Morley Robbins on the RCP Lab Panel
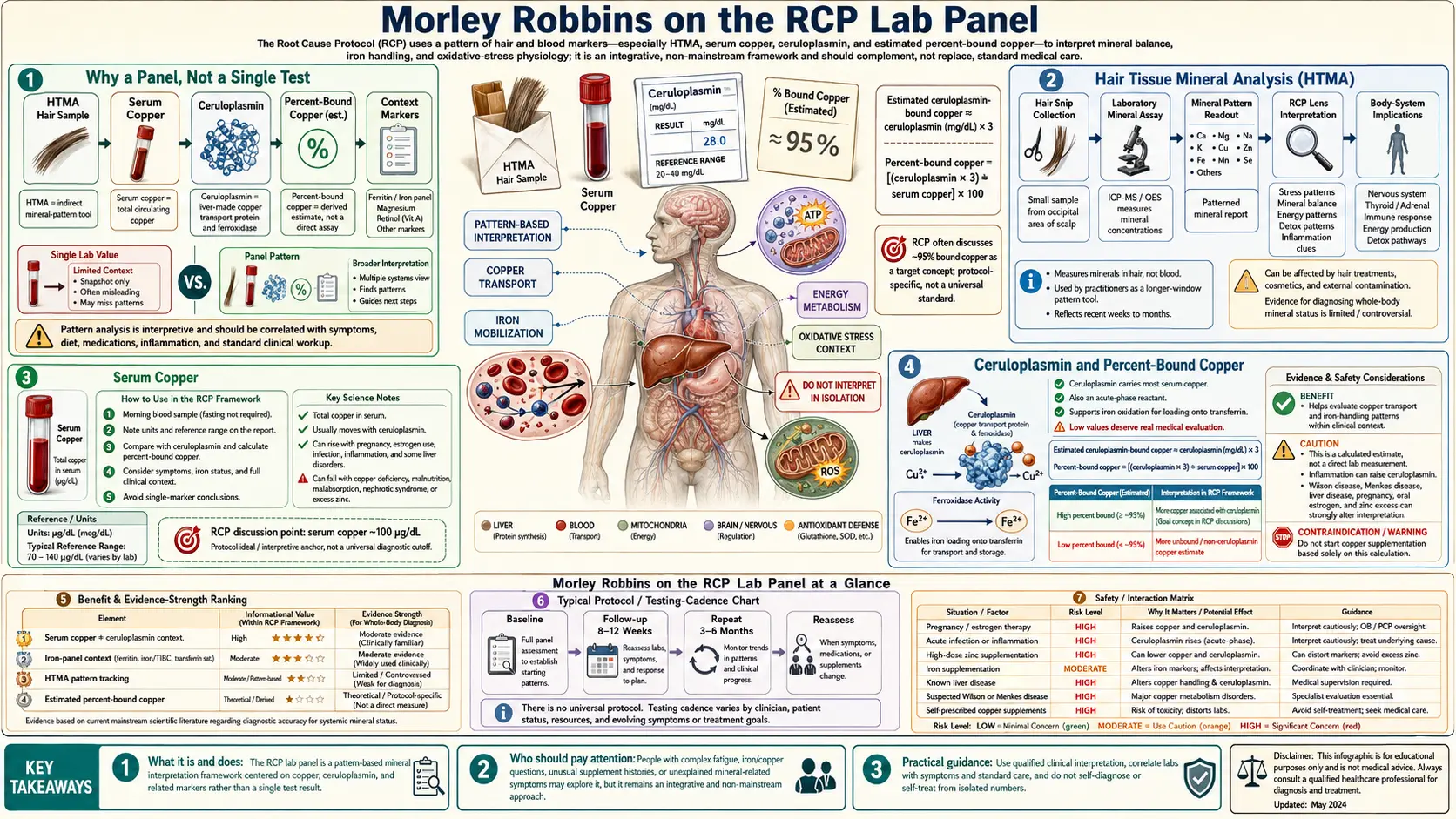
The Root Cause Protocol (RCP) Lab Panel is Morley Robbins' recommended set of blood and hair tests for objectively tracking copper-iron metabolism over time. It is not a single proprietary test — it is a curated assembly of widely-available assays (Hair Tissue Mineral Analysis, serum copper, ceruloplasmin with calculated %-bound, full iron panel, ferritin, magnesium RBC, retinol-binding protein) that, when interpreted together rather than in isolation, reveal the functional copper deficiency / iron dysregulation pattern that drives most chronic-fatigue and inflammatory symptom complexes. This page walks through each marker, the relationships between markers, how to order the tests through both specialty labs (Doctor's Data, Trace Elements) and conventional labs (LabCorp, Quest), how to sequence baseline vs. follow-up testing, and how to read the panel as a coherent whole rather than as a set of independent reference-range judgments.
