HRV Training for Stress Management
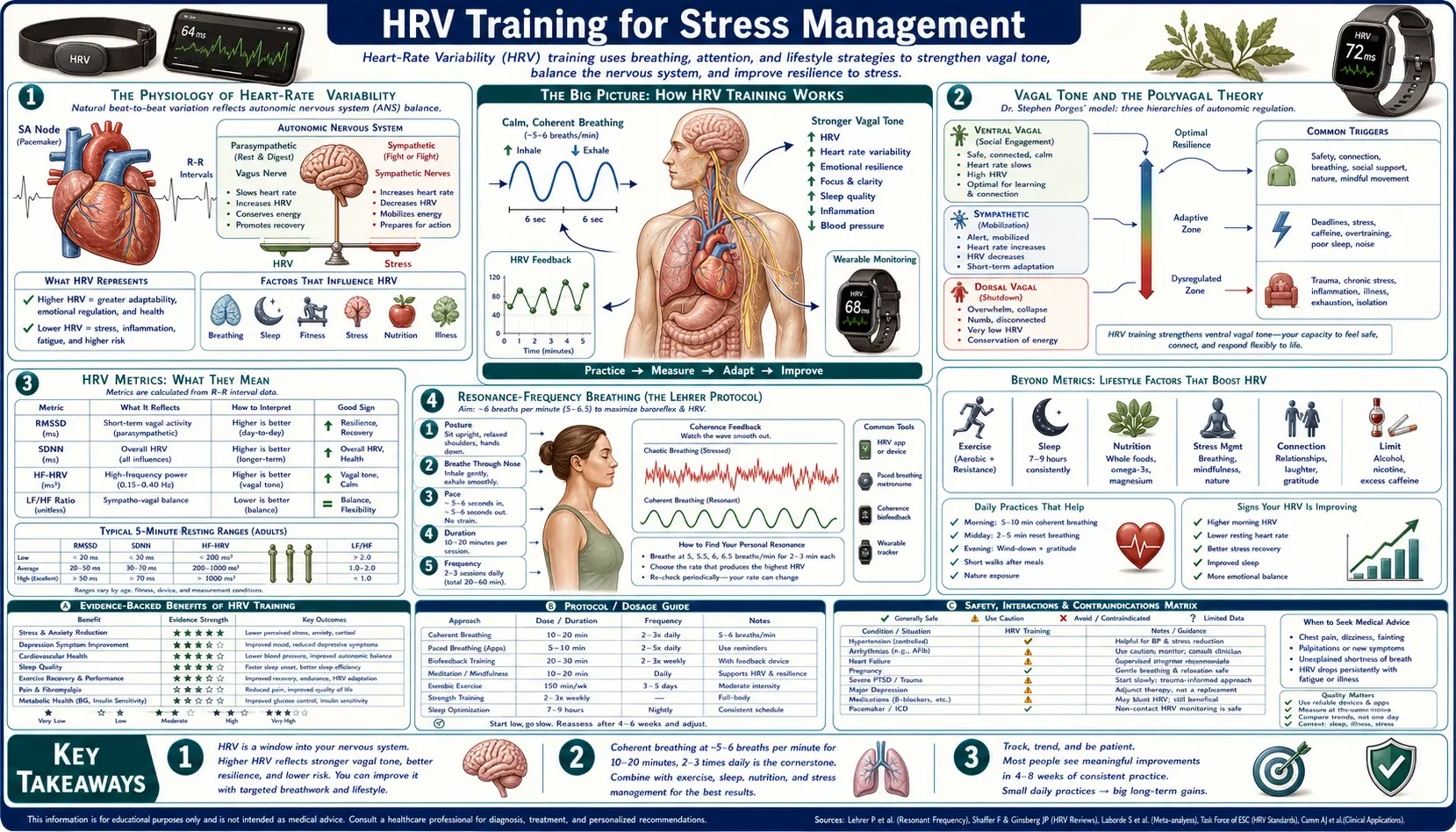
Heart-rate variability (HRV) is the natural beat-to-beat variation in the time between successive heartbeats — a precise non-invasive readout of vagal (parasympathetic) tone and autonomic balance. Higher HRV reflects greater parasympathetic engagement, better baroreflex sensitivity, and a more flexible cardiovascular system; lower HRV is independently predictive of cardiovascular mortality, depression, anxiety, and inflammation. Unlike most physiological markers, HRV is also a trainable parameter — deliberate practice of resonance-frequency breathing (typically around 5.5 breaths per minute, the rate at which the baroreflex feedback loop resonates with respiratory sinus arrhythmia) raises baseline HRV by 20-40% over 4-8 weeks of regular practice. The clinical translation has been one of the most robust findings in psychophysiology: HRV biofeedback shows moderate-to-large effect sizes for anxiety, depression, PTSD, hypertension, and athletic recovery. This deep dive covers the underlying physiology, the principal HRV metrics (RMSSD, SDNN, HF-HRV), the Lehrer-Vaschillo resonance-frequency protocol, wearable trackers, and practical training protocols.
