Cold and Sauna Exposure for Stress Management
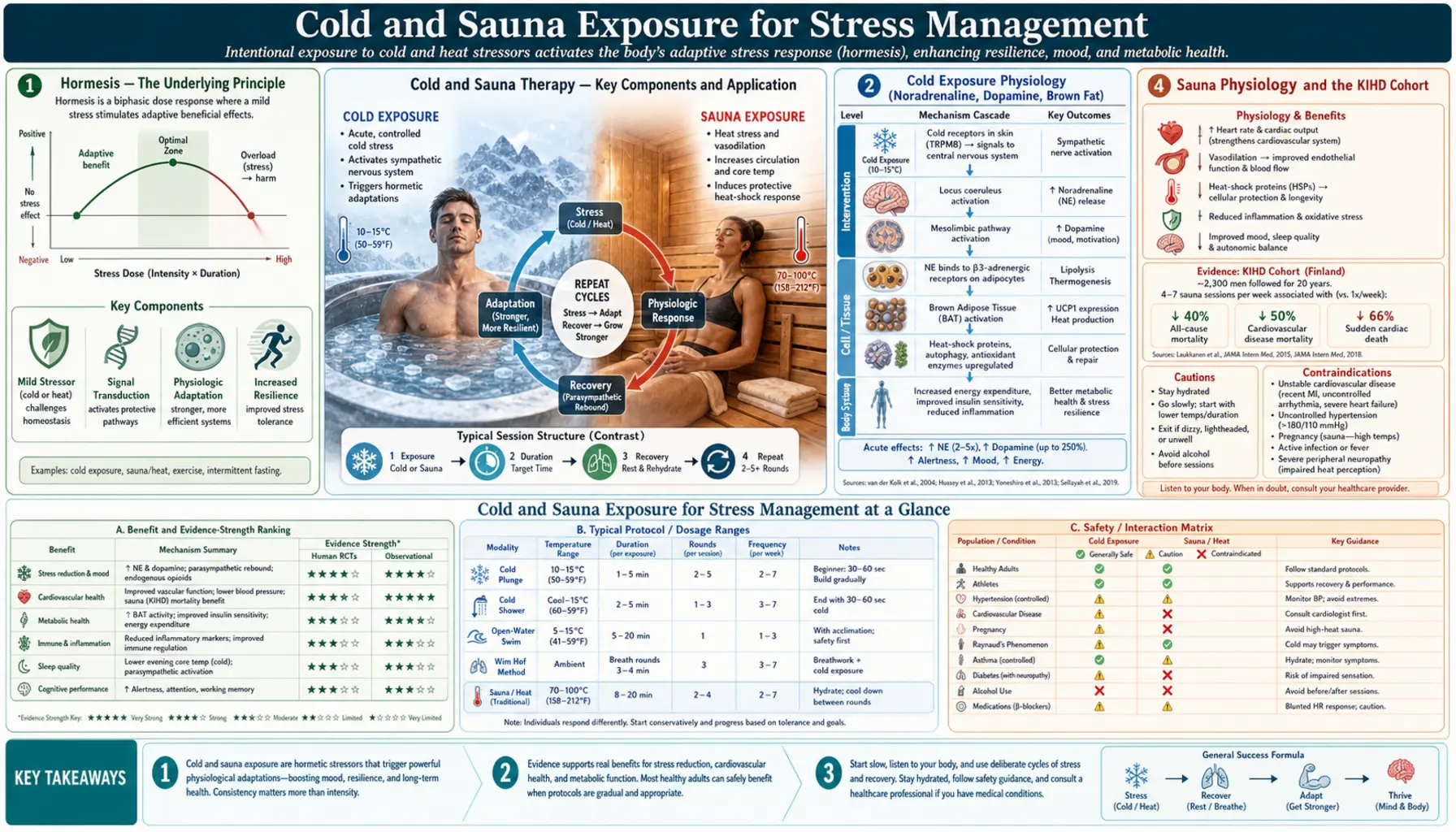
Cold-water immersion and dry-sauna heat are the two most-studied hormetic stressors in the modern stress-management literature. Cold immersion raises plasma noradrenaline 200-530% and dopamine ~250% for hours, producing a sustained mood elevation that has been compared to a controlled pharmacological intervention. Dry-sauna heat — especially the Finnish-style 80-100°C sauna — has been documented in the 25-year prospective Kuopio Ischaemic Heart Disease (KIHD) cohort to halve cardiovascular and all-cause mortality at 4-7 sessions per week. The unifying mechanism is hormesis: a brief, intense, predictable stressor produces adaptive upregulation of the body's stress-defense systems (heat-shock proteins, antioxidant enzymes, baseline vagal tone), with the net effect that subsequent chronic stress produces less downstream damage. This deep dive walks through the physiology of cold and heat exposure, the principal protocols (cold plunge, cold shower, Wim Hof Method, Finnish sauna, infrared sauna, contrast therapy), the documented clinical outcomes, and the contraindications — particularly the genuine arrhythmia and cold-shock risks that make this category not for everyone.