Table of Contents
- Why a Panel, Not a Single Test
- Hair Tissue Mineral Analysis (HTMA)
- Serum Copper
- Ceruloplasmin and Percent-Bound Copper
- The Full Iron Panel: Serum Iron, TIBC, UIBC, Saturation
- Ferritin and the Low-End-of-Range Interpretation
- Retinol-Binding Protein
- Magnesium RBC
- Supporting Markers (Vitamin D, CRP, CBC, Liver Enzymes)
- Sequencing: Baseline, Follow-Up, and Timing
- Lab Vendor Options
- Reading the Panel Together
- Common Patterns
- Cautions and Limitations
- Key Research Papers
- Connections
- Featured Videos
Why a Panel, Not a Single Test
Conventional medicine's evaluation of mineral status typically consists of a single marker per question: ferritin for iron stores, serum copper for copper status, RBC magnesium (sometimes) for magnesium status. Each marker is interpreted against its own reference range in isolation. The RCP approach rejects this framing as biochemically incoherent. Copper and iron are obligate metabolic partners through the ferroxidase enzymes; ceruloplasmin is functionless without copper loading; iron handling cannot be assessed without simultaneously assessing the copper-dependent machinery that moves it; and magnesium is the cofactor for the ATP-dependent steps that load both minerals onto their carrier proteins. Reading any one marker without the others guarantees misinterpretation.
The RCP panel is therefore designed as a system view. The clinician orders the full set at baseline, then tracks changes in the pattern over time as dietary and supplemental interventions take effect. A single elevated serum copper means one thing if ceruloplasmin is loaded and another if ceruloplasmin is unloaded. A "normal" ferritin means one thing in a non-inflamed patient and another in someone with CRP of 12 mg/L. The panel's value lies in the relationships between markers, not in the individual numbers.
Hair Tissue Mineral Analysis (HTMA)
Hair Tissue Mineral Analysis is the keystone test of the RCP panel and one of the few tests that Robbins considers genuinely non-optional. A small sample (approximately one tablespoon) of hair clipped close to the scalp, typically from the back of the head, is sent to a reference laboratory where the inorganic mineral content is measured by inductively coupled plasma mass spectrometry (ICP-MS). The output is a quantitative report showing approximately 30 minerals and toxic metals, expressed in micrograms per gram (mcg/g) of hair, along with key ratios (calcium-to-magnesium, sodium-to-potassium, calcium-to-potassium, zinc-to-copper) that have decades of empirical pattern interpretation behind them.
The advantage of hair analysis over serum testing is that hair represents a longitudinal tissue record rather than a snapshot. Hair grows approximately half an inch per month, so a 1.5-inch sample reflects mineral deposition over roughly the preceding three months. The minerals are sequestered in the keratin matrix as the hair shaft is formed at the follicle, capturing what was bioavailable in the body during that growth window. Serum tests, by contrast, reflect what is in the bloodstream at the moment the tube is drawn — a value that the body actively defends through hormonal and renal homeostasis and that often masks tissue-level deficiency or excess.
For the copper-iron framework, the key HTMA findings to look for include: low hair copper (suggesting tissue copper depletion, since serum may be normal while tissue is depleted), elevated hair calcium with low magnesium (the "slow oxidizer" metabolic pattern), elevated hair iron (consistent with tissue iron deposition), and zinc-to-copper ratio greater than 12 (suggesting copper displacement from chronic zinc exposure). Toxic metals — mercury, lead, cadmium, aluminum, arsenic — are also reported and may reveal exposures the patient is unaware of.
