Time-Restricted Eating 16:8 — The Daily Metabolic Switch
Time-restricted eating (TRE) compresses all daily food intake into a fixed window — most commonly 8 hours of feeding, 16 hours of fasting — without prescribing what or how much to eat within the window. The protocol's scientific home is the Satchin Panda lab at the Salk Institute, where mouse studies starting in 2012 (Hatori et al., Cell Metabolism) established that mice eating the same high-fat diet across the same total calories but confined to an 8-hour window were dramatically protected from obesity, fatty liver, hyperinsulinemia, and inflammation compared to mice with ad-libitum 24-hour access. The mechanism is not calorie restriction. It is circadian alignment of feeding to the metabolic active phase and the daily metabolic switch from glucose to ketone fuel that becomes possible only when the eating window ends well before sleep.
Interactive Visualization Fat Burning & Ketosis — what actually happens Follow a fatty acid out of a fat cell to the mitochondrial gate and find it padlocked by insulin. Drop the carbs, open CPT1, and watch the liver start making ketones. Launch →
Table of Contents
- What 16:8 Actually Means in Practice
- The Circadian Biology Behind TRE
- The Daily Metabolic Switch (Glucose to Ketones)
- Insulin and Glucose Effects
- Weight Loss Without Calorie Counting
- Practical Implementation
- Early vs Late Eating Window — Which Wins?
- What Breaks a Fast (and What Doesn't)
- Cautions and Who Should Not Do TRE
- Key Research Papers
- Connections
- Featured Videos
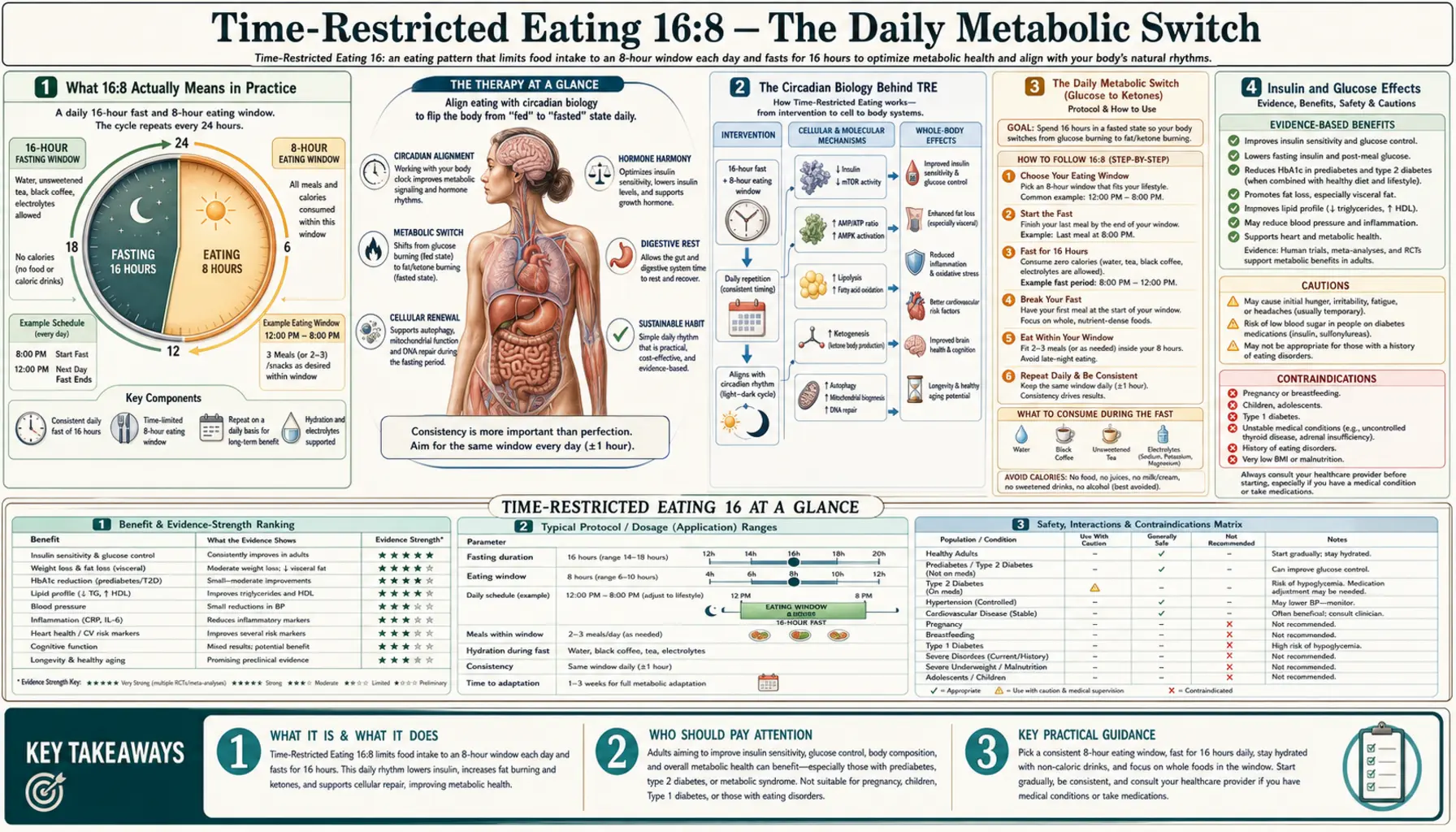
What 16:8 Actually Means in Practice
The 16:8 ratio refers to hours per day — 16 hours of complete food abstinence (water, plain tea, and black coffee are allowed) paired with an 8-hour eating window during which a person eats normally, in whatever number of meals they prefer. The most common implementations:
- Skip-breakfast pattern — eat from noon to 8 PM, fast from 8 PM until noon the next day. This is the most popular pattern in adult practitioners because it preserves social dinner.
- Skip-dinner pattern (early TRF) — eat from 7 AM to 3 PM, fast from 3 PM through the rest of the day and overnight. This is the version that produces the strongest metabolic effects in research (Sutton 2018, Jamshed 2019), because evening eating disrupts the circadian phase more than morning eating.
- Mid-day window — eat from 10 AM to 6 PM. A workable compromise that preserves a light breakfast and a moderate dinner.