Table of Contents
- Hormesis — The Underlying Principle
- Cold Exposure Physiology (Noradrenaline, Dopamine, Brown Fat)
- Cold Protocols (Plunge, Shower, Open-Water, Wim Hof)
- Sauna Physiology and the KIHD Cohort
- Sauna Protocols (Finnish, Infrared, Contrast)
- The Søberg / Soberg Cold-and-Sauna Protocol
- Mental Health Effects (Depression, Anxiety, Mood)
- Cardiovascular and All-Cause Mortality Evidence
- Contraindications and Risk Management
- Key Research Papers
- Connections
- Featured Videos
Hormesis — The Underlying Principle
Hormesis is a biological dose-response phenomenon in which a low or moderate dose of a stressor produces a beneficial adaptive response, whereas a high dose of the same stressor causes harm. The classic example is exercise: muscular and cardiovascular stress within a tolerable range drives adaptation that makes the body stronger and more resilient; the same stress beyond the tolerable range causes injury and rhabdomyolysis. Cold and heat exposure are pure thermal-stress applications of the same principle.
The molecular machinery of hormesis is well-mapped. Mild stress triggers transcription factors including HSF1 (heat shock factor 1), Nrf2 (nuclear factor erythroid 2-related factor 2), FOXO, and SIRT1, which in turn upregulate a coordinated suite of cytoprotective proteins: heat-shock proteins (HSP70, HSP90), antioxidant enzymes (superoxide dismutase, catalase, glutathione peroxidase), mitochondrial biogenesis factors, and proteostasis machinery. The cell becomes more resistant to subsequent stress of all kinds — what the cardiology literature calls "preconditioning."
The translation to deliberate thermal exposure is direct. A 3-minute cold plunge at 50°F or a 20-minute Finnish sauna at 85°C delivers a brief but intense thermal stress that is well below the tissue-damage threshold but well above the threshold for hormetic transcription-factor activation. Regular practice over weeks-to-months produces measurable upregulation of HSP70, improved antioxidant capacity, and improved tolerance to subsequent stress of any kind — thermal, psychological, infectious, or surgical.
Cold Exposure Physiology (Noradrenaline, Dopamine, Brown Fat)
Sudden cold exposure triggers a coordinated sympathetic activation called the cold-pressor response. The principal acute effects, well-characterized in laboratory studies of subjects immersed to the neck in 40-50°F water:
- Plasma noradrenaline rises 200-530% within the first 30-60 seconds and remains elevated for 1-2 hours after exit. The classic Šrámek 2000 paper (Eur J Appl Physiol) measured peak plasma noradrenaline of 1,800-2,700 pg/mL during whole-body cold-water immersion, compared to baseline ~300-500 pg/mL.
- Plasma dopamine rises ~250% from baseline and remains elevated for ~3 hours. This is an unusual feature — few pharmacological or behavioral interventions produce a sustained dopamine elevation of this magnitude without rapid tolerance.
- Plasma cortisol rises modestly during acute exposure, primarily driven by ACTH release in response to the noradrenergic surge.