Serum Copper
Serum copper is the most familiar copper marker and the one most often misinterpreted. The conventional reference range in adults is typically 70-140 mcg/dL, with values above the upper limit sometimes labeled "copper toxicity." The Robbins reading is more nuanced: serum copper reflects the sum of ceruloplasmin-bound copper (the metabolically active fraction) and non-ceruloplasmin-bound copper (the unbound, potentially redox-active fraction), and the interpretation depends entirely on the ratio between these two fractions, which can only be calculated when ceruloplasmin is measured concurrently.
The optimal RCP target for serum copper is approximately 100-120 mcg/dL in women and 90-110 mcg/dL in men, with the caveat that the number is only meaningful in the context of ceruloplasmin. A serum copper of 130 mcg/dL with a ceruloplasmin of 35 mg/dL (well-loaded) is favorable; the same serum copper of 130 mcg/dL with a ceruloplasmin of 18 mg/dL (under-loaded) signals a substantial pool of unbound copper that is not doing the work of the active enzyme.
Serum copper is mildly affected by estrogen state (oral contraceptives, hormone replacement therapy, and pregnancy all raise it by stimulating hepatic ceruloplasmin synthesis), acute inflammation (ceruloplasmin is a positive acute-phase reactant), and recent zinc intake (high zinc suppresses copper absorption over weeks). Sample handling is straightforward — serum copper is stable in standard red- or gold-top tubes at room temperature for several hours and refrigerated overnight.
Ceruloplasmin and Percent-Bound Copper
Ceruloplasmin is the most diagnostically valuable single marker in the RCP panel. It is the alpha-2 glycoprotein synthesized in hepatocytes that carries approximately 95% of the body's circulating copper and performs the ferroxidase reaction that converts ferrous iron (Fe-2+) to ferric iron (Fe-3+) for loading onto transferrin. Each ceruloplasmin molecule contains six tightly-bound copper atoms when fully loaded; without all six copper atoms in place, the protein is still secreted into the bloodstream and still measured by immunoassay, but it lacks enzymatic activity. This distinction — between immunoreactive ceruloplasmin (mass-based) and enzymatic ceruloplasmin (activity-based) — is the central diagnostic point of the panel.
The typical conventional reference range for serum ceruloplasmin is 20-35 mg/dL. The Robbins target is the upper portion of this range, approximately 30-35 mg/dL, with the understanding that values in the low end of normal often coexist with frank functional ceruloplasmin deficiency. Specialty reference laboratories (Mayo, ARUP) offer a separate ceruloplasmin oxidase activity assay that measures the enzymatic capacity directly; this is the gold-standard test for functional copper status but is not routinely ordered by primary care physicians.
The clinically useful surrogate is the calculated percent-bound copper, derived from the relationship: each mg/dL of ceruloplasmin should carry approximately 3 mcg/dL of copper. The formula is: %-bound = (ceruloplasmin mg/dL × 3) / serum copper mcg/dL × 100. A normally-loaded ceruloplasmin yields a %-bound value of approximately 80-95%. Values below 80% suggest under-loading; values below 70% suggest substantial unbound copper and are the classic RCP signature of functional copper deficiency despite numerically "normal" total copper. The non-ceruloplasmin-bound copper fraction can be calculated by subtraction: serum copper − (ceruloplasmin × 3) = unbound copper, which should ideally be under 10 mcg/dL.
The Full Iron Panel: Serum Iron, TIBC, UIBC, Saturation
A complete iron panel is essential for understanding the iron side of the copper-iron equation. Ordering ferritin alone — the conventional shortcut — misses most of the actionable information. The four core iron markers, each providing distinct physiological information, are:
- Serum iron (reference 60-170 mcg/dL): a snapshot of iron bound to transferrin in the moment of the draw. Subject to substantial diurnal variation (morning values are typically higher than evening) and to recent dietary iron intake.
- Total iron-binding capacity (TIBC) (reference 250-450 mcg/dL): a measure of how much transferrin is available to carry iron. TIBC rises in iron deficiency (the body upregulates transferrin synthesis to capture scarce iron) and falls in iron overload, inflammation, malnutrition, and liver disease.