Table of Contents
- The Physiology of Heart-Rate Variability
- Vagal Tone and the Polyvagal Theory
- HRV Metrics: RMSSD, SDNN, HF-HRV, LF/HF Ratio
- Resonance-Frequency Breathing (the Lehrer Protocol)
- Coherence Training (HeartMath)
- Wearable HRV Trackers
- Practical Training Protocol
- Clinical Evidence (Anxiety, PTSD, Hypertension)
- Cautions and What HRV Cannot Measure
- Key Research Papers
- Connections
- Featured Videos
The Physiology of Heart-Rate Variability
The heart does not beat at a constant rate. Even in a resting subject, the interval between successive R-waves on the ECG varies from beat to beat by tens or hundreds of milliseconds. The variability is not noise — it is highly structured information about the state of the autonomic nervous system that controls heart rate. Three principal sources contribute:
- Respiratory sinus arrhythmia (RSA) — heart rate accelerates during inspiration and slows during expiration. The acceleration is driven by transient vagal withdrawal during inspiration; the slowing is driven by vagal re-engagement during expiration. RSA produces the high-frequency (HF) band of HRV (0.15-0.4 Hz, corresponding to typical respiratory rates of 9-24 breaths/min). HF-HRV is the cleanest available non-invasive index of pure vagal tone.
- Baroreflex oscillations — the baroreflex loop — baroreceptors in the carotid sinus and aortic arch sensing blood pressure, signaling the brainstem, adjusting heart rate and vascular tone — has a natural resonance frequency around 0.1 Hz (one cycle every 10 seconds, or 6 breaths/min). When the subject breathes at this resonance frequency, the baroreflex enters resonance with respiration and HRV amplitude becomes dramatically larger. This phenomenon is the basis of HRV biofeedback.
- Thermoregulatory and humoral oscillations — very-low-frequency (VLF) oscillations (<0.04 Hz) reflect slower regulatory processes including thermoregulation, renin-angiotensin activity, and humoral factors. The functional significance of VLF is less well-characterized than HF or LF.
The net result is a heart-rate signal that, when transformed into the frequency domain, shows distinct peaks at the respiratory rate (HF, vagal), at the baroreflex resonance (LF, mixed), and at very low frequencies (VLF, slower regulatory). Each band carries different information.
Vagal Tone and the Polyvagal Theory
The vagus nerve (cranial nerve X) is the body's principal parasympathetic conduit, innervating the heart, lungs, gut, and most internal organs. Vagal output to the sinoatrial node of the heart is the dominant determinant of resting heart rate and the moment-to-moment variability around that rate. A high vagal tone produces a slow resting heart rate, a large RSA, and a high HF-HRV; a low vagal tone produces a faster resting heart rate, blunted RSA, and low HF-HRV.
Stephen Porges's polyvagal theory (2001 Int J Psychophysiol) reframes the vagus as two functionally distinct branches: an evolutionarily older unmyelinated dorsal vagal complex (DVC) associated with immobilization and freeze responses, and an evolutionarily newer myelinated ventral vagal complex (VVC) associated with social engagement, calm vigilance, and the modulation of cardiac output during ordinary social interaction. The VVC originates in the nucleus ambiguus, projects to the heart, larynx, pharynx, and facial muscles, and mediates the "social engagement system" of voice, gaze, and facial expression that humans use to signal safety to one another.
The clinical implication is that HRV reflects more than just cardiovascular regulation — it indexes social-engagement capacity, emotional regulation, and prefrontal-cortical inhibition of the limbic stress-response system. Thayer and colleagues (Ann N Y Acad Sci 2008) have extensively documented the relationship between HRV and prefrontal cortex function via what they call the "central autonomic network" — the medial prefrontal cortex, insula, amygdala, and brainstem nuclei that jointly regulate autonomic output.