- Brown adipose tissue (BAT) activation — cold exposure is the principal physiological activator of brown fat thermogenesis. Brown fat burns glucose and fatty acids for heat via uncoupling protein 1 (UCP1). Regular cold exposure expands BAT mass and BAT activity over weeks; the Søberg 2021 Cell Reports Medicine paper documented substantially elevated BAT activity in winter swimmers compared to controls.
- Improved insulin sensitivity — the BAT activation and the noradrenergic activation jointly improve glucose disposal. Regular cold exposure has documented effects on insulin sensitivity comparable to moderate exercise.
- Reduced inflammation — the Kox 2014 PNAS paper documented that subjects trained in the Wim Hof breathing and cold-exposure method were able to voluntarily attenuate the inflammatory response to endotoxin (LPS) administration, with reduced TNF-α, IL-6, and IL-8 production.
The sustained mood elevation following cold exposure — widely reported anecdotally and now documented in multiple psychophysiology studies — is almost certainly driven by the dopamine elevation. Unlike pharmacological dopamine agonists, the cold-induced rise produces no acute hedonic spike (the experience during immersion is uncomfortable, not pleasurable), and there is no documented tolerance with regular practice.
Cold Protocols (Plunge, Shower, Open-Water, Wim Hof)
The principal cold-exposure protocols differ in intensity, duration, and accessibility:
- Cold shower — the most accessible protocol. End a normal warm shower with 30 seconds to 3 minutes of the coldest setting (typically 50-65°F in residential plumbing). Buijze and colleagues (PLoS One 2016) randomized 3,018 adults to daily cold showers (30, 60, or 90 seconds) for 30 days; the active group had a 29% reduction in self-reported sick-days from work, with no difference between dose groups.
- Cold plunge / ice bath — immersion to the neck in 38-55°F water for 2-5 minutes. The current consumer cold-plunge market (Plunge, Cold Stoic, Ice Barrel) targets ~50°F as a typical setting. The Huberman protocol calls for total weekly cold exposure of ~11 minutes (e.g., 3 minutes × 4 sessions/week at 50°F).
- Open-water swimming — winter swimming in lakes, rivers, or oceans at 40-50°F. The Finnish, Scandinavian, and Russian traditions have centuries of practice. The 2020 BMJ Case Reports paper documented dramatic remission of treatment-resistant depression in a single patient following adoption of weekly cold-water swimming — an anecdote that triggered a wave of clinical research.
- Wim Hof Method — a structured program combining cold exposure with specific breathing technique (3-4 rounds of 30-40 power breaths followed by breath-holding) and progressive cold tolerance training. The 2014 Kox PNAS paper demonstrated that Wim Hof Method practitioners could voluntarily attenuate the LPS inflammatory response — the first documented evidence of voluntary modulation of the innate immune system.
- Cryotherapy chamber — brief (2-3 minute) exposure to extremely cold air (-110 to -140°C) in a commercial whole-body cryotherapy chamber. The very short exposure means much less actual tissue cooling than a 50°F water immersion despite the more dramatic stated temperature. Clinical evidence for cryotherapy chambers is mixed and substantially weaker than for water immersion.
Practical guidance for beginners: start with 30-second cold showers, work up to 1-3 minutes over 4-8 weeks, then consider moving to cold-plunge if you want a more intense stimulus. Frequency matters more than duration — 4×3-minute sessions per week appears more effective than 1×12-minute session per week.
Sauna Physiology and the KIHD Cohort
The Finnish sauna tradition, going back over two thousand years, exposes the body to dry heat at 80-100°C (176-212°F) for 5-30 minutes at a time. Core body temperature rises by 0.5-1.0°C, heart rate roughly doubles (from a typical resting 60-70 bpm to 100-150 bpm), cardiac output increases 60-70%, and significant sweating produces fluid loss of 0.5-1.5 liters per session.
The cardiovascular load is comparable to moderate exercise. Heart rate, stroke volume, and cardiac output increase. Peripheral vasodilation lowers systemic vascular resistance and blood pressure transiently falls during the session, then rebounds in the cooling phase. Repeated sessions appear to drive cardiovascular adaptation similar to exercise: improved endothelial function, lower resting blood pressure, improved arterial compliance, and reduced left ventricular hypertrophy.
