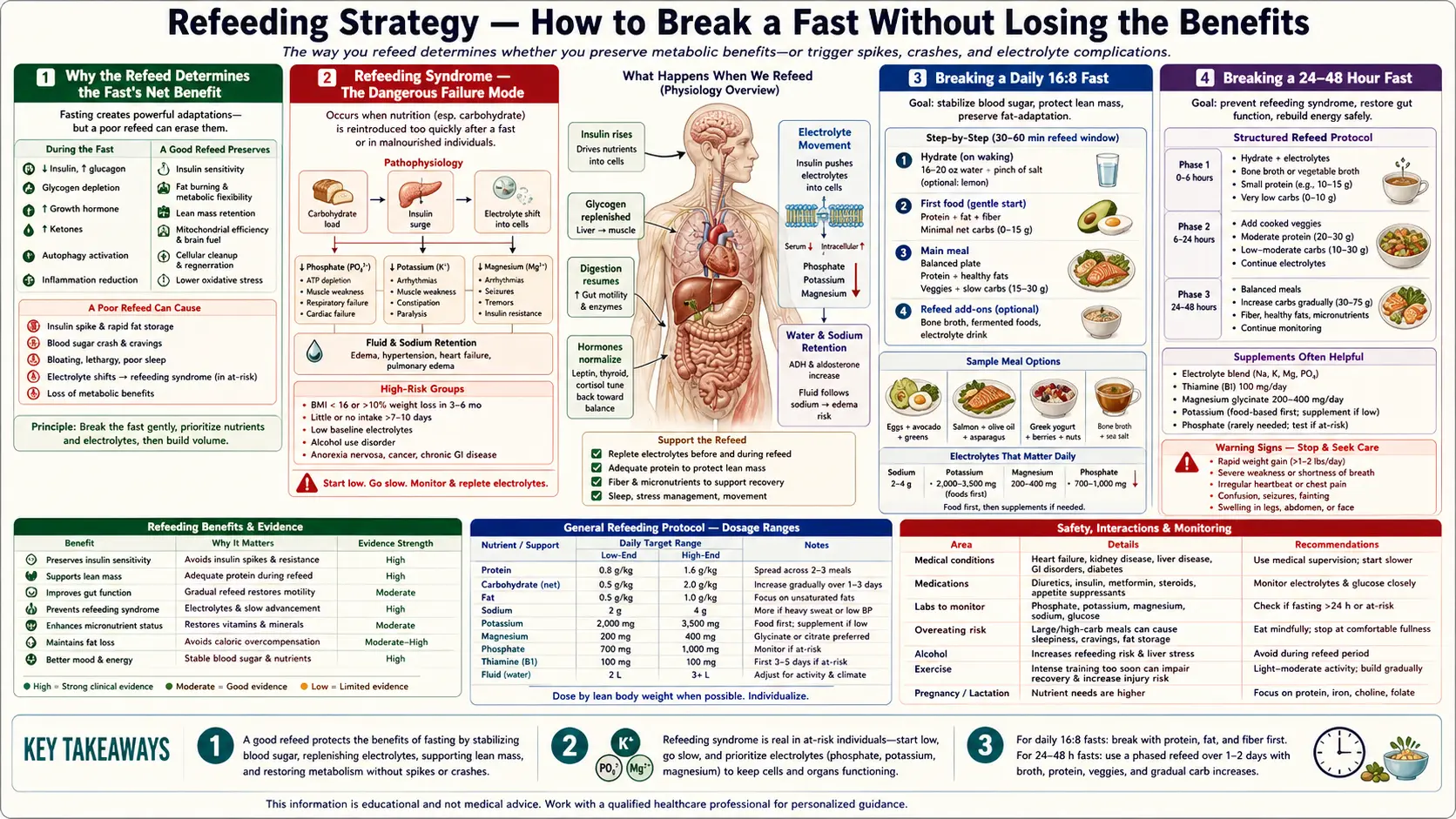
Refeeding Strategy — How to Break a Fast Without Losing the Benefits
The most-skipped chapter of fasting education is refeeding. Practitioners obsess over fasting protocols, BHB strips, and autophagy markers, then break a 72-hour fast with a pizza and wonder why they feel terrible. The refeed itself either preserves or destroys the metabolic benefits of the preceding fast — and in extended fasts of 5+ days, an improperly executed refeed can produce refeeding syndrome, a potentially fatal disorder of phosphorus, potassium, magnesium, and thiamine homeostasis first recognized in liberated WWII concentration-camp survivors who died from cardiac and respiratory failure within days of being given high-carbohydrate meals. This page covers the bone-broth-then-fat-then-protein-then-carbs sequence, the electrolyte and thiamine repletion that prevents refeeding syndrome, the role of L-glutamine and probiotics in gut-mucosa recovery, and the discipline of not overcompensating after a successful fast.
