Morley Robbins on the Magnesium Foundation
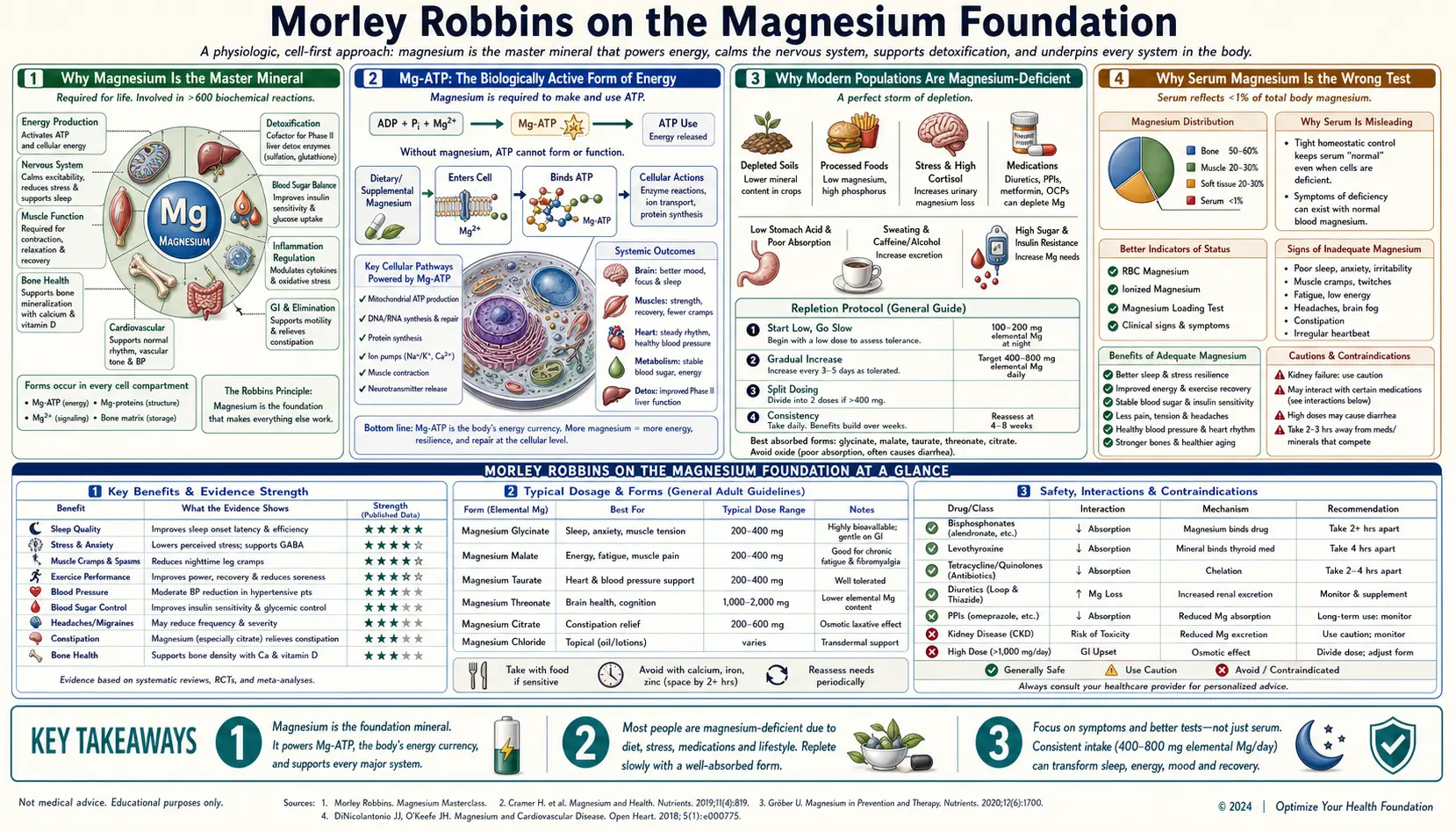
Magnesium is the foundational mineral on which the entire Root Cause Protocol is built. It is a cofactor for more than 800 enzyme reactions in the human body — including every single ATP-dependent reaction, since the biologically active form of ATP is Mg-ATP rather than free ATP. Morley Robbins' argument is that almost all chronic-disease patients are functionally magnesium-deficient, that conventional serum magnesium misses this deficiency in 90%+ of cases (because the body sacrifices intracellular magnesium to maintain serum concentration), and that magnesium repletion is the single most important first step before any other mineral intervention can succeed. This page covers the biochemistry of why magnesium is the master mineral, why serum magnesium is the wrong test, the comparison of supplemental magnesium forms (glycinate, threonate, malate, taurate, citrate, oxide), the food sources Robbins prioritizes, daily protocols, and the cautions for renal and other special populations.