- Unsaturated iron-binding capacity (UIBC): the portion of TIBC not currently occupied by iron. UIBC = TIBC − serum iron. Some labs report this directly rather than calculated.
- Transferrin saturation (TSAT): the percentage of transferrin currently carrying iron, calculated as serum iron / TIBC × 100. The RCP optimal range is 25-35%. Values below 20% suggest iron deficiency; values above 45% suggest iron overload or hemochromatosis-spectrum disease and warrant further evaluation.
Transferrin saturation is the single most useful iron marker for the RCP framework because it directly reflects the functional efficacy of the copper-dependent ferroxidase machinery. When ceruloplasmin is unloaded, freshly-absorbed iron cannot be efficiently oxidized and loaded onto transferrin, so TSAT remains low even when total body iron (as reflected in ferritin) is rising. A pattern of low or low-normal TSAT (15-22%) coexisting with elevated ferritin (above 100 ng/mL) is the diagnostic fingerprint of functional copper deficiency / iron dysregulation. Conventional medicine reads the low TSAT as iron deficiency and prescribes iron; the RCP reading is the opposite — the problem is unbound iron piling up in tissues because the ferroxidase loading step is broken.
Ferritin and the Low-End-of-Range Interpretation
Ferritin is the intracellular iron-storage protein, and its serum concentration is conventionally treated as a clean proxy for total body iron stores. The Robbins reading of ferritin departs sharply from conventional practice on two points: the optimal range and the acute-phase confound.
Optimal range: the conventional reference range for serum ferritin (typically 15-200 ng/mL in women, 30-400 ng/mL in men) reflects what is statistically common in an iron-fortified population, not what is biologically optimal. Robbins targets are substantially lower: approximately 30-50 ng/mL in women and 50-70 ng/mL in men, with anything sustained above 80 ng/mL flagged for evaluation and anything above 150 ng/mL considered a definite signal for iron reduction (typically through therapeutic phlebotomy / blood donation). These targets align with the Iron Disorders Institute recommendations and with the hemochromatosis-prevention literature.
Acute-phase confound: ferritin is a positive acute-phase reactant. Inflammation of any kind — bacterial or viral infection, autoimmunity, obesity, recent vaccination, even intense exercise within the prior 48 hours — elevates serum ferritin independently of iron stores. A "normal" or elevated ferritin in an inflamed patient may coexist with frank bone-marrow iron deficiency. The RCP rule is to always interpret ferritin alongside a high-sensitivity C-reactive protein (hsCRP): if hsCRP is greater than 3 mg/L, the ferritin reading is suspect and should be repeated when inflammation has resolved. When ferritin is elevated and hsCRP is also elevated, the elevated ferritin may simply reflect inflammation rather than true iron overload; when ferritin is elevated and hsCRP is normal, the elevation almost certainly reflects true iron loading.
Trend matters more than any single value. A ferritin that is rising over serial measurements — even within the conventional reference range — signals progressive iron accumulation and warrants intervention. A ferritin that is falling toward the RCP target with intervention is the goal.
Retinol-Binding Protein
Retinol-binding protein (RBP, or more specifically RBP4) is the carrier protein that transports vitamin A (retinol) from hepatic stores to peripheral tissues. It is included in the RCP panel for two reasons. First, vitamin A is a required cofactor for hepatic ceruloplasmin synthesis — without adequate retinol, the liver cannot produce well-loaded ceruloplasmin even when copper intake is adequate. Second, RBP is a sensitive marker of both vitamin A status and hepatic protein synthesis capacity, both of which bear on the entire copper-iron-ceruloplasmin axis.
The reference range for serum RBP4 varies by laboratory but typically falls between 30-75 mcg/mL in adults. The RCP target is the middle to upper portion of this range. Low RBP4 (below 30 mcg/mL) suggests either vitamin A insufficiency, protein malnutrition, zinc deficiency (zinc is required for hepatic RBP synthesis), or chronic liver disease. Elevated RBP4 (above 80 mcg/mL) has been associated with insulin resistance and is sometimes used as a marker of metabolic dysfunction.
