HPA Axis Regulation for Stress Management
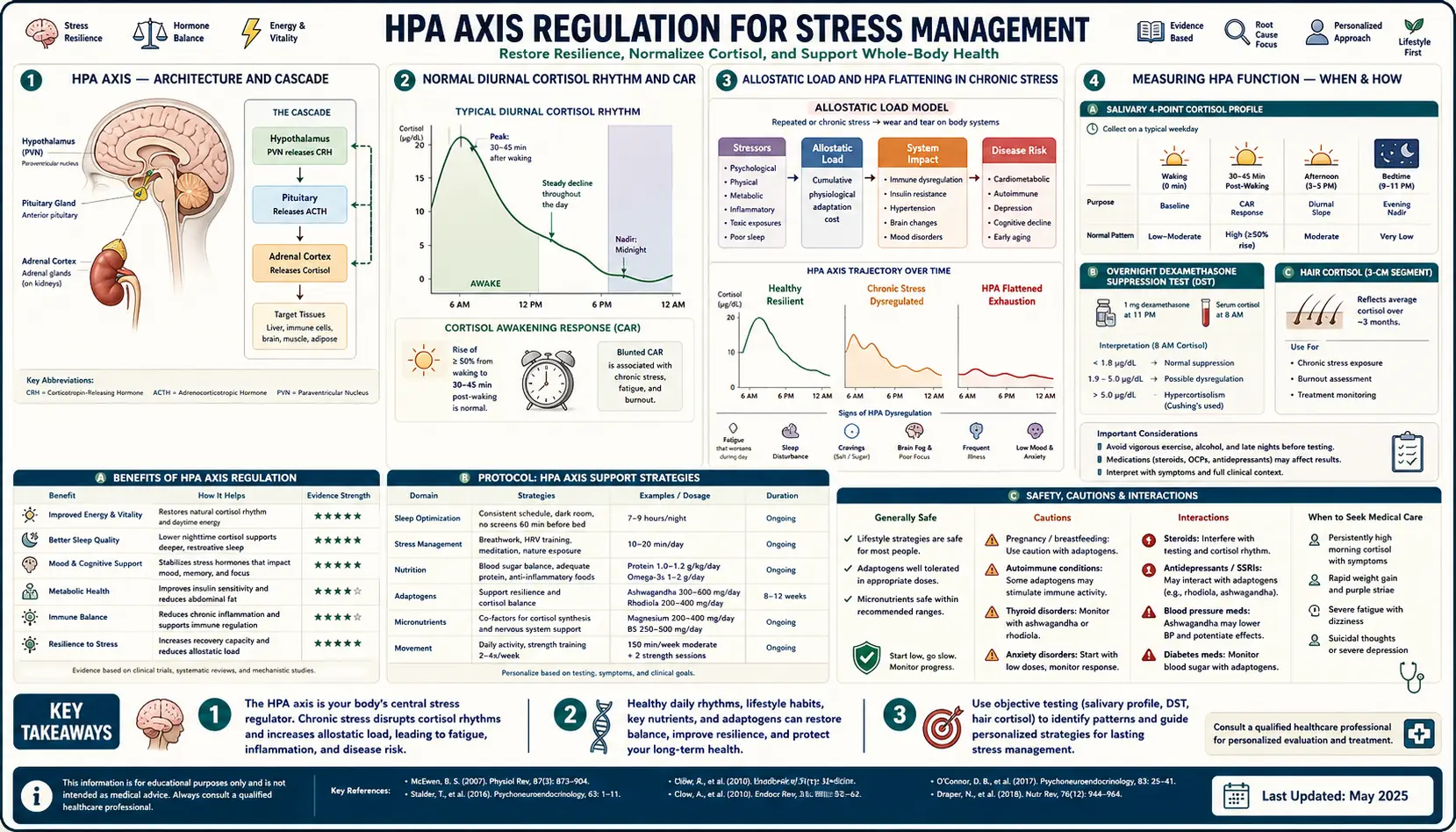
The hypothalamic-pituitary-adrenal (HPA) axis is the body's central stress-response system — a three-part neuroendocrine cascade that runs from a paraventricular hypothalamic nucleus through the pituitary's anterior lobe out to the adrenal cortex, releasing the glucocorticoid hormone cortisol into circulation. Under healthy conditions the axis has a tight diurnal rhythm: cortisol peaks 30-45 minutes after waking (the cortisol awakening response, CAR), rises sharply during acute stress, and falls to a near-zero trough around midnight. Under chronic stress that rhythm flattens, the morning peak disappears, the evening trough fills in, and the body lives in a state of low-grade glucocorticoid exposure that drives insulin resistance, hippocampal atrophy, central adiposity, sleep fragmentation, and bone loss. This deep dive walks through the architecture of the axis, the gold-standard tests for measuring its function, and the four behavioral and pharmacological interventions with the strongest evidence for restoring a healthy diurnal rhythm: mindfulness-based stress reduction (MBSR), cognitive-behavioral therapy for insomnia (CBT-I), phosphatidylserine, and structured sleep hygiene.
