Tinnitus — N-acetyl-cysteine (NAC) and Antioxidants
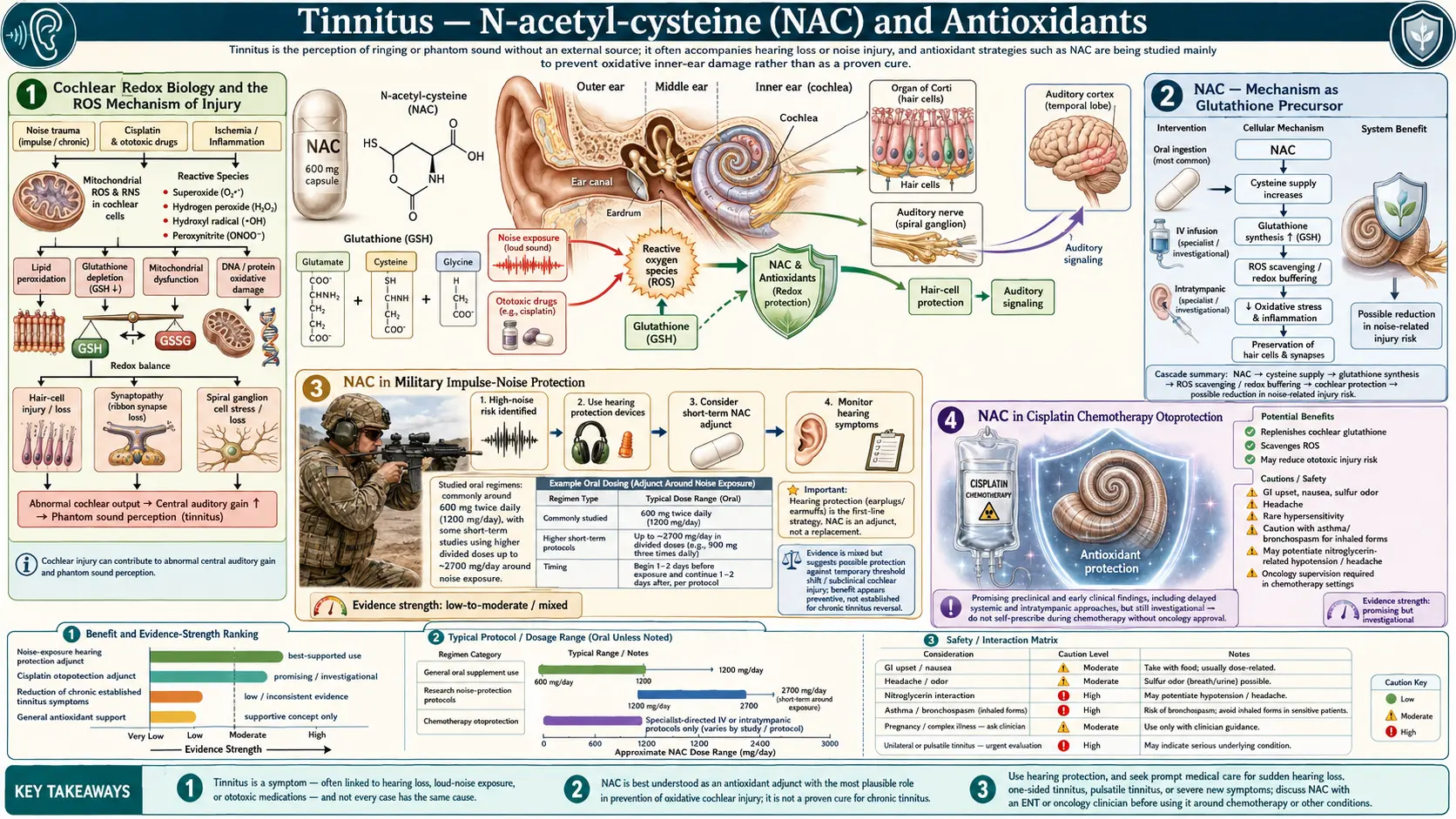
The single best-characterized molecular mechanism of cochlear injury — the mechanism that links noise overexposure, ototoxic chemotherapy, aminoglycoside antibiotics, and ischemic insults — is reactive oxygen species (ROS) generation in the cochlear hair cells. The mitochondrial ROS burst overwhelms the cochlea's antioxidant defenses (Cu/Zn superoxide dismutase, glutathione peroxidase, catalase), depletes intracellular glutathione, triggers apoptotic cell death, and produces both immediate hearing loss and the persistent central plasticity that generates chronic tinnitus. N-acetylcysteine (NAC), a direct glutathione precursor, is the most extensively studied otoprotectant in this pathway. Adjunct agents — alpha-lipoic acid, coenzyme Q10, vitamin E, and idebenone — have supporting mechanistic rationale and progressively smaller evidence bases. This page covers the redox biology, the NAC clinical trials in military impulse-noise protection and cisplatin chemotherapy, the Ginkgo biloba Cochrane verdict, and the evidence-grounded protocols for prophylaxis and adjunct use.