The clinical implication: a patient with low ceruloplasmin and low RBP often responds better to vitamin A repletion (from cod liver oil or beef liver, not synthetic retinyl palmitate) than to copper repletion alone. The two interventions are synergistic, and the RBP value indicates which to prioritize.
Magnesium RBC
Serum magnesium is one of the least useful magnesium markers in the laboratory catalog. Only approximately 1% of total body magnesium is in the serum compartment, and the body defends this 1% aggressively through renal reabsorption and bone exchange. By the time serum magnesium drops below the reference range, intracellular magnesium has typically been depleted for years.
The RCP panel uses magnesium RBC (erythrocyte magnesium) instead, because it reflects the intracellular magnesium pool that is more clinically meaningful. The reference range for magnesium RBC is approximately 4.2-6.8 mg/dL, with the RCP target in the upper portion of the range (5.5-6.5 mg/dL). Values below 5.0 mg/dL are interpreted as functionally depleted regardless of where they fall in the conventional reference range, and warrant intervention with a well-tolerated magnesium form (glycinate, malate, or threonate). See the Magnesium Foundation page for the full treatment rationale and titration approach.
Magnesium status bears on the copper-iron panel because magnesium is a cofactor for the ATP-dependent steps in both ceruloplasmin loading and transferrin loading, and because magnesium depletion drives hepatic iron deposition through multiple mechanisms documented in the experimental nutrition literature. A patient with persistently low magnesium RBC is unlikely to normalize their copper-iron panel without first restoring magnesium.
Hair magnesium, reported on the HTMA, provides a complementary longitudinal view and is interpreted alongside the magnesium RBC value rather than in place of it.
Supporting Markers (Vitamin D, CRP, CBC, Liver Enzymes)
Beyond the core copper-iron markers, the full RCP workup typically includes several supporting tests that contextualize the panel and identify confounders:
- 25-hydroxyvitamin D: not directly part of the copper-iron axis, but vitamin D activation requires magnesium, and high-dose synthetic vitamin D supplementation depletes magnesium and may worsen the copper-iron imbalance. The Robbins target is the lower end of the conventional reference range (40-60 ng/mL) from sun exposure when possible, rather than aggressive supplementation toward the upper range.
- High-sensitivity C-reactive protein (hsCRP): essential for interpreting ferritin. Target is below 1.0 mg/L; values above 3 mg/L invalidate ferritin as a clean iron-store marker until the inflammation is resolved.
- Complete blood count (CBC) with differential: hemoglobin, hematocrit, MCV, MCH, MCHC, and RDW provide the hematology context. Iron deficiency anemia typically presents with microcytic hypochromic indices (low MCV, low MCH); functional copper deficiency may present with normocytic or macrocytic anemia and elevated RDW.
- Comprehensive metabolic panel with liver enzymes (ALT, AST, GGT, alkaline phosphatase): elevated ALT and AST may indicate hepatic iron deposition; GGT is a sensitive marker of hepatobiliary stress and oxidative load; alkaline phosphatase is a zinc-dependent enzyme and can be low in zinc deficiency.
- Thyroid panel (TSH, free T4, free T3, reverse T3): copper is required for the deiodinases that convert T4 to T3, and the symptom overlap between functional copper deficiency and hypothyroidism is substantial. A full thyroid panel helps distinguish primary thyroid pathology from copper-deficient T3 conversion failure.
- Fasting insulin and HbA1c: iron overload is strongly associated with insulin resistance and type 2 diabetes; tracking glycemic markers alongside the iron panel reveals the metabolic consequences.
Sequencing: Baseline, Follow-Up, and Timing
The recommended sequence for new patients is:
- Baseline draw, week 0: order the full panel after at least 12 hours of fasting, with the patient off any iron supplements for one week, off any high-dose vitamin C (above 250 mg/day) for two weeks, and off any high-dose zinc (above 25 mg/day) for two weeks if possible. Morning collection (before 10 a.m.) is preferred to control for diurnal variation in serum iron. The HTMA hair sample can be collected at any time.
- First follow-up, 3 months: repeat the full panel after three months of intervention. Three months is the typical window for ferritin and ceruloplasmin to show meaningful change in response to dietary and supplemental adjustments, and matches one HTMA hair-growth cycle.
