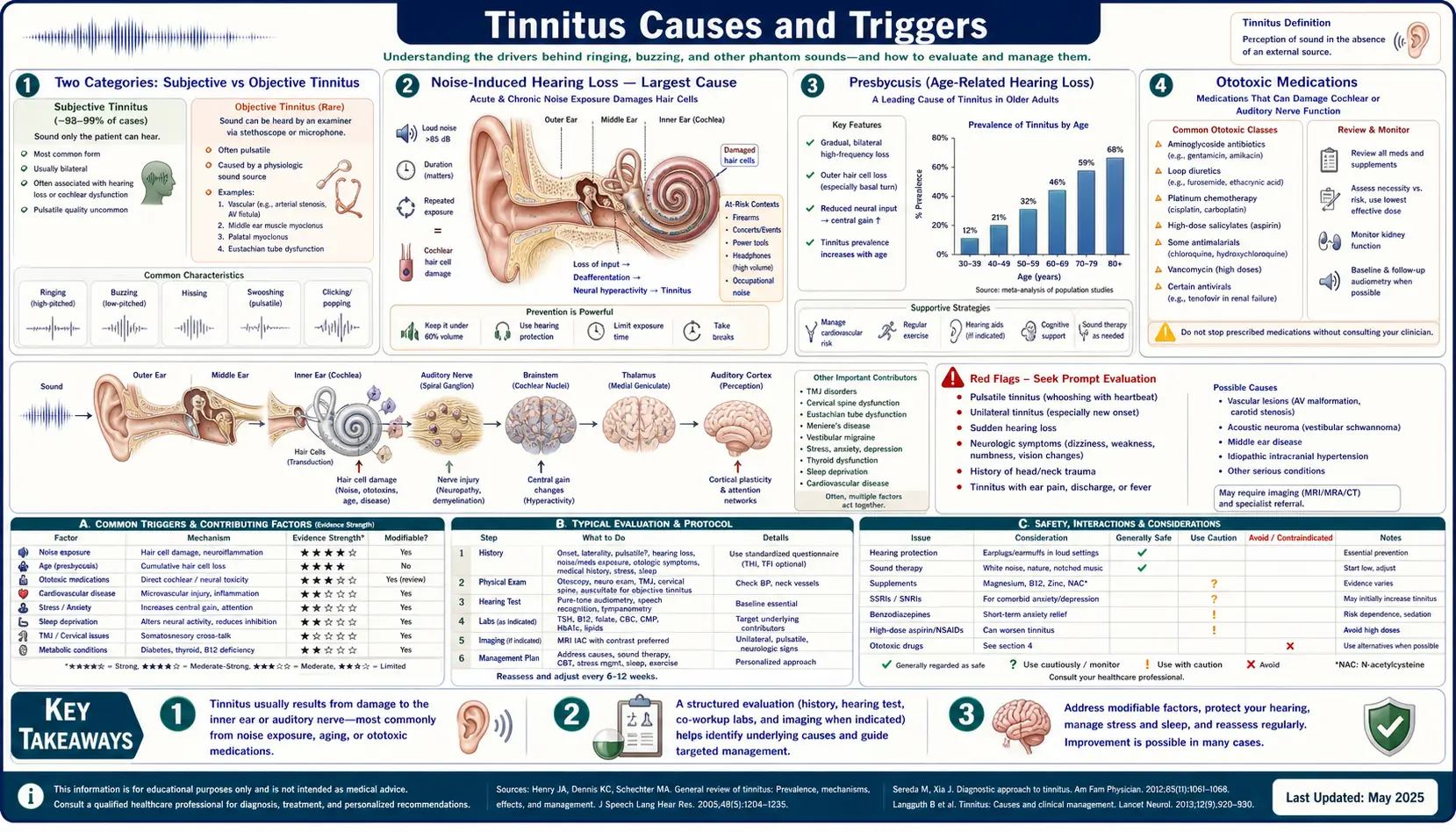
The first clinical distinction is between subjective tinnitus (heard only by the patient, generated by neural activity without external sound) and objective tinnitus (a real acoustic phenomenon that can sometimes be heard by an examining clinician with a stethoscope placed over the ear). Subjective tinnitus accounts for greater than 99% of cases. Objective tinnitus, while rare, is more often treatable because it has a definable acoustic generator — vascular turbulence, palatal myoclonus, stapedial muscle spasm, eustachian tube dysfunction — that can sometimes be eliminated.