Variants closer to 14:10 or 12:12 are easier and produce real but smaller effects. Variants tighter than 16:8 — 18:6, 20:4 (the "Warrior Diet"), or one-meal-a-day (OMAD) — push toward the territory covered on the extended-fasts page. For most adults beginning intermittent fasting, 16:8 is the entry point that balances meaningful metabolic effect with sustainability.
The Circadian Biology Behind TRE
Every cell in the body keeps time. The suprachiasmatic nucleus (SCN) in the hypothalamus is the master clock, entrained primarily by light, but peripheral clocks in the liver, pancreas, gut, muscle, and adipose tissue are entrained primarily by feeding. The peripheral clocks regulate the expression of approximately 10-15% of the transcriptome in a circadian rhythm — metabolic enzymes, hormone receptors, transporters, and inflammatory mediators all rise and fall over the 24-hour cycle.
The default arrangement, baked in by evolution for diurnal mammals: insulin sensitivity, glucose tolerance, and digestive enzyme secretion peak during the active phase (daylight) and are suppressed during the rest phase (night). A 600-calorie meal eaten at 8 AM produces a smaller blood glucose excursion than the same meal eaten at 8 PM, even in the same person on the same day. Beta cells release less insulin in the evening. Gastric emptying slows in the evening. The liver's gluconeogenic machinery ramps up in the early morning hours to maintain fasting glucose during sleep (the dawn phenomenon).
Modern eating patterns, with the heaviest meal typically eaten in the evening and frequent snacking from breakfast through bedtime, are circadian misaligned. The peripheral clocks of the liver and pancreas are told one phase by feeding signals while the SCN sees a different phase from light. This misalignment is associated with metabolic syndrome features even in the absence of overall calorie excess — shift workers have approximately 23% higher rates of metabolic syndrome and type 2 diabetes than day workers, controlling for diet quality and calories.
Time-restricted eating, especially when the window is placed in the metabolic active phase (early TRF), realigns the peripheral clocks with the SCN. The peripheral signal — food — arrives in the daytime, matching the master clock's daytime signal — light. The result is improved glucose tolerance, improved insulin sensitivity, lower nocturnal blood pressure, and improved sleep quality.