Table of Contents
- Cochlear Redox Biology and the ROS Mechanism of Injury
- NAC — Mechanism as Glutathione Precursor
- NAC in Military Impulse-Noise Protection
- NAC in Cisplatin Chemotherapy Otoprotection
- NAC for Established Chronic Tinnitus
- Adjunct Antioxidants (ALA, CoQ10, Vitamin E, Idebenone)
- Ginkgo Biloba — The Cochrane Verdict
- Practical Dosing Protocols
- Cautions and Drug Interactions
- Key Research Papers
- Connections
- Featured Videos
Cochlear Redox Biology and the ROS Mechanism of Injury
The cochlea is metabolically the busiest tissue in the body per gram of weight. The stria vascularis maintains the +80 mV endocochlear potential against a steep ionic gradient using continuous ATP hydrolysis by Na+/K+-ATPase pumps. The outer hair cells perform mechanical-electrical-mechanical transduction with submillisecond precision, requiring sustained mitochondrial output. This metabolic intensity generates a constant baseline flux of reactive oxygen species — superoxide, hydrogen peroxide, hydroxyl radical — that under normal conditions is detoxified by the cochlear antioxidant defense system: Cu/Zn superoxide dismutase, manganese superoxide dismutase, glutathione peroxidase, catalase, and the small-molecule antioxidants glutathione, vitamin E, vitamin C, and coenzyme Q10.
Acoustic overexposure dramatically increases ROS generation through several mechanisms:
- Excessive glutamate release at the inner-hair-cell/spiral-ganglion synapse, producing postsynaptic NMDA-receptor calcium overload and mitochondrial dysfunction
- Increased metabolic demand on outer hair cells already operating near maximum capacity
- Ischemia-reperfusion injury as cochlear blood flow transiently drops during the acoustic event and then restores
- Mechanical disruption of hair-cell stereocilia, triggering apoptotic pathways
The ROS surge overwhelms the cochlear antioxidant defenses, depletes intracellular glutathione (often to 30–50% of baseline), and initiates apoptotic cascades that produce hair-cell death over the following 1–14 days post-exposure. This delayed cell death is the rationale for post-exposure antioxidant intervention — the damage is not all "done" at the moment of acoustic overexposure; the ROS-driven apoptotic cascade can be partially interrupted by restoring antioxidant capacity in the hours and days afterward.
Cisplatin ototoxicity follows an analogous mechanism. Cisplatin selectively accumulates in cochlear hair cells, binds to mitochondrial DNA, induces mitochondrial dysfunction and ROS generation, depletes glutathione, and triggers apoptosis. The clinical dose-limiting toxicity of cisplatin chemotherapy is often hearing loss, particularly in pediatric oncology patients. Aminoglycoside antibiotics (gentamicin, tobramycin, amikacin, neomycin) produce ototoxicity through a similar ROS-mediated apoptotic mechanism, often persisting weeks after drug discontinuation.