The clinical question on first encounter is therefore: does the patient's tinnitus have any character suggesting an objective generator? Pulsatile tinnitus that tracks the heartbeat strongly suggests a vascular cause (worth pursuing imaging). Tinnitus with a clicking or thumping quality that the examiner can detect suggests palatal myoclonus or stapedial myoclonus. Pure tonal or high-frequency hissing tinnitus is almost always subjective and the workup focuses on identifying the peripheral cochlear or central cause.
Noise-Induced Hearing Loss — The Largest Cause
Acoustic overexposure is by far the most common identifiable cause of subjective tinnitus, accounting for an estimated 40–50% of cases in adult civilian populations and a substantially higher fraction in military veterans (tinnitus is the most common service-connected disability in the US Department of Veterans Affairs system).
The mechanism is mechanical and biochemical injury to the outer hair cells of the cochlea, the most vulnerable structures in the inner ear. Acoustic overexposure produces a sudden glutamate excitotoxic surge at the inner-hair-cell synapse, mitochondrial calcium overload, reactive oxygen species generation, and ultimately apoptotic and necrotic death of outer hair cells — particularly in the basal (high-frequency) region of the cochlea. The classic noise notch on audiometry at 4 kHz reflects this anatomic pattern.
The relationship between noise exposure and tinnitus is not linear. A single severe acoustic event (a gunshot, an explosion, a rock concert) can produce immediate and permanent tinnitus. Repetitive moderate exposure (workplace noise, regular concert attendance, prolonged use of in-ear headphones at high volume) produces cumulative damage that emerges as tinnitus and hearing loss after years of exposure. The "temporary threshold shift" that follows acute exposure — the ringing and muffled hearing that resolves over hours to days after a loud event — was historically considered harmless but is now understood to produce cochlear synaptopathy (hidden hearing loss) even when audiogram thresholds return to normal.
Presbycusis (Age-Related Hearing Loss)
Presbycusis is the gradual high-frequency sensorineural hearing loss that occurs with aging, driven by progressive loss of outer hair cells, stria vascularis atrophy, and degeneration of spiral ganglion neurons. It is the second-most-common identifiable cause of tinnitus and dominates the etiology in patients over 60.
The pattern of hearing loss in presbycusis — gradual rolloff above 2–4 kHz — matches the frequency at which most patients perceive their tinnitus. This is not coincidence. The Schaette and McAlpine "central gain" model proposes that the central auditory cortex compensates for reduced afferent input from a damaged cochlea by turning up its own gain, much like a hearing aid amplifying a weak signal. The upregulated central gain amplifies spontaneous neural activity into a perceived tone — the phantom signal of tinnitus — centered at the frequencies where peripheral input is most attenuated.
The clinical implication is that audiometry should be performed in every adult patient presenting with new tinnitus. The frequencies of the patient's tinnitus typically correspond to the frequencies of their hearing loss, and amplification with appropriately fit hearing aids reduces the central gain and often the perceived tinnitus loudness as a side effect of the primary hearing-loss treatment. See the sound therapy page for the role of hearing aids in tinnitus management.
Ototoxic Medications
Several drug classes are well-documented to cause tinnitus and hearing loss through direct cochlear toxicity. The major offenders:
- Salicylates (aspirin) — at high doses (greater than 4 g/day), aspirin produces dose-dependent reversible tinnitus through cochlear COX inhibition and outer-hair-cell electromotility changes. Tinnitus resolves within 24–72 hours of dose reduction. The threshold dose for symptoms varies considerably; some patients develop tinnitus on standard analgesic doses.
- Aminoglycoside antibiotics — gentamicin, tobramycin, amikacin, neomycin, and streptomycin produce ototoxicity through cochlear and vestibular hair-cell death, often permanent. Risk is greatest with prolonged IV therapy, renal impairment, and pre-existing hearing loss. Genetic susceptibility (mitochondrial A1555G mutation) produces severe permanent hearing loss after a single dose in affected individuals.