Table of Contents
- Why Magnesium Is the Master Mineral
- Mg-ATP: The Biologically Active Form of Energy
- Why Modern Populations Are Magnesium-Deficient
- Why Serum Magnesium Is the Wrong Test
- Comparing the Supplemental Forms
- Food Sources of Magnesium
- The Magnesium-Copper-Iron Triangle
- Robbins' Daily Magnesium Protocol
- Clinical Applications
- Cautions and Contraindications
- Key Research Papers
- Connections
- Featured Videos
Why Magnesium Is the Master Mineral
Magnesium is the second most abundant intracellular cation (after potassium) and the fourth most abundant cation in the body overall. The adult human body contains approximately 25 g of magnesium, distributed roughly as follows: 60% in bone, 27% in muscle, 6-7% in other soft tissues, and only about 1% in extracellular fluid (with serum magnesium representing a tiny fraction of that 1%).
The functional importance of magnesium is concentrated in two domains:
- Enzymatic cofactor — magnesium is a required cofactor for more than 800 enzyme reactions, including every ATP-dependent reaction in the body. The biologically active form of adenosine triphosphate is Mg-ATP (a magnesium ion chelated to two of the three phosphate groups); free ATP without magnesium is enzymatically inert. This means magnesium is required for protein synthesis, DNA replication, muscle contraction, nerve conduction, neurotransmitter release, glucose metabolism, insulin sensitivity, and the entire electron-transport chain of mitochondrial energy production.
- Membrane stabilizer and ion-channel regulator — magnesium stabilizes the resting membrane potential of excitable cells (neurons, cardiac myocytes, skeletal muscle) by inhibiting calcium influx through voltage-gated calcium channels and by blocking the NMDA glutamate receptor at rest. Magnesium deficiency removes these brakes, producing the cardinal symptoms of hyperexcitability: muscle cramps, twitching, tremor, anxiety, insomnia, arrhythmia, and seizure threshold lowering.
Robbins frames magnesium as the "master mineral" because almost every other mineral function depends on it. Copper loading onto ceruloplasmin requires ATP, which requires magnesium. Iron transport through cell membranes requires ATP, which requires magnesium. Vitamin D activation to 1,25-dihydroxyvitamin D requires three magnesium-dependent enzyme steps. Even calcium homeostasis is partly regulated by magnesium, which suppresses parathyroid hormone release.
Mg-ATP: The Biologically Active Form of Energy
The biochemistry of magnesium and ATP is worth a separate section because it is the mechanistic foundation of why magnesium deficiency presents clinically as fatigue. ATP (adenosine triphosphate) is the universal energy currency of the cell, but free ATP at physiological intracellular pH carries a strong net negative charge from its three phosphate groups (typically a -3 or -4 charge depending on protonation state). This negative charge makes free ATP repel itself and other negatively-charged enzyme active sites, rendering it functionally useless.
Magnesium ion (Mg-2+) binds to two of the three phosphate groups of ATP, neutralizing the negative charge and creating the magnesium-ATP complex that is recognized by every ATP-dependent enzyme in the body. Without sufficient intracellular magnesium, free ATP accumulates but cannot be used. The cell experiences functional ATP deficiency despite having adequate ATP synthesis capacity — the energy is locked up in a form the enzymes cannot recognize.