The single most influential body of evidence is the Kuopio Ischaemic Heart Disease (KIHD) prospective cohort study of 2,315 middle-aged Finnish men followed from baseline (1984-1989) for over 20 years. The headline findings, published by Tanjaniina Laukkanen and colleagues in JAMA Internal Medicine 2015:
- Compared to men using the sauna 1 time/week, men using the sauna 2-3 times/week had a 22% lower sudden cardiac death (SCD) risk; men using the sauna 4-7 times/week had a 63% lower SCD risk.
- All-cause mortality showed a similar dose-response: 24% lower at 2-3 sessions/week, 40% lower at 4-7 sessions/week.
- Time-per-session also mattered: sessions of >19 minutes were associated with 52% lower SCD risk vs sessions of <11 minutes.
- Subsequent KIHD analyses extended the findings to dementia (66% lower risk at 4-7 sessions/week), Alzheimer's disease, stroke, and hypertension.
The KIHD findings are observational and the population is genetically and culturally distinct, so causal inference and external generalizability require caution. But the consistency of the dose-response across multiple endpoints, the biological plausibility of the cardiovascular and HSP-related mechanisms, and the supporting evidence from short-term randomized trials together make the sauna intervention one of the best-supported lifestyle interventions for cardiovascular and all-cause mortality currently known.
Sauna Protocols (Finnish, Infrared, Contrast)
The three principal sauna modalities differ in heat source and air temperature:
- Finnish (traditional) sauna — wood- or electric-heated stones radiating dry heat at 80-100°C (176-212°F), with occasional water pours (löyly) producing brief humidity spikes. This is the modality of the KIHD evidence. Typical session: 10-20 minutes, 1-2 rounds, with cooling intervals between. Twice-weekly is the minimum dose with documented mortality benefit; 4-7 times/week is associated with the largest effect.
- Infrared sauna — far-infrared (FIR) emitters heating the body directly without significantly heating the surrounding air. Cabin temperatures are much lower (50-65°C) but skin and tissue heating is comparable due to the radiant transfer. Infrared sauna is the closest readily available analog to the Finnish sauna for residential use. Direct mortality evidence is limited (no KIHD-scale infrared cohort exists) but short-term cardiovascular and inflammatory markers respond similarly.
- Steam room (Turkish hammam / Russian banya) — much lower temperature (40-50°C) with very high humidity. The cardiovascular load is lower than a dry Finnish sauna. Documented benefits exist but are smaller in magnitude.
- Contrast therapy — alternating heat (sauna) and cold (plunge or cold shower) in rotating cycles. The Scandinavian tradition (sauna → jump in lake → back to sauna) is the canonical pattern. Contrast amplifies both the sympathetic activation of the cold component and the vasodilatory effect of the heat component; subjects typically report a more dramatic mood elevation than either modality alone.
The Hussain and Cohen 2018 systematic review (Evid Based Complement Alternat Med) catalogs the documented clinical effects across all modalities: reduced blood pressure, improved endothelial function, reduced symptoms of rheumatoid arthritis and ankylosing spondylitis, modest weight reduction (mostly fluid loss with rebound), improved chronic pain, and reduced depression scores.
The Søberg / Soberg Cold-and-Sauna Protocol
Susanna Søberg, a Danish physiologist and the author of the 2022 book "Winter Swimming," has been one of the principal researchers translating Scandinavian cold-and-heat traditions into clinical protocols. Her 2021 Cell Reports Medicine paper compared regular winter swimmers (mean 56 swims/year, mostly without subsequent sauna) to non-swimming controls and found significantly elevated brown adipose tissue activity, improved cold-induced thermogenesis, and improved insulin sensitivity.
The "Søberg principle" articulated in interviews and subsequent writing distills the practical recommendations:
- For cold adaptation: 11 minutes per week total — spread across 2-4 sessions, typically 2-3 minutes per session at 50-55°F. This is the minimum dose with documented metabolic and mood effects.