HRV Metrics: RMSSD, SDNN, HF-HRV, LF/HF Ratio
HRV can be quantified in either the time domain (direct statistics on the inter-beat interval series) or the frequency domain (Fourier or autoregressive spectral analysis of the same series). The most widely used metrics are:
- RMSSD (root mean square of successive differences) — the square root of the mean of the squared differences between consecutive RR intervals. RMSSD is the time-domain measure that most directly reflects vagal (parasympathetic) activity and is highly correlated with HF-HRV. RMSSD is the metric most wearables (Oura, Whoop, Polar) report as their primary HRV value. Typical resting RMSSD ranges: 20-80 ms in healthy adults, lower in elderly and in clinical populations, higher in trained athletes (often >100 ms).
- SDNN (standard deviation of NN intervals) — the standard deviation of all valid RR intervals in the recording. SDNN reflects total HRV from all sources and is therefore higher than RMSSD. SDNN is the most validated long-term cardiovascular risk marker; a 24-hour SDNN <50 ms is associated with markedly elevated all-cause mortality in cardiac patients.
- HF-HRV (high-frequency power, 0.15-0.4 Hz) — the spectral power in the band corresponding to respiratory sinus arrhythmia. Almost purely vagal. Typically reported in absolute units (ms²) or normalized units (HF nu = HF / (HF + LF) × 100).
- LF-HRV (low-frequency power, 0.04-0.15 Hz) — spectral power in the band corresponding to baroreflex oscillations. Mixed sympathetic and parasympathetic contribution; commonly but contentiously interpreted as a sympathetic marker.
- LF/HF ratio — historically interpreted as a sympathovagal balance index. Modern HRV scholarship has largely rejected this interpretation as oversimplified; LF/HF should be interpreted with caution and is increasingly de-emphasized.
- pNN50 — percentage of successive RR intervals that differ by more than 50 ms. Vagal index, closely related to RMSSD.
The 2017 Shaffer and Ginsberg Frontiers in Public Health review is the definitive open-access primer on metrics and normative ranges and is recommended reading for any clinician or consumer interpreting HRV data.
Resonance-Frequency Breathing (the Lehrer Protocol)
The single most effective HRV-training intervention is paced breathing at the subject's individual resonance frequency — the breathing rate that produces the largest beat-to-beat heart-rate oscillation. Paul Lehrer and Evgeny Vaschillo developed the canonical protocol (Appl Psychophysiol Biofeedback 2003) and have refined it over twenty subsequent years.
The technique:
- Find the resonance frequency — in a calibration session, the subject breathes at successively slower rates (typically 7.0, 6.5, 6.0, 5.5, 5.0, 4.5 breaths/min) for 2-3 minutes at each rate while HRV is recorded. The rate that produces the largest peak-to-trough heart-rate oscillation is the resonance frequency. Most adults resonate between 4.5 and 6.5 breaths/min, with a population median near 5.5 breaths/min (one breath every ~11 seconds).
- Equal inhalation and exhalation, no breath-hold — at 5.5 breaths/min, that is 5.45 seconds inhale, 5.45 seconds exhale, no hold. Some protocols use a slightly longer exhalation (4 in, 7 out, for instance) to enhance vagal engagement, but Lehrer's original protocol uses equal phases.
- Diaphragmatic breathing — the breath should originate from the diaphragm (abdomen rises on inhalation, falls on exhalation) rather than the chest. Chest breathing fragments the breath into small high-frequency components that disrupt the resonance.
- 20-minute sessions, twice daily — the original protocol prescribes 20 minutes of paced breathing in the morning and 20 minutes in the evening, for 8-10 weeks. After the initial training period, 10-15 minutes once daily maintains the gains.
The mechanism is straightforward: at the resonance frequency, the baroreflex feedback loop and the respiratory sinus arrhythmia are in phase, and the cardiovascular system effectively exercises its own regulatory machinery. Sustained practice strengthens the baroreflex, raises vagal tone, and produces measurable increases in resting HRV, baroreflex sensitivity, and parasympathetic dominance.
Coherence Training (HeartMath)
The HeartMath Institute, founded in 1991, developed a related but distinct biofeedback approach focused on "psychophysiological coherence" — a state of high HRV amplitude concentrated narrowly around the resonance frequency, combined with deliberate cultivation of positive emotional states (gratitude, appreciation, care). The HeartMath protocol uses paced breathing at approximately 6 breaths/min (close to the Lehrer resonance frequency for most adults) combined with attention focused on the heart region and the deliberate generation of a positive emotional state.
The HeartMath research database includes over 300 published papers documenting effects on stress, anxiety, blood pressure, and cognitive performance, including trials in police officers, military personnel, healthcare workers, and corporate populations. The intervention is delivered through the emWave and Inner Balance hardware-software combinations, with real-time visual feedback on coherence.