- Ongoing monitoring, 6-12 months: once a stable pattern is established, the panel can be repeated every 6-12 months for monitoring. Patients on therapeutic phlebotomy for iron reduction typically check hemoglobin and ferritin between donations and the full panel annually.
If the baseline panel reveals an acute inflammatory state (hsCRP greater than 5 mg/L), defer interpretation of ferritin until inflammation resolves. If the baseline reveals hemoglobin below the donor cutoff (typically 12.5 g/dL in women, 13.0 g/dL in men), evaluate for true iron deficiency anemia versus anemia of chronic disease before pursuing iron-reduction strategies.
Lab Vendor Options
The RCP panel does not require any single proprietary vendor and can be assembled from any combination of specialty and conventional laboratories. The most commonly used vendors:
- Doctor's Data (St. Charles, IL): long-established specialty reference lab offering HTMA, urine essential and toxic elements, and stool tests. Their HTMA report includes the standard 30+ mineral profile with mineral ratios and interpretive commentary. Patient pricing is in the $80-120 range and the test can be ordered through a practitioner account or, in many states, direct-to-consumer through telehealth services.
- Trace Elements Inc. (Addison, TX): another well-regarded HTMA specialty lab with a slightly different reporting format that emphasizes oxidation type (fast vs. slow oxidizer) alongside the mineral values. Pricing is similar to Doctor's Data.
- LabCorp and Quest Diagnostics: the two major U.S. clinical reference labs can run the full serum panel (copper, ceruloplasmin, iron panel with TIBC and saturation, ferritin, RBP, magnesium RBC, hsCRP, CBC, CMP, thyroid panel, vitamin D, insulin, HbA1c). Most components are covered by U.S. health insurance when ordered by a physician; ceruloplasmin oxidase activity is a less common send-out and may require Mayo Clinic Laboratories or ARUP referral.
- Direct-to-consumer services (Ulta Lab Tests, Walk-In Lab, Quest QuestDirect, LabCorp OnDemand): allow ordering most of the serum components without a physician referral in most U.S. states, with cash pricing typically running $200-400 for the full panel. HTMA must be ordered through a practitioner account or through one of the specialty labs' consumer programs.
- Mosaic Diagnostics (formerly Great Plains Laboratory): offers a metals panel and an organic acids test that complement but do not replace the core RCP panel.
For patients outside the U.S., equivalent reference labs exist in most developed countries (Biolab in the UK, ARL in Australia, Genova/CDSA worldwide). The specific lab vendor matters less than consistency — once a vendor is chosen, all follow-up testing should be done at the same lab to keep methodology and reference ranges consistent over time.
Reading the Panel Together
The RCP panel is read as an integrated whole. A worked example: a 42-year-old woman presents with chronic fatigue, hair loss, cold intolerance, anxiety, and a borderline-low TSH. Her panel returns:
- Serum copper: 142 mcg/dL (above reference range)
- Ceruloplasmin: 19 mg/dL (low-normal)
- Calculated %-bound copper: (19 × 3) / 142 × 100 = 40% (markedly low; target 80-95%)
- Calculated unbound copper: 142 − (19 × 3) = 85 mcg/dL (markedly high; target under 10)
- Serum iron: 65 mcg/dL (low-normal)
- TIBC: 410 mcg/dL (high-normal)
- Transferrin saturation: 16% (low; target 25-35%)
- Ferritin: 180 ng/mL (elevated; RCP target 30-50)
- hsCRP: 0.8 mg/L (normal)
- Magnesium RBC: 4.6 mg/dL (low-normal)
- RBP4: 28 mcg/mL (low)
- HTMA: low hair copper, elevated hair calcium, zinc-to-copper ratio of 14
The pattern is classic functional copper deficiency with iron dysregulation. The body has copper in circulation (total serum copper is elevated), but it is unbound — ceruloplasmin is under-loaded, so the copper cannot do its enzymatic work. Iron transport is failing: TSAT is low because the ferroxidase step is broken, while ferritin is elevated because iron is being deposited in tissues rather than circulating safely on transferrin. The patient is not iron-deficient and would not benefit from iron supplementation; she is iron-dysregulated and needs ceruloplasmin support (retinol, magnesium, whole-food copper). The HTMA confirms tissue copper depletion and excess zinc displacement.