Table of Contents
- The HPA Axis — Architecture and Cascade
- The Normal Diurnal Cortisol Rhythm and the CAR
- Allostatic Load and HPA Flattening in Chronic Stress
- Measuring HPA Function (Salivary 4-Point, DST, Hair Cortisol)
- Mindfulness-Based Stress Reduction (MBSR)
- Cognitive-Behavioral Therapy for Insomnia (CBT-I)
- Phosphatidylserine (PS)
- Sleep Hygiene and the HPA Axis
- Cautions and What to Avoid
- Key Research Papers
- Connections
- Featured Videos
The HPA Axis — Architecture and Cascade
The HPA axis is a three-step relay. A psychological or physiological stressor signals the paraventricular nucleus (PVN) of the hypothalamus to release corticotropin-releasing hormone (CRH) and arginine vasopressin (AVP) into the hypophyseal portal blood. CRH binds CRH-R1 receptors on corticotrophs in the anterior pituitary, triggering release of adrenocorticotropic hormone (ACTH) into the systemic circulation. ACTH binds melanocortin-2 receptors (MC2R) on cells of the zona fasciculata of the adrenal cortex, stimulating synthesis and secretion of cortisol. Cortisol then exerts negative feedback at both the hypothalamus and the pituitary, normally completing the loop and returning the system to baseline within 60-90 minutes.
Cortisol acts on virtually every cell in the body through two receptors: the high-affinity mineralocorticoid receptor (MR) and the lower-affinity glucocorticoid receptor (GR). At baseline cortisol concentrations, MR is mostly saturated and GR is occupied only fractionally. During stress, cortisol rises to levels that engage GR throughout the body. Activated GR translocates to the nucleus and either transactivates target genes (gluconeogenesis enzymes, anti-inflammatory mediators, neurotrophic factors) or transrepresses inflammatory transcription factors (NF-κB, AP-1). The net effect of acute cortisol is mobilization of fuel, suppression of non-essential systems (digestion, reproduction, growth), and dampening of inflammation. Acutely, this is adaptive. Chronically, it becomes pathological.
The Normal Diurnal Cortisol Rhythm and the CAR
Cortisol is not secreted at a steady rate. It follows a circadian rhythm driven by the suprachiasmatic nucleus (SCN) of the hypothalamus — the body's master clock — and modulated by pulsatile CRH release every 60-90 minutes. The healthy curve has four features:
- Cortisol awakening response (CAR) — a sharp 50-156% rise in cortisol within 30-45 minutes of waking. This is the single most-studied HPA marker. A blunted CAR is associated with burnout, fibromyalgia, atypical depression, and chronic fatigue. An exaggerated CAR is associated with anticipatory anxiety, melancholic depression, and chronic work stress.
- Daytime decline — cortisol falls progressively across the morning and early afternoon. The slope of the decline (the diurnal cortisol slope, DCS) is a measure of HPA flexibility. A flat slope predicts cardiovascular mortality and accelerated aging.
- Late-afternoon nadir-and-bump — cortisol reaches a relative low around 4-6 PM but typically shows a small late-afternoon rise tied to the evening meal.
- Midnight trough — cortisol falls to near zero between 11 PM and 2 AM. This window is when growth hormone is highest, melatonin peaks, and the immune system is most active. Loss of the trough — elevated 11 PM cortisol — is a robust marker of chronic stress, insomnia, and Cushing's syndrome.
Disrupting any of the four features — through chronic stress, shift work, jet lag, alcohol use, late-night screen exposure, or chronic inflammation — produces measurable HPA dysregulation that downstream interventions can reverse.