From a strict psychophysiological standpoint, the HeartMath protocol is a packaging and extension of Lehrer-Vaschillo resonance-frequency breathing with the addition of explicit emotion-regulation training. The added emotion-regulation component may extend the clinical effect beyond pure HRV improvement, particularly in populations where emotional regulation is the primary deficit. The combined protocol has been adopted by multiple government and military programs for resilience training.
Wearable HRV Trackers
The clinical-grade ECG-based HRV measurement of the Lehrer trials is impractical for daily monitoring. The past decade of wearable development has made high-quality HRV measurement accessible to consumers. The principal categories:
- Polar H10 chest strap — the gold-standard consumer device, validated against ECG with sub-millisecond accuracy. The chest strap measures the actual electrical R-wave and is the only consumer device suitable for research-grade HRV. Paired with apps like Elite HRV, HRV4Training, or Lehrer's own Resonance Breath app.
- Oura Ring — measures HRV during sleep via wrist/finger photoplethysmography (PPG). Reports a nightly average HRV (RMSSD) and trends over time. Less accurate than the Polar H10 but more comfortable for daily wear.
- Whoop strap — continuous wrist-worn PPG with focus on athletic recovery. Reports daily HRV and a recovery score.
- Apple Watch — ECG single-lead spot measurement and PPG-based continuous monitoring. The "HRV" reported by Apple Health is SDNN over selected windows.
- Garmin watches — recent Garmin models include wrist-based HRV with daily summary in the Garmin Connect app.
For training (rather than monitoring), the chest-strap solution is strongly preferred: the wrist-based PPG measurements during waking, active hours are unreliable due to motion artifact and the inherently lower temporal resolution of PPG vs ECG. For nightly trend monitoring during sleep, the Oura and Whoop are adequate.
Practical Training Protocol
A practical 8-week training program based on the Lehrer protocol:
- Week 1: Resonance frequency calibration. Using a Polar H10 + Elite HRV (or similar), record 2-minute paced-breathing sessions at 7, 6.5, 6, 5.5, 5, and 4.5 breaths/min. Identify the rate producing the largest heart-rate oscillation. This is your resonance frequency.
- Weeks 2-8: Twice-daily 20-minute sessions. Practice paced breathing at your resonance frequency for 20 minutes in the morning and 20 minutes in the evening. Use the visual breathing pacer in Elite HRV, Inner Balance, or a simple metronome app.
- Weekly check-in. Repeat a 5-minute baseline HRV measurement (no paced breathing, just quiet sitting) once a week to track progress. Baseline RMSSD typically rises 20-40% over 8 weeks.
- Acute stress micro-doses. When stressed during the day, take 1-3 minutes to drop into resonance-frequency breathing. The acute effect is rapid: heart rate falls, blood pressure normalizes, mental clarity returns. Lehrer calls this "carry-over."
- Maintenance. After 8 weeks of training, drop to once-daily 10-15 minute sessions to maintain the gains. Most subjects find a morning session is most sustainable.
The Lin and colleagues meta-analysis (J Hum Hypertens 2012) and Goessl and colleagues meta-analysis (Psychol Med 2017) document that 8 weeks of paced-breathing HRV biofeedback produces sustained reductions in systolic blood pressure (mean ~5 mmHg), diastolic blood pressure (mean ~3 mmHg), and anxiety scores comparable to many pharmacological interventions, with no significant adverse events.
Clinical Evidence (Anxiety, PTSD, Hypertension)
The clinical-trial evidence for HRV biofeedback covers a remarkably broad set of conditions:
- Generalized anxiety disorder — the Goessl 2017 meta-analysis (24 studies, 484 patients) found a large effect size (Hedges' g = 0.83) for HRV biofeedback on self-reported stress and anxiety, with the effect maintained at follow-up.
- Post-traumatic stress disorder — Tan and colleagues (Appl Psychophysiol Biofeedback 2011) tested HRV biofeedback in combat-related PTSD veterans and found significant reductions on the PTSD Checklist and Beck Depression Inventory. Subsequent trials in police officers, first responders, and military populations have confirmed the effect.
- Hypertension — multiple trials have shown 4-8 weeks of HRV biofeedback produces blood pressure reductions of 5-10 mmHg systolic. The mechanism is thought to be improved baroreflex sensitivity rather than acute heart-rate slowing.
- Asthma — Lehrer's group has published several positive trials of HRV biofeedback as adjunctive treatment in adult asthma, with reductions in inhaled steroid requirement.