- For sauna benefit: 57 minutes per week total — spread across 3-7 sessions of 15-20 minutes each. This is roughly the dose associated with the 40% all-cause mortality reduction in KIHD.
- End on cold, not on heat, if the goal is metabolic adaptation — ending on cold preserves the brown-fat activation signal. Ending on heat closes the session with vasodilation and gentle relaxation but blunts the BAT signaling.
- End on heat, not on cold, if the goal is sleep and relaxation — the post-sauna cooling phase, especially in a cooler bedroom, mimics the natural pre-sleep core-temperature drop and facilitates sleep onset.
This is a useful framework but the underlying evidence is more modest than the precision of the numbers suggests; the "11 minutes" and "57 minutes" are extrapolations from non-randomized cohort data, not clinical trial outputs. The numbers are reasonable practical targets but should not be treated as bright lines.
Mental Health Effects (Depression, Anxiety, Mood)
The mental-health literature on cold and sauna exposure is smaller than the cardiovascular literature but has been accelerating since 2018:
- Depression — the 2016 van Tulleken open-water swimming case report in BMJ Case Reports described complete remission of a 17-year history of treatment-resistant depression following adoption of weekly cold-water swimming. A subsequent open trial in Brighton (Massey 2020) documented significant improvement in depression symptoms in 30 patients enrolled in a 10-week supervised sea-swimming program. The 2018 Janssen Hyperthermia trial (JAMA Psychiatry) found a single whole-body hyperthermia session produced significant reduction in depression scores at 6 weeks compared to sham.
- Anxiety — both cold and sauna produce acute sympathetic activation, which counterintuitively can lower chronic anxiety through habituation. Open-water swimming communities report reduced trait anxiety; mechanism is plausibly stress inoculation.
- Mood and well-being — the sustained dopamine elevation following cold exposure produces a 2-3 hour mood elevation that subjects compare to (but find more sustainable than) pharmacological stimulants. The post-sauna parasympathetic rebound produces a complementary calm-and-relaxed state.
- Cognitive function — cold exposure produces transient improvements in attention and working memory immediately after exit (Marx 2024 Eur J Appl Physiol), likely driven by the noradrenergic surge.
- Sleep — evening sauna with subsequent cooling facilitates sleep onset; morning cold exposure advances the circadian phase and supports morning alertness.
Cardiovascular and All-Cause Mortality Evidence
The cardiovascular evidence for sauna is among the strongest for any lifestyle intervention. The principal datasets:
- KIHD (Kuopio Ischaemic Heart Disease) — 2,315 Finnish men, 20+ year follow-up, sauna 4-7×/week associated with 63% reduction in sudden cardiac death and 40% reduction in all-cause mortality vs 1×/week.
- Laukkanen 2018 BMC Medicine — combined sauna and cardiorespiratory fitness showed multiplicative benefit: men with both high fitness and frequent sauna had the lowest cardiovascular and all-cause mortality.
- Patrick & Johnson 2021 (Exp Gerontol) — comprehensive review of sauna as a lifestyle practice for healthspan extension, summarizing the KIHD and supporting short-term mechanistic evidence.
- Cold-water exposure — the mortality evidence is limited because no KIHD-equivalent cold cohort exists. The Esperland 2022 IJCH review concluded that the available evidence supports modest cardiovascular, metabolic, and mood benefits at moderate cold exposure, with non-trivial risk at extreme exposures.
The combined cold-and-sauna evidence supports a reasonable inference that the protective effect is driven by repeated mild sympathetic stress with full subsequent parasympathetic recovery — the same fundamental mechanism that makes exercise cardioprotective. The thermal protocols are best understood as a partial substitute for or supplement to exercise in patients who cannot or will not exercise at sufficient volume, not as a replacement for it.
Contraindications and Risk Management
Both modalities carry genuine risks that exclude meaningful subsets of the population:
- Uncontrolled cardiovascular disease — cold and sauna both significantly load the cardiovascular system. Patients with unstable angina, recent myocardial infarction, severe aortic stenosis, uncontrolled hypertension (>180/110), or recently decompensated heart failure should not undertake either without cardiology clearance.