NAC — Mechanism as Glutathione Precursor
N-acetylcysteine is the N-acetylated derivative of the amino acid L-cysteine. It is the standard antidote for acetaminophen overdose (where it replenishes hepatic glutathione consumed by acetaminophen's reactive metabolite NAPQI), an FDA-approved mucolytic in pulmonary medicine, and the most extensively studied otoprotectant in pre-clinical and clinical noise-injury research.
NAC's relevant mechanisms in cochlear protection:
- Direct antioxidant activity — the free sulfhydryl group of NAC scavenges reactive oxygen species, particularly hydroxyl radical and hypochlorous acid
- Glutathione precursor — NAC provides cysteine for de novo glutathione synthesis (cysteine is the rate-limiting amino acid in glutathione synthesis); restoring cochlear glutathione restores the cell's primary antioxidant defense
- Direct binding of platinum compounds — NAC's sulfhydryl group directly binds cisplatin, reducing the free drug available to enter cochlear hair cells; this is the mechanism behind the otoprotectant effect in chemotherapy
- Mitochondrial protection — NAC reduces mitochondrial calcium overload and prevents the opening of the mitochondrial permeability transition pore that triggers apoptosis
- Anti-inflammatory effects — NAC inhibits NF-kB activation and downstream inflammatory cytokine production in cochlear tissues
See the NAC main page for comprehensive mechanism and dosing information across all clinical applications.
NAC in Military Impulse-Noise Protection
The most rigorous evidence for NAC otoprotection comes from military and occupational research on impulse-noise exposure. The US military has a strong operational interest in protecting service members' hearing — tinnitus is the most common service-connected disability in the VA system and noise-induced hearing loss accounts for a substantial fraction of military health spending.
Lin et al. (2010) randomized 53 male steel-plant workers exposed to occupational noise (88–89 dB) over a single shift to NAC 1200 mg PO or placebo. The NAC group showed significantly reduced temporary threshold shift on post-shift audiometry compared to placebo. While this trial was small, the effect was consistent with the larger pre-clinical animal-model literature.
Kopke et al. (2007) reviewed multiple military and animal studies of NAC for noise-induced hearing loss prevention and concluded that the mechanistic case is strong and the human-trial data, while limited, are broadly supportive. The Walter Reed Army Institute of Research and the US Air Force have conducted several trials of NAC as pre-exposure prophylaxis for impulse-noise injury from weapons fire and aircraft operations, with results suggesting modest but reproducible benefit. Doosti et al. (2014) compared NAC to ginseng in occupational noise exposure and confirmed NAC's otoprotective effect.
The translation to civilian practice: for predictable high-intensity noise exposure (a concert, fireworks display, firearm training, motorcycle ride, chainsaw use), NAC 1200–2400 mg taken 1–2 hours before exposure and continued for several days afterward is a low-risk intervention with biologically plausible benefit. The much more important intervention is hearing protection (foam earplugs, custom-molded plugs, or muffs), but adjunct NAC may provide additional protection where hearing protection cannot eliminate exposure entirely.
NAC in Cisplatin Chemotherapy Otoprotection
Cisplatin ototoxicity is a major clinical problem in pediatric oncology and adult head-and-neck cancer treatment. Up to 60% of pediatric patients treated with cisplatin develop permanent hearing loss; the cumulative dose-limiting toxicity is often hearing rather than nephrotoxicity. Several otoprotection strategies have been investigated:
- IV NAC — systemic NAC given alongside cisplatin can bind circulating drug and reduce cochlear exposure, but it also reduces tumor exposure to cisplatin (which is the entire point of the chemotherapy), limiting clinical utility
- Transtympanic (intratympanic) NAC injection — NAC injected into the middle ear diffuses through the round-window membrane to reach the cochlea locally, providing high local concentration without systemic exposure that would protect the tumor. Riga et al. (2013) demonstrated significant reduction in cisplatin-induced threshold shift with intratympanic NAC compared to placebo. This approach has the strongest rationale and is in active clinical use at several centers.