- Depression — HRV biofeedback as monotherapy or adjunct to antidepressants has shown moderate effect sizes for depression symptom reduction.
- Athletic recovery and performance — resting HRV is widely used by athletes to titrate training load. A morning RMSSD below the individual's rolling baseline signals overreaching and indicates an easy/recovery day; HRV at or above baseline signals readiness for hard training.
- Functional GI disorders — the gut is heavily vagally innervated, and HRV biofeedback has been studied in irritable bowel syndrome, functional dyspepsia, and inflammatory bowel disease with modestly positive results.
Cautions and What HRV Cannot Measure
HRV is a powerful tool but a partial one. Several cautions apply:
- HRV is not a measure of stress per se — it is a measure of autonomic flexibility. Acutely stressful events can produce a transient drop in HRV, but the chronically stressed patient may show normal or even elevated HRV depending on the type of stress and the population baseline.
- Wide normal range. Healthy adults show RMSSD values from below 20 ms to above 100 ms. The clinically relevant question is not the absolute value but the trend within an individual: a 30% drop from one's own baseline is meaningful even if the absolute value is still in the "normal" range.
- Atrial fibrillation invalidates HRV. AFib produces irregular RR intervals that artifactually inflate HRV metrics in a way that does not reflect vagal tone. HRV cannot be meaningfully calculated in AFib patients.
- Beta-blockers raise HRV. Patients on beta-blockers will have elevated HRV that reflects pharmacological blockade rather than vagal tone. Compare within-individual trends rather than absolute values.
- Cardiac arrhythmias and ectopy. PVCs (premature ventricular contractions) and PACs (premature atrial contractions) create RR-interval artifacts that should be filtered before HRV calculation. Quality HRV apps do this automatically.
- Time-of-day matters. HRV varies considerably across the day. Compare apples to apples: morning vs morning, sleep vs sleep, not random daytime spot measurements.
- Caffeine, alcohol, and sleep deprivation all transiently depress HRV. Confounding from these is the principal challenge in interpreting day-to-day variation.
Key Research Papers
- Lehrer PM, Vaschillo E, Vaschillo B, Resonant-frequency biofeedback training to increase cardiac variability: rationale and manual for training (Appl Psychophysiol Biofeedback 2003) — PubMed 12737096
- Lehrer PM, Gevirtz R, Heart rate variability biofeedback: how and why does it work? (Front Psychol 2014) — PubMed 25101026
- Goessl VC, Curtiss JE, Hofmann SG, The effect of heart rate variability biofeedback training on stress and anxiety: a meta-analysis (Psychol Med 2017) — PubMed 28478782
- Thayer JF, Lane RD, A model of neurovisceral integration in emotion regulation and dysregulation (J Affect Disord 2000) — PubMed 11163422
- Thayer JF, Hansen AL, Saus-Rose E, Johnsen BH, Heart rate variability, prefrontal neural function, and cognitive performance (Ann Behav Med 2009) — Search PubMed
- Thayer JF, Yamamoto SS, Brosschot JF, The relationship of autonomic imbalance, heart rate variability and cardiovascular disease risk factors Search PubMed
- Shaffer F, Ginsberg JP, An overview of heart rate variability metrics and norms (Front Public Health 2017) — PubMed 29034226
- Porges SW, The polyvagal theory: phylogenetic substrates of a social nervous system (Int J Psychophysiol 2001) — PubMed 11587772
- Tan G, Dao TK, Farmer L, Sutherland RJ, Gevirtz R, Heart rate variability (HRV) and posttraumatic stress disorder (PTSD): a pilot study (Appl Psychophysiol Biofeedback 2011) — Search PubMed
- Lin G et al., Heart rate variability biofeedback decreases blood pressure in prehypertensive subjects Search PubMed
- Sevoz-Couche C, Laborde S, Heart rate variability and slow-paced breathing: when coherence meets resonance (Neurosci Biobehav Rev 2022) — Search PubMed
- Task Force of the European Society of Cardiology, Heart rate variability: standards of measurement, physiological interpretation, and clinical use (Circulation 1996) — PubMed 8598068
Connections
- Stress Management Benefits Hub
- HPA Axis Regulation
- Adaptogens
- Cold and Sauna Exposure
- Stress Management (Main Page)
- Meditation
- Sleep Hygiene
- Hypertension
- Atrial Fibrillation
- Anxiety
- Depression
- PTSD
- Irritable Bowel Syndrome
- Cortisol Lab Test
- All Remedies