Interactive Visualization Fat Burning & Ketosis — what actually happens Follow a fatty acid out of a fat cell to the mitochondrial gate and find it padlocked by insulin. Drop the carbs, open CPT1, and watch the liver start making ketones. Launch →
Table of Contents
- Why the Refeed Determines the Fast's Net Benefit
- Refeeding Syndrome — The Dangerous Failure Mode
- Breaking a Daily 16:8 Fast
- Breaking a 24-48 Hour Fast
- Breaking a 72-Hour or Longer Fast
- Electrolyte and Thiamine Repletion
- L-Glutamine, Probiotics, and Gut-Mucosa Recovery
- Avoiding the Post-Fast Binge
- Warning Signs That Demand Medical Attention
- Key Research Papers
- Connections
- Featured Videos
Why the Refeed Determines the Fast's Net Benefit
The fast itself produces metabolic changes — insulin suppression, ketosis, growth hormone elevation, autophagy induction, immune cell turnover. The refeed is the cellular signal to switch back to growth-and-synthesis mode. If executed well, the refeed harnesses the heightened insulin sensitivity, the elevated growth hormone, and the cleared cellular landscape to support a wave of efficient nutrient uptake and tissue rebuilding. If executed poorly, the refeed produces dangerous blood-glucose spikes (because the body's glucose-handling machinery has been quiescent for days), violent insulin surges with reactive hypoglycemia, GI distress (because gut digestive enzymes have downregulated), and electrolyte derangement.
The general principle: the longer the fast, the slower and more deliberate the refeed must be. A 16-hour daily fast can be broken with a normal meal. A 24-48 hour fast benefits from a few hours of gentle reintroduction. A 72-hour fast requires a structured 24-hour refeed protocol. A 5-day or longer fast requires medical supervision and may require 2-3 days of progressive refeeding before normal eating resumes.
The other principle: the refeed is when the gains are consolidated. Practitioners who treat the refeed as a reward and consume large quantities of refined carbohydrates and processed food undo much of the fast's benefit within hours — the insulin surge, mTOR reactivation, and inflammatory response of an ultra-processed refeed can overshoot the fasted baseline and produce a net-negative outcome. The refeed should be nourishing food, deliberately paced, and aligned with the post-fast metabolic state.
Refeeding Syndrome — The Dangerous Failure Mode
Refeeding syndrome is the cluster of metabolic disturbances that can follow rapid reintroduction of nutrition in a chronically undernourished patient. It was first systematically described in the 1940s in liberated WWII prisoners of war and concentration-camp survivors who died unexpectedly within days of being fed by well-meaning relief workers. Modern recognition came largely through the parenteral nutrition literature of the 1970s-80s.
The mechanism: during prolonged fasting or starvation, intracellular stores of phosphorus, potassium, magnesium, and water-soluble vitamins (especially thiamine) become depleted, but serum levels often appear normal because of slow renal clearance and intracellular-to-extracellular redistribution. When carbohydrate is reintroduced, the resulting insulin surge drives a sudden intracellular shift of phosphorus, potassium, and magnesium — producing rapid and severe drops in serum levels of all three within hours. Simultaneously, thiamine demand rises sharply because thiamine is the cofactor for pyruvate dehydrogenase and is needed for the resumption of carbohydrate metabolism.
The clinical syndrome:
- Hypophosphatemia — the most dangerous component. Severe hypophosphatemia (< 1.0 mg/dL) produces respiratory muscle weakness (because ATP synthesis requires phosphorus), cardiac dysfunction, rhabdomyolysis, hemolysis, and seizures.
- Hypokalemia — cardiac arrhythmias, muscle weakness, ileus.
- Hypomagnesemia — arrhythmias, tetany, seizures.
- Thiamine deficiency — Wernicke encephalopathy (confusion, ataxia, ophthalmoplegia) or wet beriberi (high-output cardiac failure).
- Volume overload — refeeding-induced sodium retention can produce pulmonary edema in patients with marginal cardiac function.
The classic high-risk population is chronically malnourished hospitalized patients receiving aggressive enteral or parenteral nutrition, not healthy intermittent-fasting practitioners. But a 7-day water-only fast in a person who was already lean to begin with can produce a milder version of the same phenomenon. The general rule: fasts beyond 5 days, fasts undertaken by underweight or chronically ill people, and any extended fast where the refeed begins with a large carbohydrate load, all increase refeeding-syndrome risk.