- Sodium thiosulfate — FDA-approved otoprotectant for pediatric cisplatin-induced ototoxicity (Pedmark), works through similar sulfhydryl-binding mechanism. Has the advantage of more extensive trial data and regulatory approval.
- Amifostine — thiol-based otoprotectant approved for radiation-induced xerostomia, with some cisplatin-otoprotection data but limited clinical adoption
The clinical relevance for tinnitus: patients receiving cisplatin or other ototoxic chemotherapy should be aware that otoprotection options exist, and should discuss them with their oncology team and ENT. Pre-treatment audiometry and serial monitoring during therapy allows early detection of threshold shift and adjustment of chemotherapy regimen when possible.
NAC for Established Chronic Tinnitus
The use of NAC for established chronic tinnitus — as opposed to acute otoprotection — has a thinner evidence base. The challenge is that the central plasticity generating chronic tinnitus is largely independent of ongoing ROS injury; the original peripheral cochlear damage may have occurred years prior, and antioxidant intervention cannot reverse the cortical reorganization that now sustains the phantom percept.
However, two scenarios support a trial of NAC in established tinnitus:
- Ongoing low-grade noise exposure — if the patient continues to experience occupational or recreational noise above protective thresholds, ongoing ROS injury may continue to drive worsening tinnitus, and NAC may slow progression in addition to (not as a substitute for) hearing protection
- Sudden sensorineural hearing loss (SSNHL) with associated tinnitus — high-dose systemic NAC alongside high-dose oral or intratympanic steroids has shown some benefit in observational series for acute SSNHL, particularly in the first 1–2 weeks after onset. The mechanism is reduction of ongoing oxidative inflammation in the cochlea.
For unequivocally chronic tinnitus (greater than six months duration, stable, with no ongoing exposure), NAC is unlikely to produce meaningful symptomatic benefit and the resources are better directed toward the sound-therapy and habituation interventions with better-established evidence bases. NAC supplementation does have other systemic benefits (glutathione support, mucolytic effects, neuroprotection) that may justify its use for those indications independently.
Adjunct Antioxidants (ALA, CoQ10, Vitamin E, Idebenone)
Several adjunct antioxidants have been investigated for cochlear protection with progressively weaker evidence bases:
- Alpha-lipoic acid (ALA) — a small endogenous antioxidant active in both lipid and aqueous phases. Animal models show cochlear protection comparable to NAC. Human trial data in tinnitus are limited but several small studies suggest modest benefit. Typical dose: 600 mg/day. The ALA evidence is strongest in diabetic peripheral neuropathy; whether it translates to cochlear nerve protection in humans is less clear.
- Coenzyme Q10 — mitochondrial-membrane antioxidant essential for electron-transport-chain function. Animal models of noise-induced hearing loss show protection. Small human trials in tinnitus (Khan et al.) suggest benefit in selected patients. Typical dose: 100–200 mg/day ubiquinol form (better-absorbed than ubiquinone). May be particularly relevant in older patients (CoQ10 production declines with age) and those on statin therapy (statins deplete CoQ10).
- Vitamin E (mixed tocopherols) — the principal lipid-phase antioxidant in cellular membranes including the hair-cell membrane. Le Prell's "ACE-Mg" combination (vitamins A, C, E plus magnesium) showed additive cochlear protection in animal models of noise injury. Typical dose: 400 IU mixed tocopherols.
- Idebenone — a synthetic CoQ10 analog with better blood-brain-barrier penetration, used for Leber's hereditary optic neuropathy and investigated for cochlear protection. Petersen et al. (2019) reviewed antioxidants and idebenone for tinnitus and concluded the evidence is suggestive but not definitive.