Allostatic Load and HPA Flattening in Chronic Stress
The dominant theoretical framework for chronic stress is Bruce McEwen's concept of allostasis and allostatic load, introduced in the 1993 paper "Stress and the individual" and elaborated in his 1998 NEJM review. Allostasis is the active process of maintaining stability through change — the body adjusts its set points to meet challenge. Allostatic load is the cumulative wear-and-tear that accrues when the system is forced to adjust too often, too intensely, or for too long.
The four trajectories that produce pathological allostatic load are:
- Repeated hits — many stressors over time, each within normal range, but cumulatively excessive.
- Lack of adaptation — the system fails to habituate to repeated stressors of the same type, producing full-magnitude responses every time.
- Prolonged response — failure to terminate the stress response once the stressor has passed, leaving cortisol elevated for hours or days.
- Inadequate response — failure to mount an adequate cortisol response to a real stressor, allowing inflammatory and immune cascades that cortisol normally restrains to run unchecked. This is the paradoxical pattern that characterizes chronic fatigue, PTSD, atypical depression, and burnout.
Heim and colleagues (J Psychosom Res 2000) coined the term hypocortisolism for the fourth pattern, in which baseline cortisol is paradoxically low because the axis has been driven to exhaustion or downregulated by chronic feedback. Hypocortisolism is the dominant HPA pattern in long-standing burnout, post-traumatic stress disorder, fibromyalgia, and chronic fatigue syndrome — not the high-cortisol pattern most patients expect.
Measuring HPA Function (Salivary 4-Point, DST, Hair Cortisol)
Three classes of test characterize HPA function. Each measures a different aspect.
- Salivary cortisol four-point curve — the patient collects saliva at four points across the day: immediately on waking, 30 minutes after waking, late afternoon (around 4 PM), and bedtime. The samples are sent to a specialty lab (DiagnosTechs, ZRT, Genova) for cortisol assay. The four values together describe the CAR (samples 1 and 2), the diurnal slope (sample 1 to sample 4), and the evening trough (sample 4). This is the test of choice for outpatient evaluation of chronic stress, burnout, and unexplained fatigue.
- Dexamethasone suppression test (DST) — the patient takes 1 mg of dexamethasone at 11 PM, then measures serum cortisol at 8 AM. Dexamethasone is a synthetic glucocorticoid that should suppress endogenous cortisol via negative feedback. A morning cortisol >1.8 mcg/dL indicates failure of suppression, classically diagnostic of Cushing's syndrome but also seen in melancholic depression. Heuser, Yassouridis, and Holsboer extended this with the combined DEX/CRH test, which adds a CRH bolus the morning after dexamethasone and detects the more subtle HPA hyperactivity that characterizes treatment-resistant depression.
- Hair cortisol — cortisol incorporates into the hair shaft as it grows (~1 cm/month), and a 3 cm segment of hair reflects the integrated cortisol exposure of the previous three months. This is the test of choice for retrospective assessment of chronic stress and for research applications where the within-day rhythm is less important than the long-term mean. Stalder and colleagues (2012, 2016) validated hair cortisol against repeated salivary sampling.
Mindfulness-Based Stress Reduction (MBSR)
MBSR is the most extensively studied non-pharmacological intervention for HPA dysregulation. The original program was developed by Jon Kabat-Zinn at the University of Massachusetts Medical Center in 1979 for patients with chronic pain and stress-related illness. It is an eight-week structured curriculum: 2.5-hour weekly group classes, a full-day silent retreat in week six, and daily home practice of formal meditation (sitting meditation, body scan, gentle yoga) and informal mindfulness (eating, walking, working with present-moment awareness).
The 2017 meta-analysis by Pascoe and colleagues (J Psychiatr Res) pooled 45 randomized trials of MBSR and found significant reductions in systolic blood pressure, salivary cortisol, C-reactive protein, and self-reported stress, with effect sizes consistently in the moderate range (Cohen's d 0.4-0.6). The 2014 JAMA Internal Medicine meta-analysis by Goyal and colleagues found moderate evidence that mindfulness meditation programs reduce anxiety, depression, and pain — comparable in effect size to many active treatments and substantially better than no treatment.
The Tang, Hölzel, and Posner 2015 Nature Reviews Neuroscience review of the neuroscience of mindfulness summarizes the imaging evidence: structural and functional changes in the prefrontal cortex (improved attentional control), the anterior cingulate cortex (improved emotional regulation), the insula (improved interoception), and the hippocampus (volume increases with sustained practice). The amygdala, a major driver of HPA activation, shows reduced reactivity to emotional stimuli. The net mechanistic effect is restored top-down inhibition of the limbic stress-response system.