This is the mechanistic explanation for the most universal symptom of magnesium deficiency: fatigue that is not improved by sleep or stimulants. The patient's mitochondria are making ATP, but the cells cannot use it. Caffeine and stimulants force a transient symptomatic improvement by mobilizing what little Mg-ATP is functionally available, at the cost of further depleting catecholamine reserves. The only correction is to restore intracellular magnesium so that the existing ATP pool becomes biologically usable.
For more on the broader role of mitochondrial function in chronic fatigue, see our Chronic Fatigue Syndrome page or the Cure Your Fatigue book overview.
Why Modern Populations Are Magnesium-Deficient
The pre-industrial human diet, based on whole grains, leafy greens, legumes, nuts, seeds, and mineral-rich water from springs, delivered approximately 500-1,200 mg of magnesium per day. The modern American diet delivers, on average, 250-350 mg/day — well below the RDA of 400 mg for men and 310 mg for women, and dramatically below the pre-industrial intake. The reasons include:
- Soil mineral depletion — intensive monoculture agriculture with high-NPK synthetic fertilizers has progressively depleted soil magnesium over decades. Crops grown on magnesium-depleted soil contain less magnesium per unit weight.
- Refined grain processing — the bran and germ of whole grains contain most of the magnesium. Refining to white flour removes 80%+ of the original magnesium content, and fortification programs add back iron and B-vitamins but not magnesium.
- Water treatment — municipal water softening removes calcium and magnesium. Bottled water and well water in many regions contain meaningful magnesium; "soft" treated tap water contains essentially none.
- Caffeine, alcohol, and refined sugar — all three increase urinary magnesium excretion. Heavy consumption of any of them produces accelerated magnesium loss.
- Diuretic medications — loop diuretics (furosemide), thiazides (HCTZ), and others increase urinary magnesium loss. PPI acid-suppression drugs reduce intestinal magnesium absorption.
- Chronic stress and elevated cortisol — the stress response mobilizes intracellular magnesium and increases urinary excretion. Chronic stress is a chronic magnesium drain.
- Endurance exercise — meaningful magnesium loss through sweat, particularly in heat. Endurance athletes have measurably higher magnesium requirements.
The net effect is that the modern population has subclinical to clinical magnesium deficiency at very high prevalence — estimates from NHANES data and the work of Stefan Pasiakos and others suggest 50-75% of U.S. adults have intake below the RDA, and a significant fraction have RBC magnesium levels in the deficient range.
Why Serum Magnesium Is the Wrong Test
Serum magnesium is the test conventional medicine uses to assess magnesium status, and it is almost useless for that purpose. The reason is that the body prioritizes serum magnesium concentration extremely tightly (the normal range is 1.7-2.2 mg/dL, an unusually narrow range for any electrolyte). When dietary intake drops, the body sacrifices intracellular magnesium — pulling it out of muscle, bone, and other tissue stores — to maintain serum concentration.
The consequence: by the time serum magnesium falls below the lab's reference range (i.e., the patient is labeled "hypomagnesemic"), the intracellular and tissue magnesium has already been profoundly depleted, often by 50% or more. The lab is reporting the very last stage of magnesium deficiency. The patient may have had functional intracellular deficiency — with all the associated symptoms — for years before serum magnesium fell.
The better tests, in order of clinical utility:
- RBC (red blood cell) magnesium — widely available, measures the magnesium content of red blood cells, which reflects intracellular magnesium more closely than serum. Robbins' target is approximately 6.0-6.5 mg/dL (some labs report in mmol/L, where the target is approximately 2.5-2.7 mmol/L). The conventional reference range upper limit is around 6.5 mg/dL, and many "normal" results are actually low-normal and reflect ongoing deficiency.
- Magnesium tolerance test — an IV magnesium load followed by 24-hour urine collection; retention of more than 25% of the load suggests functional deficiency. Cumbersome, rarely done outside research settings.