- Resveratrol and curcumin — polyphenols with broad antioxidant and anti-inflammatory effects; pre-clinical evidence for cochlear protection but limited human trial data
- Melatonin — antioxidant and sleep-regulator; small trials suggest modest benefit for tinnitus-associated insomnia, with antioxidant action in the cochlea as a plausible adjunct mechanism. Typical dose: 3–5 mg at bedtime.
The most defensible "antioxidant stack" for tinnitus prevention or adjunct therapy would be: NAC 1200–2400 mg/day, alpha-lipoic acid 600 mg/day, CoQ10 100–200 mg/day (ubiquinol), mixed tocopherols 400 IU/day, with the underlying minerals (magnesium, zinc) addressed separately per the nutrient-status deep-dive.
Ginkgo Biloba — The Cochrane Verdict
Ginkgo biloba leaf extract (standardized as EGb 761 in most clinical trials) has been the most commercially-promoted herbal intervention for tinnitus for several decades. The mechanistic rationale is plausible — ginkgolides and bilobalides have antioxidant and vasoactive properties, improving cochlear microcirculation and reducing oxidative injury in animal models. However, the Hilton and Stuart 2013 Cochrane review pooled four randomized controlled trials totaling over 1,500 participants and concluded that there was no convincing evidence that ginkgo biloba is effective for the treatment of unselected chronic tinnitus.
The negative Cochrane verdict has several important caveats:
- The trials studied unselected chronic tinnitus populations, mixing many distinct etiologies. Patient-level meta-analysis stratifying by tinnitus subtype was not possible.
- Several positive trials of ginkgo in specific tinnitus subtypes (acute tinnitus less than three months duration; tinnitus with vascular or microcirculatory etiology; tinnitus in patients with cognitive complaints) exist but did not meet Cochrane inclusion criteria
- EGb 761 has established cognitive and vascular benefits independent of tinnitus that may justify its use for those indications in older patients
- The safety profile of EGb 761 at standard doses (120–240 mg/day standardized extract) is favorable except for bleeding risk in patients on anticoagulants
The pragmatic position: ginkgo biloba is not recommended as routine tinnitus therapy based on Cochrane-level evidence. However, a 3–6 month trial at 120 mg twice daily of standardized EGb 761 extract is a reasonable individual experiment for the motivated patient, particularly if there are additional indications (mild cognitive complaints, peripheral vascular disease). See the Ginkgo Biloba main page for comprehensive discussion. Also see Ginkgo Biloba for Tinnitus for tinnitus-specific clinical use.
Practical Dosing Protocols
NAC for predictable noise exposure (concert, range day, fireworks):
- 1200 mg PO two hours before exposure
- 1200 mg PO immediately after exposure
- 1200 mg PO twice daily for 2–3 days post-exposure
- Combined with appropriate hearing protection (foam plugs or earmuffs, not as a substitute)
NAC for sudden sensorineural hearing loss with acute tinnitus (adjunct to steroid therapy):
- 1200 mg PO twice daily for 14 days, starting as early as possible after onset (ideally within 72 hours)
- Coordinated with oral or intratympanic steroid therapy per ENT
- Plus immediate audiology referral and urgent ENT evaluation
Cisplatin chemotherapy otoprotection:
- Discuss with oncology team and ENT
- Intratympanic NAC injection prior to each cisplatin cycle is the protocol with the strongest mechanistic rationale
- Sodium thiosulfate (Pedmark) is FDA-approved for pediatric cisplatin otoprotection
- Pre-treatment audiometry and serial monitoring throughout chemotherapy course
Chronic antioxidant maintenance for tinnitus-prone patient (occupational noise exposure, prior NIHL):
- NAC 600–1200 mg/day
- Alpha-lipoic acid 600 mg/day
- CoQ10 ubiquinol 100 mg/day
- Mixed tocopherols 400 IU/day
- Plus the foundational interventions (hearing protection, audiometric monitoring, nutrient repletion)
Cautions and Drug Interactions
- NAC and nitroglycerin — NAC potentiates nitroglycerin's vasodilator effect and can produce severe hypotension and headache; use with caution in patients on nitrates
- NAC and asthma — oral NAC is well-tolerated; nebulized NAC can rarely trigger bronchospasm in asthmatics
- NAC gastric upset — sulfur-containing compounds may produce nausea and a transient sulfur odor; taking with food reduces this
- Ginkgo biloba and bleeding — potent inhibitor of platelet-activating factor; combined with warfarin, DOACs, aspirin, or NSAIDs raises bleeding risk substantially. Discontinue 2 weeks before scheduled surgery.