Cognitive-Behavioral Therapy for Insomnia (CBT-I)
Insomnia and HPA dysregulation are bidirectional — insomnia drives evening cortisol elevation, and evening cortisol elevation drives insomnia. Breaking the cycle is one of the highest-leverage interventions in chronic stress management. CBT-I is the first-line treatment recommended by the American College of Physicians (2016 guidelines) and is more effective than any pharmacological alternative for sustained improvement.
The 2015 Annals of Internal Medicine meta-analysis by Trauer and colleagues pooled 20 randomized trials (1,162 patients) and found CBT-I produced clinically significant reductions in sleep-onset latency (mean 19 minutes), wake-after-sleep-onset (mean 26 minutes), and improvements in sleep efficiency that persisted at 6-12 month follow-up — long after most sleep medications would have lost effect or produced rebound insomnia. The five components are:
- Stimulus control — bed is only for sleep and sex. No reading, no screens, no TV in bed. If awake more than 20 minutes, get out of bed and do something quiet until sleepy.
- Sleep restriction — counterintuitively, restrict time in bed to the amount of actual sleep, even if this means initially sleeping only 5-6 hours. This builds sleep pressure and consolidates fragmented sleep. Once sleep efficiency exceeds 85%, time in bed is gradually extended.
- Cognitive restructuring — identify and challenge catastrophic thoughts about insomnia ("If I don't sleep tonight I won't function tomorrow") that maintain hyperarousal.
- Sleep hygiene — standard recommendations on caffeine, alcohol, light, and temperature.
- Relaxation training — progressive muscle relaxation, autogenic training, or paced breathing to lower presleep arousal.
Vgontzas and colleagues (J Clin Endocrinol Metab 2001) demonstrated that chronic insomniacs have elevated 24-hour cortisol secretion compared to good sleepers, with the elevation concentrated in the evening and early-night hours. Successful CBT-I normalizes the evening cortisol trough and restores the diurnal rhythm.
Phosphatidylserine (PS)
Phosphatidylserine is a phospholipid that is highly concentrated in the inner leaflet of neuronal cell membranes, particularly in the hippocampus and prefrontal cortex. Supplemental PS appears to blunt the cortisol response to acute stress without affecting baseline cortisol secretion — an unusual pharmacological profile that makes it useful in patients with intact HPA architecture but excessive stress reactivity.
The original studies in the 1990s used bovine-cortex-derived PS, which was withdrawn due to bovine spongiform encephalopathy (BSE) concerns. Modern PS is derived from soy lecithin or sunflower lecithin. Hellhammer and colleagues (Stress 2004) showed that 400 mg/day of soy-derived PS for three weeks significantly blunted the cortisol response to the Trier Social Stress Test in healthy young men. Monteleone and colleagues (Eur J Clin Pharmacol 1992) showed 800 mg/day blunted ACTH and cortisol responses to physical exercise. Effects appear within 10-14 days and are dose-dependent up to ~800 mg/day.
Typical clinical dosing is 100-300 mg twice daily, taken with meals. The principal use case is the anxious patient with elevated stress reactivity, particularly when stressful events are predictable (public speaking, athletic competition, examinations). PS is well-tolerated; the principal side effect is gastrointestinal upset at higher doses. There is no known interaction with antidepressants or sedatives at typical doses.
Sleep Hygiene and the HPA Axis
The single most consequential thing most patients can do to restore HPA function is to consistently get 7-9 hours of high-quality sleep, with consistent timing. The mechanisms are well-mapped:
- Light exposure — bright morning light (10,000 lux for 10-30 minutes within an hour of waking) advances the cortisol awakening response and the evening melatonin onset by anchoring the suprachiasmatic nucleus. Conversely, evening blue-light exposure (typically from phone, tablet, or computer screens) suppresses melatonin and shifts the cortisol curve later. Blue-blocking glasses worn 2-3 hours before bed, or hardware filters (Apple Night Shift, f.lux), partially mitigate this.
- Temperature — core body temperature must drop ~1°C for sleep onset. Bedroom temperature in the 65-68°F (18-20°C) range facilitates this. A hot shower or sauna 1-2 hours before bed paradoxically promotes sleep onset by triggering compensatory heat loss.