- Ionized magnesium — the metabolically active fraction of serum magnesium, more sensitive than total serum magnesium but still imperfect.
- EXA Test (Exa Tech intracellular magnesium) — a buccal swab assay measuring intracellular magnesium in epithelial cheek cells, no longer widely available in the U.S. but conceptually the most accurate test when available.
For practical RCP use, RBC magnesium is the standard. The target is 6.0-6.5 mg/dL, and the goal is to reach this within 6-12 months of consistent magnesium repletion through food, supplementation, and topical application.
Comparing the Supplemental Forms
Magnesium supplements come in many forms with substantially different bioavailability, tolerance, and target-tissue distribution:
- Magnesium glycinate (bisglycinate) — magnesium chelated to two glycine amino acid molecules. High bioavailability (~80%), minimal GI side effects, calming due to the glycine. The general-purpose first choice for most RCP patients. Typical dose 200-400 mg elemental magnesium per day.
- Magnesium L-threonate (Magtein) — the only form that has been shown to meaningfully cross the blood-brain barrier and elevate brain magnesium concentration. Preferred for cognitive symptoms, age-related memory issues, and traumatic brain injury recovery. More expensive. Typical dose 1.5-2 g of the compound (~140-200 mg elemental magnesium) per day.
- Magnesium malate — magnesium bound to malic acid, a key intermediate in the Krebs cycle. Often preferred for muscle pain and fibromyalgia, where the malic acid component may contribute to mitochondrial energy support. Typical dose 200-400 mg elemental per day.
- Magnesium taurate — magnesium bound to taurine, an amino acid with cardiovascular and CNS effects. Preferred for cardiovascular indications (arrhythmia, blood pressure) and for patients with co-existing sleep or anxiety issues where the taurine contribution adds benefit.
- Magnesium citrate — magnesium bound to citric acid. Reasonable bioavailability, but pronounced laxative effect at moderate doses. Used clinically as an osmotic laxative; less ideal for daily mineral repletion. Typical dose limited by GI tolerance.
- Magnesium oxide — cheapest and most common in mass-market supplements. Poor bioavailability (~4%), strong laxative effect. Largely useless for actual magnesium repletion despite high label-claimed milligrams per tablet.
- Magnesium chloride — available as oral supplement or as topical "magnesium oil" for transdermal application. Topical magnesium chloride has support from Mark Sircus and others as a way to bypass the GI tract entirely, particularly useful in patients with limited GI tolerance.
- Magnesium sulfate (Epsom salts) — primarily used as a bath additive for transdermal absorption. The magnesium content of an Epsom salt bath that is actually absorbed is modest but consistent with the goal of background repletion.
Robbins' typical protocol combines magnesium glycinate orally (300-400 mg elemental, often split between morning and evening doses) with topical magnesium chloride or Epsom salt baths 2-3 times per week, and emphasis on food sources at every meal. For patients with cognitive symptoms, magnesium threonate is added.
Food Sources of Magnesium
The densest food sources of magnesium per 100 g serving:
- Raw cacao powder: 500 mg
- Pumpkin seeds (pepitas): 535 mg
- Brazil nuts: 376 mg
- Almonds: 270 mg
- Sunflower seeds: 325 mg
- Cashews: 270 mg
- Spinach (cooked): 87 mg (one cup has ~150 mg)
- Swiss chard (cooked): 86 mg
- Black beans: 70 mg
- Avocado: 29 mg
- Dark chocolate (85%): 228 mg
- Tofu: 53 mg
- Quinoa (cooked): 64 mg
- Salmon: 27 mg
- Mineral water (some brands): 10-100 mg/L
For practical reference, a typical American diet of refined grains and conventionally-grown produce delivers approximately 1-2 mg of magnesium per 100 kcal. A magnesium-rich whole-food diet delivers approximately 6-10 mg per 100 kcal. The difference is the entire population deficiency story.