- Loop diuretics — furosemide, bumetanide, and ethacrynic acid cause usually-reversible tinnitus through disruption of the stria vascularis sodium-potassium ATPase, particularly at high IV doses and in patients with renal insufficiency.
- Platinum-based chemotherapy — cisplatin produces dose-dependent, often permanent, ototoxicity and tinnitus through outer-hair-cell ROS injury. Carboplatin is somewhat less ototoxic at standard doses. This is the setting in which N-acetylcysteine and other antioxidants are most actively investigated as otoprotectants (see the NAC deep-dive).
- Quinine and chloroquine — quinine produces dose-dependent reversible tinnitus (the syndrome called "cinchonism"). The antimalarial chloroquine is similar.
- NSAIDs — ibuprofen, naproxen, and indomethacin can produce tinnitus through a salicylate-like mechanism, generally reversible.
A medication review is essential at the first tinnitus visit. Discontinuation of an ototoxic medication when possible — or substitution to a non-ototoxic alternative — can resolve drug-induced tinnitus entirely.
Otologic Conditions (Meniere's, Otosclerosis, Schwannoma)
Several specific otologic diseases produce tinnitus as a primary feature:
- Meniere's disease — an idiopathic disorder of endolymphatic hydrops producing the classic triad of fluctuating low-frequency hearing loss, episodic vertigo, and roaring or low-pitched tinnitus. The tinnitus quality is characteristic and distinguishes Meniere's from most other causes. Sodium restriction, diuretics, and intratympanic steroid or gentamicin injection are standard management.
- Otosclerosis — abnormal bony remodeling fixing the stapes footplate, producing conductive hearing loss and often tinnitus, frequently in younger adults (peak onset 20–40). Stapedectomy surgery resolves the conductive loss and often the tinnitus.
- Vestibular schwannoma (acoustic neuroma) — a benign tumor of Schwann cells on the vestibular branch of cranial nerve VIII, presenting with unilateral hearing loss, tinnitus, and sometimes vertigo. The crucial clinical pearl is that any unilateral tinnitus deserves MRI imaging to rule out schwannoma. Most are slow-growing and managed with observation, but a missed schwannoma growing into the cerebellopontine angle can be catastrophic.
- Eustachian tube dysfunction — chronic middle-ear pressure dysregulation produces a sensation of fullness and often low-pitched fluctuating tinnitus. Nasal steroid sprays, Valsalva maneuvers, and (in selected cases) balloon dilation of the eustachian tube address the underlying pathology.
- Cerumen impaction — the simplest and most embarrassingly missed cause. Removing impacted wax can resolve tinnitus in a small but real fraction of cases. Otoscopic examination should occur at every new tinnitus visit.
Somatic Tinnitus (TMJ, Cervical Spine, Whiplash)
Somatic tinnitus is a distinct subtype in which the phantom percept is modulated by movement or pressure of the head, neck, or jaw. The underlying mechanism is convergence of somatosensory input from the trigeminal nerve and upper-cervical dorsal-root ganglia onto the dorsal cochlear nucleus — the first central relay of the auditory pathway. Aberrant somatosensory signaling from TMJ dysfunction or cervical-spine pathology biases dorsal-cochlear-nucleus activity and generates a phantom auditory signal.
Clinical features that suggest somatic tinnitus:
- Tinnitus modulated by jaw clenching, chewing, or neck rotation
- Co-existing TMJ pain, clicking, or limited mouth opening
- Co-existing cervical pain or limited neck range of motion
- History of whiplash, cervical-spine surgery, or chronic posture-related neck strain
- Normal or near-normal audiogram
Treatment of the underlying somatic dysfunction — physical therapy for cervical spine and posture, dental management of TMJ dysfunction, occlusal splints, trigger-point injections — can produce substantial tinnitus improvement in this subset. The Levine model (1999) of somatic tinnitus is the seminal description of the mechanism.
Pulsatile and Vascular Tinnitus
Pulsatile tinnitus — a rhythmic sound that tracks the heartbeat — is a distinct subtype that almost always has an identifiable vascular cause. Unlike most tinnitus, pulsatile tinnitus warrants prompt imaging workup because some causes are surgically correctable and a few are life-threatening.