The therapeutic intervention: stop any iron supplements, stop high-dose isolated vitamin C, stop isolated zinc supplements, add beef liver 1-2 oz daily, add a well-tolerated magnesium form titrated toward the RCP magnesium target, add cod liver oil for whole-food vitamin A, and consider one therapeutic phlebotomy to reduce the elevated ferritin. Repeat the panel at three months and expect to see ferritin trending toward 80 ng/mL, ceruloplasmin trending toward 25 mg/dL, %-bound copper rising above 70%, and TSAT rising into the 20s.
Common Patterns
Several recurring patterns appear on RCP panels in the patient populations Robbins describes:
- Classic functional copper deficiency / iron dysregulation: elevated total copper, low ceruloplasmin, low %-bound copper, elevated unbound copper, low TSAT, elevated ferritin, low magnesium RBC, low RBP. Most common pattern in chronic-fatigue presentations.
- Iron deficiency anemia (genuine): low hemoglobin, low MCV, low MCH, low serum iron, high TIBC, low TSAT (under 15%), low ferritin (under 30 ng/mL), normal copper and ceruloplasmin. Warrants iron repletion alongside copper-supportive measures.
- Anemia of chronic disease / inflammation: low hemoglobin with normal-to-elevated ferritin, low TSAT, elevated hsCRP. Driven by hepcidin-mediated iron sequestration; treat the underlying inflammation, not the iron.
- Hereditary hemochromatosis-spectrum: TSAT above 45%, ferritin above 300 ng/mL, frequently elevated liver enzymes, often family history. Warrants HFE genetic testing and hematology referral.
- Wilson's disease (rare opposite syndrome): low total serum copper, very low ceruloplasmin (often under 10 mg/dL), high non-ceruloplasmin copper, elevated 24-hour urine copper, hepatic or neuropsychiatric symptoms. Warrants hepatology referral and ATP7B genetic testing; the RCP approach is contraindicated.
- Zinc-copper displacement: elevated zinc-to-copper ratio on HTMA, low serum copper and ceruloplasmin, often history of long-term zinc supplementation or chronic denture-cream exposure (older zinc-containing formulations). Reverses with cessation of zinc supplementation and copper repletion.
- Postmenopausal iron accumulation: in women, ferritin trending upward across postmenopausal years as menstrual iron losses cease; baseline ferritin in the 60s often climbs into the 150s+ over a decade. Therapeutic phlebotomy is highly effective.
Cautions and Limitations
- HTMA methodology variability: HTMA results depend on sample preparation (washed vs. unwashed hair), instrumentation (ICP-MS vs. older ICP-OES or AAS), and laboratory technique. Two HTMAs from different labs on the same patient may not agree closely on absolute values. Pick one lab and use it consistently for trend analysis.
- External hair contamination: hair color treatments, bleaching, swimming pool chlorine and copper, and certain shampoos can artifactually elevate or suppress hair mineral values. Document recent treatments and avoid HTMA in the 4-6 weeks after major hair processing.
- Ceruloplasmin assay variability: the immunoassay measures total protein, not enzymatic activity. A patient with apoceruloplasmin (the copper-free protein) will have a normal immunoassay value despite zero functional activity. The ceruloplasmin oxidase activity assay is the definitive test when there is clinical-lab discordance.
- Acute illness window: do not interpret the panel during or within 2-4 weeks after acute infection, surgery, vaccination, or significant injury. Acute-phase reactant elevation (ferritin, ceruloplasmin, hsCRP) will distort the picture.
- Pregnancy: serum copper and ceruloplasmin rise substantially in pregnancy as a normal physiological adaptation. Reference ranges and RCP targets developed in non-pregnant adults do not apply. The RCP framework is generally not adopted during active pregnancy.
- Estrogen exposure: oral contraceptives and hormone replacement therapy elevate ceruloplasmin and serum copper. Note hormonal status when interpreting.
- Direct-to-consumer testing limitations: while convenient, DTC labs typically do not include physician interpretation or follow-up. Pair DTC testing with a functional medicine practitioner who can integrate the panel with clinical context.