The Magnesium-Copper-Iron Triangle
The integration point for the RCP framework is the magnesium-copper-iron triangle. All three minerals are interdependent:
- Magnesium is required to load copper onto ceruloplasmin — the loading reaction is ATP-dependent, requires Mg-ATP, and fails when intracellular magnesium is depleted. A magnesium-deficient patient cannot achieve normal functional copper status even with adequate dietary copper intake.
- Copper (via ceruloplasmin) is required to safely move iron — as discussed on Copper-Iron Imbalance, ceruloplasmin ferroxidase activity is the rate-limiting step in iron transport. A functionally copper-deficient patient accumulates iron in tissues.
- Excess tissue iron drives oxidative stress that depletes intracellular magnesium — lipid peroxidation damages cell membranes, increases membrane permeability, and accelerates intracellular magnesium loss to the extracellular fluid. Iron overload becomes a magnesium-depletion mechanism.
The clinical consequence is that the three minerals must be addressed together. Repleting magnesium alone produces some symptomatic improvement but does not correct the underlying copper-iron imbalance. Loading copper without adequate magnesium produces minimal functional ceruloplasmin activity. Reducing iron without supporting copper just produces iron deficiency anemia. The protocol works as an integrated whole.
Robbins' Daily Magnesium Protocol
A typical RCP-aligned daily magnesium intake protocol:
- Morning: magnesium glycinate 150-200 mg elemental with breakfast
- Throughout day: magnesium-rich food at every meal — pumpkin seeds on yogurt, dark leafy greens with lunch and dinner, raw cacao or dark chocolate as snack, almonds or cashews
- Evening: magnesium glycinate 150-200 mg elemental at bedtime (the evening dose contributes to sleep onset and quality through GABA-A receptor modulation)
- 2-3 times per week: Epsom salt bath (2 cups Epsom salts in a warm bath, 20 minutes) for transdermal repletion
- Optional: topical magnesium chloride spray on shoulders, abdomen, or calves at bedtime
- Mineral water: when feasible, drink magnesium-rich mineral water (such as Gerolsteiner or other European brands with documented >100 mg Mg/L)
Total elemental magnesium from supplements: ~300-400 mg. From food: another ~300-500 mg. Total daily intake: ~600-900 mg, which is above the RDA but appropriate for repletion of long-standing deficiency. Once RBC magnesium reaches the 6.0-6.5 mg/dL target range, the supplemental dose can be reduced to maintenance levels (typically 200-300 mg/day from supplements, with continued food emphasis).
Side effects to monitor: loose stools or diarrhea indicates the dose has exceeded individual GI tolerance for the specific form being used — reduce dose or switch to a better-tolerated form (glycinate, threonate, malate). Drowsiness is expected with evening dosing and is part of the desired effect.
Clinical Applications
The clinical conditions where magnesium repletion has well-documented benefit, with relevant references:
- Migraine prevention — the American Academy of Neurology gives magnesium a Level B recommendation for migraine prophylaxis (effective). Typical dose 400-600 mg/day elemental.
- Hypertension — meta-analyses show modest but consistent blood pressure reduction (~2-4 mmHg systolic) with daily magnesium supplementation, with larger effects in hypertensive subjects.
- Type 2 diabetes prevention and insulin sensitivity — magnesium intake is inversely associated with type 2 diabetes risk; supplementation improves fasting glucose and HOMA-IR in deficient patients.
- Atrial fibrillation prevention — magnesium supplementation reduces post-cardiac-surgery AF incidence; some evidence for ambulatory AF burden reduction.
- Premenstrual syndrome — modest but consistent reduction in mood symptoms, fluid retention, and dysmenorrhea.
- Restless legs syndrome and nocturnal leg cramps — consistent symptomatic improvement with bedtime magnesium dosing.
- Anxiety and depression — growing evidence base; magnesium glycinate at 200-400 mg elemental at bedtime is a first-line consideration.
- Constipation — magnesium citrate or magnesium oxide as an osmotic laxative.
- Asthma — IV magnesium sulfate is established acute therapy for severe exacerbations; oral magnesium may modestly reduce bronchial reactivity in chronic management.