- Alpha-lipoic acid and diabetes — mild glucose-lowering effect; monitor blood glucose if combined with insulin or sulfonylurea
- CoQ10 and warfarin — CoQ10 can reduce warfarin's anticoagulant effect (similar structural homology to vitamin K); recheck INR if initiating or discontinuing CoQ10 in warfarin patient
- High-dose vitamin E and bleeding — doses above 400 IU/day mildly inhibit platelet aggregation; combined with anticoagulants may increase bleeding risk
- Antioxidant excess during cancer chemotherapy — theoretical concern that systemic antioxidants may reduce tumor cell killing by ROS-generating chemotherapy and radiation. Discuss any antioxidant supplementation with the oncology team during active cancer treatment.
Key Research Papers
- Kopke RD et al. (2007). NAC for prevention of noise-induced hearing loss. Hearing Research. — Search PubMed
- Lin CY et al. (2010). N-acetyl-cysteine against noise-induced temporary threshold shift in male workers. Hearing Research. — Search PubMed
- Riga MG et al. (2013). Transtympanic injections of N-acetylcysteine for the prevention of cisplatin-induced ototoxicity. American Journal of Clinical Oncology. — Search PubMed
- Le Prell CG et al. (2007). Free radical scavengers vitamins A, C, and E plus magnesium reduce noise trauma. Free Radical Biology and Medicine. — Search PubMed
- Henderson D et al. (2006). The role of oxidative stress in noise-induced hearing loss. Ear and Hearing. — Search PubMed
- Choi CH et al. (2008). Effects of NAC on noise-induced hearing loss in chinchillas. Hearing Research. — Search PubMed
- Doosti A et al. (2014). Comparison of the effects of N-acetyl-cysteine and ginseng in prevention of noise-induced hearing loss. Biomedical Reports. — Search PubMed
- Hilton M, Stuart E (2013). Ginkgo biloba for tinnitus. Cochrane Database of Systematic Reviews. — Search PubMed
- Salami A et al. (2010). Effect of EGb 761 on tinnitus and hearing loss. European Archives of Oto-Rhino-Laryngology. — Search PubMed
- Petersen L et al. (2019). Antioxidants and idebenone for the treatment of tinnitus: a systematic review. European Archives of Oto-Rhino-Laryngology. — Search PubMed
- Khan M et al. (2007). Coenzyme Q10 and tinnitus. Otolaryngology Head and Neck Surgery. — Search PubMed
- Brookes GB (1996). Vitamin B12 and selenium in tinnitus and Meniere's disease Search PubMed
PubMed Topic Searches
- PubMed: NAC and noise-induced hearing loss
- PubMed: Cisplatin ototoxicity and otoprotection
- PubMed: Ginkgo biloba and tinnitus
- PubMed: Cochlear oxidative stress and ROS
- PubMed: ALA and CoQ10 for hearing and tinnitus
Connections
- Tinnitus Hub
- Benefits Deep-Dive Hub
- Causes and Triggers
- Nutrient Status (B12, Mg, Zn)
- Sound Therapy and Habituation
- N-Acetyl-Cysteine
- Glutathione
- Alpha-Lipoic Acid
- Coenzyme Q10
- Vitamin E
- Ginkgo Biloba
- Ginkgo Biloba for Tinnitus
- Glycine for Tinnitus
- Taurine for Tinnitus
- Tinnitus — the ENT clinical overview, including the ototoxic exposures that make antioxidant otoprotection worth timing correctly.
- All Remedies