The prevention strategy is straightforward: start the refeed with bone broth and a small amount of fat-and-protein, not carbohydrate. Reintroduce carbohydrate gradually over 24-48 hours. Supplement thiamine 100-300 mg/day for the first several days. Monitor for the warning signs (see below). For fasts beyond 5 days, baseline electrolytes (phosphorus, potassium, magnesium) should be checked before refeeding begins and rechecked at 12-24 hour intervals during the refeed.
Breaking a Daily 16:8 Fast
Daily TRE fasts of 16-18 hours do not produce a refeeding-syndrome risk in healthy adults. The first meal of the eating window can be a normal balanced meal — protein, fat, vegetables, moderate complex carbohydrates — without special precaution.
However, there are still better and worse choices:
- Best first-meal pattern — protein-led, with healthy fat and non-starchy vegetables. Examples: 3-egg omelet with spinach and avocado; grilled salmon with a salad; bone broth followed by a chicken breast and roasted vegetables. The protein-and-fat pattern produces a moderate, sustained insulin response.
- Worse first-meal pattern — carbohydrate-dominant, especially refined carbohydrate. A muffin, a bagel, a sweetened latte, or a bowl of cereal will produce a large blood-glucose excursion and reactive hypoglycemia within 2-3 hours because the fasted-state insulin sensitivity amplifies the glucose response.
- Hydration first — many TRE practitioners benefit from a glass of water with a pinch of mineral salt 15-30 minutes before the first meal, to rehydrate and pre-replete sodium lost during the overnight fast.
The discipline that produces sustained TRE benefit: the eating window contains real food — protein, vegetables, fruits, healthy fats — not a constant grazing pattern of snacks and sweetened beverages. Three meals in an 8-hour window with no snacking is metabolically superior to 5-6 small frequent feedings even at identical total calories, because each snack is its own mTOR-activating, insulin-secreting event.
Breaking a 24-48 Hour Fast
By 24 hours of fasting, gastric emptying has slowed, digestive enzyme secretion has downregulated, and the gut mucosa has reduced its turnover. A large meal at this point will sit in the stomach uncomfortably, may produce nausea, and often causes a violent reactive hypoglycemia event 2-3 hours later.
The structured 24-48 hour refeed protocol:
- Hour 0 (breaking the fast) — one cup of warm bone broth. Sip slowly over 15-20 minutes. The protein content is small (3-6 grams), the fat content is moderate, and the gelatin is gentle on the gut mucosa. Most importantly, the electrolytes (sodium, potassium, magnesium) replete the deficit accumulated during the fast.
- Hour 0.5-1 — if the broth is tolerated without nausea, add a small portion of healthy fat (1/2 avocado, 1 oz nuts, or 1 tbsp olive oil) and a small portion of protein (2-3 oz eggs, fish, or chicken).
- Hour 2-3 — the first "real" meal. Protein (4-6 oz), healthy fat (avocado, olive oil, butter), non-starchy vegetables (leafy greens, broccoli, asparagus). Still no significant carbohydrate.
- Hour 4-6 — if the first meal was well tolerated, a second meal can include modest amounts of starchy vegetables (sweet potato, squash) or fruit (berries). Avoid grains and refined carbohydrates for the first 24 hours of refeeding.
- Hour 8-24 — return to normal balanced eating. The goal for the first 24 hours after breaking the fast is to consume approximately 80% of normal caloric intake, with the deficit made up over the following day or two.
The reason for the broth-first protocol: it tests gut tolerance, replenishes electrolytes, and produces a smaller insulin spike than any solid food. The reason for the no-carbohydrate-first-meal rule: carbohydrate produces the largest insulin response, the largest blood-glucose excursion, and (because of the fasted-state hypersensitivity) the largest risk of reactive hypoglycemia.
Breaking a 72-Hour or Longer Fast
A 72-hour fast requires a more deliberate 24-hour refeed protocol, with explicit electrolyte and thiamine supplementation, and progressive caloric reintroduction.
- Day 1 of refeed — total intake ~25-40% of normal calories. Begin with bone broth and small portions of fat and protein. No grains, no sugar, no alcohol, no large meals. Supplement: 100-300 mg thiamine, 400 mg magnesium, 99 mg potassium, ensure adequate sodium intake.