The differential includes:
- Atherosclerotic carotid disease — turbulent flow through a stenotic carotid artery produces audible bruit transmitted to the inner ear
- Dural arteriovenous fistula — an abnormal connection between meningeal arteries and dural venous sinuses, producing turbulent flow audible to the patient. Endovascular treatment is curative.
- Glomus tumor (paraganglioma) — a vascular tumor of the middle ear or jugular bulb producing pulsatile tinnitus, conductive hearing loss, and a characteristic reddish mass behind the tympanic membrane
- Sigmoid sinus diverticulum or dehiscence — an anatomic variant producing turbulent venous flow audible in the adjacent inner ear, often correctable surgically
- Idiopathic intracranial hypertension — elevated CSF pressure produces venous turbulence and pulsatile tinnitus, especially in young overweight women; treatable with weight loss and acetazolamide
- Severe anemia or hyperthyroidism — high-output states with increased cardiac output produce audible vascular flow even in the absence of structural pathology
The standard workup for pulsatile tinnitus is MR angiography of the head and neck, with CT venography if a venous cause is suspected. Carotid duplex ultrasound screens for atherosclerotic stenosis. Audiometry, complete blood count, and TSH should also be obtained.
Central Auditory Plasticity — The Phantom-Limb Analogy
The most important conceptual advance in tinnitus neuroscience in the last 30 years is the recognition that chronic tinnitus is not generated in the ear but in the brain. The Jastreboff neurophysiologic model (1990) and the Eggermont central-gain model (2004) frame tinnitus as a phantom percept analogous to phantom-limb pain in amputees — the central nervous system continues to perceive a signal in the absence of the peripheral generator that originally produced it.
The neuroplastic mechanism: when cochlear hair cells in a specific frequency region are lost (from noise, aging, or ototoxin), the central auditory cortex receives less afferent input from those frequencies. Through Hebbian plasticity, neurons in the deafferented region of cortex expand their receptive fields to encompass adjacent frequencies and increase their spontaneous firing rate. This spontaneous activity, in the absence of acoustic input, is interpreted by higher cortical areas as a real sound — the phantom tone of tinnitus.
This central-plasticity model explains several otherwise puzzling clinical observations:
- Why surgical destruction of the cochlea (rare cochleotomy procedures) does not abolish tinnitus — the phantom signal is now generated centrally, not peripherally
- Why the perceived pitch of tinnitus matches the frequency of the audiometric hearing loss — the deafferented cortical region is what generates the phantom signal
- Why amplification (hearing aids) reduces tinnitus — restoring afferent input to the deafferented cortical region reduces the maladaptive plasticity
- Why sound therapy and notched-music therapy can reduce tinnitus — targeted acoustic input to the affected frequencies reverses the cortical reorganization
- Why severe stress, sleep deprivation, and limbic activation worsen tinnitus — the prefrontal-limbic filtering circuit that normally suppresses irrelevant background signals is impaired by these states
The Modifiable Trigger Inventory
Once tinnitus is established, its perceived loudness and intrusiveness fluctuate considerably in response to identifiable triggers. Patients should be guided through a systematic trigger inventory and a one-month elimination trial of each suspected trigger to identify which apply to them:
- Caffeine — coffee, tea, energy drinks, and caffeinated soda; aim for elimination for 30 days then reintroduction to test
- Sodium — particularly relevant in Meniere's-type tinnitus; target less than 2 g sodium/day
- Alcohol — especially red wine and beer; often produces acute worsening within hours of consumption
- Nicotine — cigarettes, e-cigarettes, and nicotine pouches; vasoconstriction reduces cochlear blood flow
- Sleep deprivation — the single most consistent modulator; less than 7 hours sleep predictably worsens next-day tinnitus