- Insurance coverage: U.S. insurance typically covers conventional serum components when ordered by a physician for an appropriate indication (fatigue, anemia, suspected hemochromatosis); HTMA, RBP4, magnesium RBC, and ceruloplasmin oxidase activity are often not covered and require cash payment.
- Not a diagnostic substitute: the RCP panel is a functional metabolic assessment, not a diagnostic test for any specific disease. Patients with red-flag symptoms (unexplained weight loss, GI bleeding, jaundice, severe fatigue with anemia) require conventional medical workup in parallel.
Key Research Papers
- Vashchenko G, MacGillivray RT (2013). Multi-copper oxidases and human iron metabolism. Nutrients 5(7):2289-2313. — PMID: 23807651
- Hellman NE, Gitlin JD (2002). Ceruloplasmin metabolism and function. Annu Rev Nutr 22:439-458. — PMID: 12055353
- Harris ZL, Klomp LW, Gitlin JD (1998). Aceruloplasminemia: an inherited neurodegenerative disease with impairment of iron homeostasis. Am J Clin Nutr 67(5 Suppl):972S-977S. — PMID: 9587138
- Walshe JM (2003). Wilson's disease: the importance of measuring serum caeruloplasmin non-immunologically. Ann Clin Biochem 40(Pt 2):115-121. — Search PubMed
- Cook JD, Flowers CH, Skikne BS (2003). The quantitative assessment of body iron. Blood 101(9):3359-3364. — PMID: 12521995
- Daru J, Colman K, Stanworth SJ, et al. (2017). Serum ferritin as an indicator of iron status: what do we need to know? Am J Clin Nutr 106(Suppl 6):1634S-1639S. — PMID: 29070560
- Kell DB, Pretorius E (2014). Serum ferritin is an important inflammatory disease marker, as it is mainly a leakage product from damaged cells. Metallomics 6(4):748-773. — PMID: 24549403
- Wilson JF, Hayes RB, Pearson JC, Tomatis L (1986). Hair mineral analysis: a review of procedures and applications. Sci Total Environ 54:1-23. — Search PubMed
- Pasricha SR, Tye-Din J, Muckenthaler MU, Swinkels DW (2021). Iron deficiency. Lancet 397(10270):233-248. — Search PubMed
- Adams PC, Reboussin DM, Barton JC, et al. (2005). Hemochromatosis and iron-overload screening in a racially diverse population. N Engl J Med 352(17):1769-1778. — PMID: 15858186
- Beutler E, Felitti VJ, Koziol JA, Ho NJ, Gelbart T (2002). Penetrance of 845G→A (C282Y) HFE hereditary haemochromatosis mutation in the USA. Lancet 359(9302):211-218. — PMID: 11812557
- Workinger JL, Doyle RP, Bortz J (2018). Challenges in the diagnosis of magnesium status. Nutrients 10(9):1202. — PMID: 30200431
- Costello RB, Elin RJ, Rosanoff A, et al. (2016). Perspective: the case for an evidence-based reference interval for serum magnesium: the time has come. Adv Nutr 7(6):977-993. — PMID: 28140318
- Olson JA (1984). Serum levels of vitamin A and carotenoids as reflectors of nutritional status. J Natl Cancer Inst 73(6):1439-1444. — Search PubMed
PubMed Topic Searches
- PubMed: Ceruloplasmin oxidase activity assay
- PubMed: Hair tissue mineral analysis (HTMA)
- PubMed: Transferrin saturation interpretation
- PubMed: Ferritin and acute-phase confound
- PubMed: RBC magnesium clinical utility
- PubMed: Retinol-binding protein 4
- PubMed: Non-ceruloplasmin-bound (free) copper
- PubMed: Therapeutic phlebotomy for iron reduction
Connections
- Morley Robbins Hub
- Benefits Deep Dive
- Copper-Iron Imbalance
- Whole Food Copper Sources
- Magnesium Foundation
- Iron Overload Hidden Toxicity
- Ceruloplasmin & Bioavailable Copper
- Copper-Iron Dysregulation
- Root Cause Protocol
- Copper
- Iron
- Magnesium
- Vitamin A
- Organ Meats (Beef Liver)
- Lab Tests
- All Remedies