The Daily Metabolic Switch (Glucose to Ketones)
The 16-hour fast of the 16:8 protocol is engineered specifically to trigger the daily metabolic switch from glucose to ketone fuel. After the last meal of the eating window, the body draws on circulating glucose for the first 4-6 hours. Hepatic glycogen stores are then mobilized for the next 6-10 hours. By approximately hour 12-14 of fasting, hepatic glycogen is largely depleted in a lean active person. The liver begins beta-oxidation of free fatty acids mobilized from adipose tissue, producing acetyl-CoA in excess of TCA-cycle demand, which is exported as ketone bodies (beta-hydroxybutyrate, acetoacetate, acetone).
BHB is more than a fuel. It is also a signaling molecule:
- Class I HDAC inhibitor — BHB at physiological fasting concentrations (1-2 mmol/L) inhibits class I histone deacetylases, altering the expression of genes involved in oxidative stress resistance (FOXO3, MT2, catalase)
- NLRP3 inflammasome blockade — Youm et al. (Nature Medicine 2015) showed BHB suppresses NLRP3 inflammasome activation, with downstream reductions in IL-1beta and IL-18, contributing to fasting's anti-inflammatory effect
- Preferred brain fuel under fasting — BHB crosses the blood-brain barrier and supplies up to 60-70% of brain energy during prolonged fasting, providing a more efficient ATP yield per oxygen than glucose
- BDNF induction — BHB upregulates brain-derived neurotrophic factor in the hippocampus, the proposed mechanism for the cognitive clarity many TRE practitioners report
A 16-hour fast typically pushes BHB to 0.3-0.6 mmol/L in a lean active practitioner — the threshold of mild nutritional ketosis. Higher BHB requires longer fasting or carbohydrate restriction. For the deeper ketosis of multi-day fasting, see the extended-fasts page.
Insulin and Glucose Effects
The most reproducible metabolic effect of 16:8 TRE in clinical trials is improvement in insulin sensitivity, often independent of weight loss. Sutton et al. 2018 randomized prediabetic men to early time-restricted feeding (6-hour eating window ending before 3 PM) versus a 12-hour control window, with food intake and weight held equal. The early-TRF group showed improved insulin sensitivity (as measured by ogtt-derived Matsuda index), reduced fasting insulin, lower blood pressure, and reduced oxidative stress markers — all without weight change. This is significant because it isolates the time-of-eating effect from the calorie-restriction effect.
Wilkinson et al. (Cell Metabolism 2020) extended the work to metabolic syndrome patients with a 10-hour eating window for 12 weeks. Improvements: 3.3 kg weight loss, 4 cm waist reduction, atherogenic lipid panel improvements (LDL, non-HDL), HbA1c reduction in those with elevated baseline, and blood pressure reductions of 5/4 mmHg.
The mechanism is twofold: lengthening the fasting period allows insulin levels to fall to nadir for longer periods each day, which restores insulin receptor sensitivity, and the alignment of feeding to the high-insulin-sensitivity daytime phase produces smaller glucose excursions per gram of carbohydrate consumed. Both effects compound — insulin sensitivity improves, which means smaller insulin response to subsequent meals, which means less fat storage and easier mobilization of adipose during the fasting window.
For patients with established type 2 diabetes or insulin resistance, 16:8 TRE is one of the most consistently effective lifestyle interventions in the modern literature. The caveat: patients on insulin or insulin secretagogues (sulfonylureas, meglitinides) must have their medications adjusted by their physician before starting, because the combination of fasting and these drugs can produce dangerous hypoglycemia.
Weight Loss Without Calorie Counting
The early enthusiasm around TRE was that it would produce weight loss as effectively as conventional calorie restriction, but without the cognitive load of tracking and measuring portions. The reality is more nuanced.
In multiple trials including the TREAT study (Lowe et al., JAMA Internal Medicine 2020), 16:8 TRE without explicit calorie restriction produced modest weight loss of 1-3% of body weight over 8-12 weeks — less than the 5-7% typically achieved with explicit calorie restriction in equivalent timeframes. The TREAT study notably found that some of the weight lost was lean mass rather than fat, raising concern that TRE alone is insufficient for body recomposition.
However, when 16:8 is paired with resistance training and adequate protein intake (1.6 g/kg/day or higher) within the eating window, the lean-mass loss is prevented and body recomposition (fat loss with lean mass preservation) is achievable. The Cienfuegos et al. 4-hour versus 6-hour TRE comparison found greater weight loss with tighter windows but similar fat-vs-lean ratio.