- Stress — through limbic activation and impaired prefrontal filtering; relaxation training, meditation, and CBT directly address this
- Loud-noise exposure — even brief exposure to concerts, power tools, or fireworks can trigger weeks of increased tinnitus; hearing protection is essential
- Aspartame and MSG — reported by some patients though formal trial evidence is limited; worth an elimination trial in stubborn cases
- Specific medications — see the ototoxic medications section above; even non-ototoxic drugs sometimes worsen tinnitus idiosyncratically
- Dehydration — aim for at least 2 L water/day; dehydration concentrates blood and may alter cochlear microcirculation
Practical Assessment for the New Tinnitus Patient
A reasonable first-visit workup for a new tinnitus patient should include:
- History — onset, duration, laterality, character (tonal, hissing, pulsatile, clicking), modulating factors (jaw, neck movement, head position), associated symptoms (hearing loss, vertigo, otalgia, fullness), occupational and recreational noise exposure, complete medication list, family history of hearing loss
- Otoscopic examination — rule out cerumen impaction, tympanic-membrane perforation, middle-ear effusion, visible mass
- Audiometry — pure-tone air and bone conduction, speech audiometry, tympanometry; ideally extending to 8 kHz
- Tinnitus matching — pitch and loudness matching using audiometric tones, validated questionnaires (Tinnitus Handicap Inventory, Tinnitus Functional Index) to quantify distress baseline
- Laboratory studies — serum B12, ferritin, magnesium, zinc, TSH, basic metabolic panel, complete blood count; see the nutrient-status deep-dive
- MRI imaging — mandatory for any unilateral tinnitus (rule out vestibular schwannoma), and for pulsatile tinnitus (MR angiography); not routinely needed for symmetric bilateral subjective tinnitus with explanatory hearing loss
- TMJ and cervical examination — particularly if tinnitus modulates with jaw or neck movement
- Specialty referral — otolaryngology for any structural finding; neurology for pulsatile or refractory cases; psychology for prominent distress component
Key Research Papers
- Jastreboff PJ (1990). Phantom auditory perception (tinnitus): mechanisms of generation and perception. Neuroscience Research. — Search PubMed
- Bauer CA (2018). Tinnitus. NEJM 378(13):1224-1231. — Search PubMed
- Schaette R, McAlpine D (2011). Tinnitus with a normal audiogram: physiological evidence for hidden hearing loss. Journal of Neuroscience. — Search PubMed
- Levine RA (1999). Somatic (craniocervical) tinnitus and the dorsal cochlear nucleus hypothesis. American Journal of Otolaryngology. — PubMed 10609479
- Tunkel DE et al. (2014). Clinical practice guideline: tinnitus. Otolaryngol Head Neck Surg. — PubMed 25273878
- Langguth B et al. (2013). Tinnitus: causes and clinical management. Lancet Neurology. — Search PubMed
- Baguley D, McFerran D, Hall D (2013). Tinnitus. Lancet. — Search PubMed
- Henry JA et al. (2005). General review of tinnitus. J Speech Lang Hear Res. — PubMed 16411806
- Bhatt JM et al. (2016). Prevalence, severity, exposures, and treatment patterns of tinnitus in the US. JAMA Otolaryngol. — PubMed 27441392
- Eggermont JJ, Roberts LE (2004). The neuroscience of tinnitus. Trends in Neurosciences. — Search PubMed
- Bisht M, Bist SS (2011). Ototoxicity: the hidden menace. Indian J Otolaryngol. — Search PubMed
- Reavis KM et al. (2017). Noise-induced hearing loss in the military. Hearing Research. — Search PubMed
PubMed Topic Searches
- PubMed: Tinnitus causes and etiology
- PubMed: Noise-induced hearing loss and tinnitus
- PubMed: Ototoxic medications and tinnitus
- PubMed: Pulsatile tinnitus workup
- PubMed: Somatic tinnitus, TMJ, cervical
Connections
- Tinnitus Hub
- Benefits Deep-Dive Hub
- Nutrient Status (B12, Mg, Zn)
- Sound Therapy and Habituation
- NAC and Antioxidants
- Ginkgo Biloba for Tinnitus
- Glycine for Tinnitus
- Taurine for Tinnitus
- Neurology
- Vitamin B12
- Magnesium
- Zinc
- N-Acetyl-Cysteine
- Ginkgo Biloba
- Tinnitus — the ENT clinical overview: diagnosis, audiometric workup, and the full differential behind these causes.
- All Remedies