- Arrhythmia — the acute sympathetic surge of cold immersion can precipitate atrial fibrillation, ventricular ectopy, and (rarely) ventricular tachycardia in susceptible individuals. Patients with documented arrhythmia history should avoid cold-water immersion or undertake it only under medical supervision.
- Cold shock response — sudden whole-body immersion in <60°F water triggers a gasp reflex, hyperventilation, and a vagally mediated heart-rate spike that can be life-threatening, particularly in the first 30 seconds. The leading cause of cold-water swimming deaths is cold-shock-induced cardiac arrest, not hypothermia. Always enter cold water gradually, never alone, never head-first.
- Pregnancy — sauna use in the first trimester has been associated with neural tube defects in some studies; most obstetric guidelines recommend avoiding sauna during pregnancy. Cold exposure is also generally not recommended.
- Dehydration and electrolyte loss — sauna sessions produce 0.5-1.5 L of fluid loss. Rehydrate with water and consider electrolyte replacement; over many sessions, sodium and magnesium replacement matters.
- Alcohol — the combination of alcohol and sauna is the principal cause of sauna-related deaths in Finland. Alcohol impairs thermoregulation, masks warning symptoms, and increases arrhythmia risk. Never use the sauna intoxicated.
- Hyperventilation before breath-holding (Wim Hof and similar protocols) — hyperventilation lowers blood CO₂ without significantly raising O₂, delaying the urge to breathe. Hyperventilation followed by breath-holding underwater has caused multiple drownings. Never practice Wim Hof breathing in or near water.
- Raynaud's phenomenon — severe Raynaud's patients can develop digital ischemia and frank tissue injury with cold exposure; relative contraindication.
- Children and elderly — thermoregulation is less robust at the extremes of age. Shorter durations and closer supervision.
Key Research Papers
- Laukkanen T et al., Association between sauna bathing and fatal cardiovascular and all-cause mortality events (JAMA Intern Med 2015) — PubMed 25705824
- Laukkanen JA, Laukkanen T, Kunutsor SK, Cardiovascular and other health benefits of sauna bathing: a review of the evidence (Mayo Clin Proc 2018) — PubMed 30077204
- Hussain J, Cohen M, Clinical effects of regular dry sauna bathing: a systematic review (Evid Based Complement Alternat Med 2018) — PubMed 29849692
- Søberg S et al., Altered brown fat thermoregulation and enhanced cold-induced thermogenesis in young, healthy, winter-swimming men (Cell Reports Medicine 2021) — Search PubMed
- Kox M et al., Voluntary activation of the sympathetic nervous system and attenuation of the innate immune response in humans (Wim Hof PNAS 2014) — PubMed 24799686
- Šrámek P et al., Human physiological responses to immersion into water of different temperatures (Eur J Appl Physiol 2000) — PubMed 10751106
- Buijze GA et al., The effect of cold showering on health and work: a randomized controlled trial (PLoS One 2016) — PubMed 27631616
- Janssen CW et al., Whole-body hyperthermia for the treatment of major depressive disorder: a randomized clinical trial (JAMA Psychiatry 2016) — PubMed 27172277
- van Tulleken C et al., Open water swimming as a treatment for major depressive disorder (BMJ Case Rep 2018) — PubMed 30131418
- Tipton MJ et al., Cold water immersion: kill or cure? (Exp Physiol 2017) — PubMed 28833689
- Patrick RP, Johnson TL, Sauna use as a lifestyle practice to extend healthspan (Exp Gerontol 2021) — Search PubMed
- Esperland D et al., Health effects of voluntary exposure to cold water — a continuing subject of debate (Int J Circumpolar Health 2022) — PubMed 36137565
Connections
- Stress Management Benefits Hub
- HPA Axis Regulation
- Adaptogens
- HRV Training
- Stress Management (Main Page)
- Cold Therapy
- Sauna
- Exercise
- Hypertension
- Atrial Fibrillation
- Depression
- Anxiety
- Insulin Resistance
- Rheumatoid Arthritis
- All Remedies