The practical bottom line: TRE produces weight loss for most people not because it has a special metabolic magic, but because spontaneous calorie intake drops when the eating window is compressed. The average TRE practitioner eats roughly 300-500 fewer calories per day than the same person ad libitum. The benefit over calorie counting is the simplicity — one decision (when to eat) rather than thousands (how much of each food). For the subset of people who can sustain that simplicity, TRE is a sustainable weight-management strategy.
Practical Implementation
- Week 1: 12:12 — eat from 7 AM to 7 PM, fast 7 PM to 7 AM. Most adults already do something close to this. Establishes the baseline.
- Week 2-3: 14:10 — tighten to a 10-hour window. E.g. eat 9 AM to 7 PM. The morning fast is the harder part for most.
- Week 4 onward: 16:8 — either skip breakfast (eat noon to 8 PM) or skip dinner (eat 7 AM to 3 PM). The early-TRF version is more metabolically effective but socially harder. The late-TRF version is easier socially but loses some of the circadian benefit.
- During the fasting window — water (target 2-3 L/day), plain black coffee, plain tea (green, black, herbal), and a pinch of mineral salt or electrolyte mix are all acceptable. Anything with calories breaks the fast.
- Within the eating window — eat real food. The metabolic benefits of TRE are blunted if the eating window is filled with ultra-processed snacks and sweetened beverages. Prioritize protein (palm-sized portion at each meal), non-starchy vegetables, healthy fats, and moderate amounts of nutrient-dense carbohydrates (sweet potato, berries, legumes).
- Hydration discipline — many of the symptoms novices attribute to "low blood sugar" during the fasting window are actually dehydration or sodium deficiency. A pinch of mineral salt in morning water often eliminates the headache, irritability, and lightheadedness that beginners report.
Early vs Late Eating Window — Which Wins?
The clinical research is essentially unanimous on this question: when measurable metabolic outcomes are compared, an early eating window (e.g. 7 AM to 3 PM) outperforms a late eating window (e.g. noon to 8 PM) on glucose tolerance, insulin sensitivity, blood pressure, and 24-hour mean glucose, even when total calories and total fasting time are identical.
The mechanism is the circadian alignment discussed above. Insulin sensitivity peaks in the morning. Beta cells respond most efficiently to glucose loads in the morning. The peripheral metabolic clocks expect food in the active phase, not the rest phase. When the eating window is moved earlier, the metabolic machinery operates in its high-efficiency configuration. When it is moved later, the same calories produce larger glucose excursions, more insulin release per gram of carbohydrate, and disrupted sleep architecture from late-night digestion.
The practical compromise: very few adults can sustain a 7 AM to 3 PM eating window long-term because it conflicts with social dinner culture. A mid-day window (10 AM to 6 PM) captures most of the metabolic benefit while preserving the ability to have dinner with family on most evenings. The hard rule that seems to matter most: no calories in the 3 hours before sleep. The last meal should be finished at least 3 hours before bedtime, ideally more.
What Breaks a Fast (and What Doesn't)
"Does X break my fast?" is the most common question novice fasters ask. The answer depends on which benefit of fasting matters most to the person asking.
- Pure water — does not break a fast on any definition.
- Plain black coffee or plain tea — negligible calories, does not measurably impair the metabolic switch, autophagy, or insulin response. Acceptable on all definitions.
- Bone broth (1 cup) — 30-50 calories with protein and electrolytes. Will modestly elevate insulin and mTOR, but the electrolytes can be a net positive for those with fasting-related fatigue or muscle cramps. Considered "fast-compatible" by Buchinger Wilhelmi clinic but not by purist autophagy frameworks.
- Pure MCT oil or unsweetened heavy cream (small amount) — fat alone produces minimal insulin response and keeps the body in fasted-state metabolism. Some practitioners add 1 tbsp MCT or 1 tbsp heavy cream to morning coffee with negligible metabolic impact — "fat fast" or "bulletproof" approach. Strict autophagy targets are partially blunted.
- Artificial sweeteners — the data are mixed. Aspartame and sucralose may produce small insulin responses in some individuals. Stevia and erythritol appear minimally impactful. If pure water is tolerable, prefer it.
- Apple cider vinegar (1 tsp in water) — negligible calories, may modestly improve fasted-state insulin sensitivity. Considered fast-compatible.