- Day 2 of refeed — total intake ~50-70% of normal calories. Introduce starchy vegetables (sweet potato, squash, beets) in modest portions. Continue thiamine and electrolyte supplementation. Avoid grains and refined carbohydrate.
- Day 3 of refeed — total intake ~80-100% of normal calories. Can introduce whole grains in modest portions. Continue elevated thiamine intake for one more day.
- Day 4 onward — return to normal eating pattern. Many extended-fast practitioners maintain a slightly tighter daily eating window (e.g. resume 16:8 TRE) for the week following a 72-hour fast, to extend the metabolic flexibility gains.
For fasts of 5 days or longer, baseline serum chemistry (phosphorus, potassium, magnesium, calcium, thiamine if available) is recommended before refeeding begins, and repeat chemistry 12-24 hours into refeeding to detect early refeeding syndrome before symptoms emerge. This is the point at which medical supervision becomes prudent.
Electrolyte and Thiamine Repletion
- Sodium — 2-3 grams over the first day of refeeding (broth, soup, sea-salted vegetables). The natriuresis of fasting depletes sodium; the refeed should replete it deliberately.
- Potassium — 3-4 grams from food sources (avocado, spinach, sweet potato, salmon, mushrooms) over the first 24-48 hours. Supplemental potassium beyond 99 mg per pill is not OTC-available in the US for good reason — potassium has a narrow therapeutic window and supraphysiologic dosing can produce dangerous hyperkalemia. Food-based potassium is safer than supplemental.
- Magnesium — 300-500 mg supplementally (magnesium glycinate or citrate) plus food sources (dark leafy greens, pumpkin seeds, almonds, dark chocolate). Magnesium is the most commonly deficient mineral in fasting practitioners.
- Phosphorus — food sources (dairy, eggs, fish, nuts) are usually adequate; supplemental phosphorus is rarely needed for self-directed extended fasts up to 72 hours. For longer fasts or in patients with risk factors for refeeding syndrome, oral phosphorus supplements may be appropriate under medical guidance.
- Thiamine (B1) — 100-300 mg/day for 3-5 days after a fast longer than 48 hours. Thiamine is required for the resumption of carbohydrate metabolism (pyruvate dehydrogenase cofactor). The classic refeeding-syndrome complication of Wernicke encephalopathy is prevented by adequate thiamine. Oral thiamine HCl is cheap, well-tolerated, and there is essentially no toxicity risk at these doses.
- B-complex — a general B-complex multivitamin alongside the thiamine is reasonable insurance, since the other B vitamins (riboflavin, niacin, B6, folate, B12) are all cofactors for various aspects of carbohydrate, fat, and protein metabolism.
L-Glutamine, Probiotics, and Gut-Mucosa Recovery
The gut mucosa turns over every 3-5 days under fed conditions — one of the fastest-renewing tissues in the body. During a fast longer than 3 days, this turnover slows substantially, and the villus enterocytes that normally absorb nutrients may show measurable atrophy. The refeed is when the mucosa rebuilds.
Two interventions support efficient gut recovery during refeeding:
- L-Glutamine — the primary fuel of enterocytes (gut epithelial cells). 5-10 grams of L-glutamine powder dissolved in water, taken in the first 24-48 hours of refeeding, supports rapid enterocyte recovery. Glutamine is technically a non-essential amino acid, but during refeeding from extended fasting it becomes "conditionally essential" because the demand outstrips endogenous synthesis.
- Probiotics and fermented foods — the microbiome composition shifts during extended fasting (reduced bacterial diversity, shifts in dominant phyla). The refeed is the opportunity to deliberately seed beneficial species. Fermented foods (sauerkraut, kimchi, kefir, plain yogurt) during the refeed support recolonization. Multi-strain probiotic supplements are reasonable adjuncts.
- Bone broth gelatin — the gelatin in well-made bone broth provides glycine and proline, the substrates for collagen synthesis and gut-mucosa repair. This is one of the reasons bone broth is the traditional first food when breaking a fast across many cultures.
Many practitioners report that their digestive tolerance after a multi-day fast is dramatically improved — foods that previously caused bloating or discomfort suddenly are well-tolerated. This is partly the gut-mucosa renewal effect and partly the microbiome reset that the fasting-refeeding cycle produces.
Avoiding the Post-Fast Binge
The psychological challenge of the refeed is often underestimated. After 48-72 hours without food, the ghrelin-driven hunger and the cognitive anticipation of "deserved" food combine to produce an urge to consume large quantities of palatable food immediately upon breaking the fast. This urge undoes the fast's benefits in two distinct ways:
- Physiologically — the large carbohydrate load produces a massive insulin surge, reactivates mTOR with full force, suppresses autophagy, and produces inflammatory cytokine elevation. The fast's metabolic benefits are not just lost but actively reversed.