- Tetany, eclampsia, and torsades de pointes — IV magnesium sulfate is the standard acute treatment for all three.
For more, see our Magnesium overview page and the deep-dive articles on Magnesium Glycinate, Magnesium Threonate, and other forms if available.
Cautions and Contraindications
- Renal insufficiency: the kidneys are the primary route of magnesium excretion. Patients with eGFR <60 mL/min/1.73 m2 have impaired magnesium clearance and are at risk of hypermagnesemia with supplementation. Patients with eGFR <30 should not take magnesium supplements without nephrology guidance.
- Bradyarrhythmia or heart block: magnesium prolongs PR interval modestly and can worsen pre-existing AV block. Use cautiously in patients with second- or third-degree heart block.
- Myasthenia gravis: magnesium reduces acetylcholine release at the neuromuscular junction and can worsen weakness in MG patients. Avoid high-dose supplementation.
- Diarrhea on initiation: common with magnesium oxide, citrate, and sulfate. Switch to glycinate, threonate, or malate, which have minimal GI effect.
- Drug interactions: magnesium chelates oral bisphosphonates, tetracycline and quinolone antibiotics, and levothyroxine, reducing their absorption. Separate magnesium dosing from these drugs by at least 2-4 hours.
- Pregnancy: magnesium is generally safe and often beneficial in pregnancy (associated with reduced pre-eclampsia risk). IV magnesium sulfate is standard for severe pre-eclampsia and eclampsia. Oral supplementation at typical doses is well-tolerated.
- Combined with calcium channel blockers: magnesium has overlapping vasodilator and antiarrhythmic effects; coordinate with the prescribing cardiologist if combining.
Key Research Papers
- de Baaij JH et al. (2015). Magnesium in man: implications for health and disease. Physiol Rev. — PubMed
- Rosanoff A et al. (2012). Suboptimal magnesium status in the United States: are the health consequences underestimated? Nutr Rev. — PubMed
- Workinger JL et al. (2018). Challenges in the diagnosis of magnesium status. Nutrients. — PubMed
- Slutsky I et al. (2010). Enhancement of learning and memory by elevating brain magnesium. Neuron. — PubMed
- Walker AF et al. (2003). Mg citrate found more bioavailable than other Mg preparations. Magnes Res. — PubMed
- Schuette SA et al. (1994). Bioavailability of magnesium diglycinate vs magnesium oxide. JPEN. — PubMed
- Zhang X et al. (2016). Effects of magnesium supplementation on blood pressure: a meta-analysis. Hypertension. — PubMed
- Dong JY et al. (2011). Magnesium intake and risk of type 2 diabetes: meta-analysis. Diabetes Care. — PubMed
- Sun-Edelstein C, Mauskop A (2009). Role of magnesium in the pathogenesis and treatment of migraine. Expert Rev Neurother. — PubMed
- Boyle NB et al. (2017). The effects of magnesium supplementation on subjective anxiety and stress: a systematic review. Nutrients. — PubMed
- DiNicolantonio JJ, OKeefe JH (2018). Subclinical magnesium deficiency: a principal driver of cardiovascular disease and a public health crisis. Open Heart. — PubMed
- Uwitonze AM, Razzaque MS (2018). Role of magnesium in vitamin D activation and function. J Am Osteopath Assoc. — PubMed
PubMed Topic Searches
- PubMed: Magnesium and ATP enzyme function
- PubMed: RBC magnesium assessment
- PubMed: Magnesium form comparison
- PubMed: Mg and vitamin D activation
- PubMed: Mg migraine prophylaxis
Connections
- Morley Robbins Hub
- Benefits Deep Dive
- Copper-Iron Imbalance
- Whole Food Copper Sources
- RCP Lab Panel
- Magnesium Replenishment
- Root Cause Protocol
- Cure Your Fatigue
- Magnesium
- Copper
- Iron
- Vitamin D3 (Mg-dependent activation)
- Hypertension
- Type 2 Diabetes
- Migraine