- Caffeine — half-life is 5-6 hours, longer in women on oral contraceptives and in slow CYP1A2 metabolizers. A 4 PM coffee still has ~25% of the original caffeine load active at midnight, displacing adenosine receptors and fragmenting REM sleep. Drake and colleagues (J Clin Sleep Med 2013) showed 400 mg of caffeine taken 6 hours before bed significantly reduced total sleep time.
- Alcohol — sedating in the first half of the night, then withdrawal-arousing in the second half. Alcohol elevates cortisol acutely and chronically, suppresses REM sleep, and is the single most common modifiable contributor to evening cortisol elevation in middle-aged drinkers.
- Meal timing — a large meal within 3 hours of sleep raises core body temperature and slows sleep onset. The popular intervention of "no food after 7 PM" has reasonable mechanistic support, though specific clinical trial evidence is limited.
Cautions and What to Avoid
Several common interventions look helpful but worsen HPA dysregulation when used chronically:
- Stimulants for "energy" — caffeine, nicotine, and prescription stimulants all activate the HPA axis directly. In the patient with already-elevated daytime cortisol, additional stimulant load worsens the underlying problem. The fix is sleep, not more caffeine.
- Alcohol as a "wind-down" — alcohol fragments sleep architecture and elevates cortisol the morning after. The patient feels worse on a regular wine-with-dinner habit than on no alcohol.
- Chronic glucocorticoid use — oral or injected prednisone, dexamethasone, or other glucocorticoids beyond a few weeks suppress the endogenous HPA axis and produce iatrogenic Cushing's syndrome at one end and addisonian crisis on abrupt withdrawal at the other. Patients on chronic glucocorticoids require gradual taper and stress-dose coverage for surgery and illness.
- "Adrenal fatigue" diagnoses and over-the-counter adrenal extracts — "adrenal fatigue" as a diagnostic label is not recognized by mainstream endocrinology and the supplements marketed for it (often containing bovine adrenal extract or hidden glucocorticoids) can produce iatrogenic adrenal suppression. The proper differential for fatigue and cortisol dysregulation includes hypothyroidism, sleep apnea, Addison's disease, depression, anemia, and undiagnosed sleep deprivation.
- Cushing's syndrome screening — sustained hypercortisolism with central adiposity, easy bruising, purple striae, proximal muscle weakness, and uncontrolled hypertension requires evaluation for Cushing's syndrome (pituitary adenoma, ectopic ACTH, adrenal adenoma) before being treated as "stress."
Key Research Papers
- McEwen BS, Protective and damaging effects of stress mediators (NEJM 1998) — PubMed 9428819
- Sapolsky RM, Romero LM, Munck AU, How do glucocorticoids influence stress responses? (Endocrine Reviews 2000) — PubMed 10696570
- Fries E, Dettenborn L, Kirschbaum C, The cortisol awakening response (CAR): facts and future directions — PubMed 18854200
- Heim C, Ehlert U, Hellhammer DH, The potential role of hypocortisolism in stress-related disorders — PubMed 10633533
- Pascoe MC et al., Mindfulness mediates the physiological markers of stress (meta-analysis 2017) — PubMed 28863392
- Goyal M et al., Meditation programs for psychological stress and well-being (JAMA Intern Med 2014) — PubMed 24395196
- Trauer JM et al., Cognitive Behavioral Therapy for chronic insomnia: systematic review and meta-analysis (Ann Intern Med 2015) — PubMed 26054060
- Vgontzas AN et al., Chronic insomnia is associated with nyctohemeral activation of the HPA axis — PubMed 11502812
- Stalder T et al., Stress-related and basic determinants of hair cortisol (meta-analysis 2016) — Search PubMed
- Tang Y-Y, Hölzel BK, Posner MI, The neuroscience of mindfulness meditation (Nat Rev Neurosci 2015) — PubMed 25783612
- Chrousos GP, Stress and disorders of the stress system (Nat Rev Endocrinol 2009) — PubMed 19488073
- Drake C et al., Caffeine effects on sleep taken 0, 3, or 6 hours before going to bed (J Clin Sleep Med 2013) — PubMed 24235903
Connections
- Stress Management Benefits Hub
- Adaptogens
- HRV Training
- Cold and Sauna Exposure
- Stress Management (Main Page)
- Cortisol Lab Test
- Adrenal Fatigue
- Cushing's Syndrome
- Meditation
- Sleep Hygiene
- Magnesium Glycinate
- L-Theanine
- Ashwagandha
- Anxiety
- Depression