- Anything with protein, sugar, or significant carbohydrate — breaks the fast in any meaningful sense. Yes, this includes "just a bite," milk in coffee, or "just a couple almonds."
Cautions and Who Should Not Do TRE
- Pregnancy and lactation — women who are pregnant or breastfeeding should not practice intermittent fasting. The fetus and the infant require steady glucose and nutrient delivery.
- Children and adolescents — growing children should not fast intermittently. Their daily caloric and nutrient requirements are too high to compress into 6-8 hours.
- Type 1 diabetes — never modify a fasting protocol on top of insulin therapy without close endocrinologist supervision. Risk of severe hypoglycemia.
- Type 2 diabetes on insulin or sulfonylureas — medication doses must be reduced by a physician before starting TRE to avoid hypoglycemia. TRE can be very effective in T2D but the medication interaction is the risk.
- History of eating disorders — particularly anorexia nervosa, bulimia, and binge eating disorder. Structured restriction patterns can trigger relapse.
- Underweight or recently ill — BMI < 18.5 is a contraindication. Recovery from major illness or surgery is not the time to start TRE.
- Elderly with sarcopenia — protein intake distribution matters more than total in older adults trying to preserve muscle. Compressing protein into a 6-hour window may not provide enough leucine pulses to maintain mTOR-dependent muscle protein synthesis.
- Heavy athletic training — endurance athletes during peak training blocks need fueling windows that may conflict with strict TRE. Most can do TRE in off-season or base-building phases but should liberalize during high-volume periods.
Key Research Papers
- Hatori M et al. (2012). Time-restricted feeding without reducing caloric intake prevents metabolic diseases in mice fed a high-fat diet. Cell Metabolism. — PubMed
- Sutton EF et al. (2018). Early time-restricted feeding improves insulin sensitivity, blood pressure, and oxidative stress even without weight loss in men with prediabetes. Cell Metabolism. — PubMed
- Wilkinson MJ et al. (2020). Ten-hour time-restricted eating reduces weight, blood pressure, and atherogenic lipids in patients with metabolic syndrome. Cell Metabolism. — PubMed
- Lowe DA et al. (2020). Effects of time-restricted eating on weight loss and other metabolic parameters in women and men with overweight and obesity (TREAT study). JAMA Internal Medicine. — PubMed
- Gabel K et al. (2018). Effects of 8-hour time restricted feeding on body weight and metabolic disease risk factors in obese adults. Nutrition and Healthy Aging. — PubMed
- Cienfuegos S et al. (2020). Effects of 4- and 6-h time-restricted feeding on weight and cardiometabolic health: a randomized controlled trial in adults with obesity. Cell Metabolism. — PubMed
- Jamshed H et al. (2019). Early time-restricted feeding improves 24-hour glucose levels and affects markers of the circadian clock, aging, and autophagy in humans. Nutrients. — PubMed
- Manoogian ENC, Panda S (2017). Circadian rhythms, time-restricted feeding, and healthy aging. Ageing Research Reviews. — PubMed
- de Cabo R, Mattson MP (2019). Effects of intermittent fasting on health, aging, and disease. NEJM. — PubMed
- Youm YH et al. (2015). The ketone metabolite beta-hydroxybutyrate blocks NLRP3 inflammasome-mediated inflammatory disease. Nature Medicine. — PubMed
- Patterson RE, Sears DD (2017). Metabolic effects of intermittent fasting. Annual Review of Nutrition. — PubMed
- Anton SD et al. (2018). Flipping the metabolic switch: understanding and applying the health benefits of fasting. Obesity. — PubMed
PubMed Topic Searches
- PubMed: Time-restricted eating 16:8
- PubMed: Early TRF and insulin
- PubMed: Circadian feeding and metabolic health
- PubMed: BHB ketosis signaling
- PubMed: TRE and metabolic syndrome
Connections
- Fat Burning & Ketosis — interactive animation
- Fasting Benefits Hub
- Fasting Overview
- Extended Fasts (24-72h)
- Autophagy & mTOR
- Refeeding Strategy
- Type 2 Diabetes
- Insulin Resistance
- Metabolic Syndrome
- Obesity
- Fatty Liver Disease
- Magnesium
- Potassium
- Sodium
- All Remedies
- Eggs (Window Protein)