- Behaviorally — the binge reinforces the cognitive pattern of fasting-as-restriction-followed-by-reward, which is the same psychological pattern that drives disordered eating. Healthy fasting practice should feel like a tool, not a deprivation followed by indulgence.
The structural prevention strategies:
- Plan the refeed in advance — before starting the fast, decide what the first meal will be and have the ingredients on hand. The post-fast brain is in a poor state for nutritional decision-making.
- Eat in a calm environment — sit down, eat slowly, chew thoroughly. The vagal-tone-driven satiety signal takes 15-20 minutes to develop; rapid eating overshoots before satiety can register.
- Use the broth-first protocol — even when not strictly required (e.g. for shorter fasts), the broth pre-meal blunts the urge to overeat by providing immediate gastric distension and a small amount of nutrient signal.
- Pre-portion the first meal — serve a normal portion onto a plate; do not eat from family-style serving dishes where the absence of a defined portion size invites overshoot.
- Avoid alcohol on refeed day — alcohol after a fast hits much harder than usual (low glycogen, low body water, low blood pressure), produces dramatic insulin and glucose dysregulation, and impairs the post-fast judgment that prevents overeating.
Warning Signs That Demand Medical Attention
Most fasting refeeds proceed uneventfully. The following symptoms during or immediately after refeeding should prompt urgent medical evaluation:
- Confusion, altered mental status, or new neurological symptoms — possible Wernicke encephalopathy from thiamine deficiency, hypoglycemia, hyponatremia, or hypophosphatemia. Emergency room visit warranted.
- Difficulty breathing or sudden weakness — possible respiratory muscle weakness from severe hypophosphatemia. Emergency room visit warranted.
- Palpitations or new arrhythmia — possible electrolyte derangement (potassium, magnesium, or calcium). Urgent evaluation.
- Severe edema or sudden weight gain within 24-48 hours of refeeding — possible refeeding-induced fluid retention with risk of pulmonary edema. Medical evaluation.
- Severe abdominal pain — possible gallstone complication or pancreatitis. Medical evaluation.
- Severe headache or visual changes — possible severe electrolyte abnormality or hypertensive event. Medical evaluation.
- Persistent vomiting — risk of further electrolyte loss and dehydration. Medical evaluation if it does not resolve quickly.
The vast majority of fasting practitioners will never encounter any of these. But the prevalence of social-media fasting content has produced a population of self-directed extended fasters who do not recognize the warning signs of refeeding syndrome until they are in the emergency department. Knowing what to watch for is the cheapest form of insurance.
Key Research Papers
- Mehanna HM, Moledina J, Travis J (2008). Refeeding syndrome: what it is, and how to prevent and treat it. BMJ. — PubMed
- Crook MA, Hally V, Panteli JV (2001). The importance of the refeeding syndrome. Nutrition. — PubMed
- Stanga Z et al. (2008). Nutrition in clinical practice — the refeeding syndrome: illustrative cases and guidelines for prevention and treatment. European Journal of Clinical Nutrition. — PubMed
- Boateng AA et al. (2010). Refeeding syndrome: treatment considerations based on collective analysis of literature case reports. Nutrition. — PubMed
- Solomon SM, Kirby DF (1990). The refeeding syndrome: a review. JPEN. — PubMed
- Friedli N et al. (2017). Management and prevention of refeeding syndrome in medical inpatients: an evidence-based and consensus-supported algorithm. Nutrition. — PubMed
- NICE (UK National Institute for Health and Care Excellence) guideline on nutrition support — refeeding syndrome criteria. — PubMed
- Wilhelmi de Toledo F et al. (2013). Fasting therapy — an expert panel update of the 2002 consensus guidelines. Forschende Komplementärmedizin. — PubMed
- Wischmeyer PE (2008). Glutamine: role in critical illness and ongoing clinical trials. Current Opinion in Gastroenterology. — PubMed
- Wang Y et al. (2015). The role of glutamine and the gut microbiota. — PubMed
- Maughan RJ, Shirreffs SM, Watson P (2007). Exercise, heat, hydration and the brain. JACN. — PubMed
- Kerndt PR et al. (1982). Fasting: the history, pathophysiology and complications. Western Journal of Medicine. — PubMed
PubMed Topic Searches
- PubMed: Refeeding syndrome
- PubMed: Fasting electrolyte management
- PubMed: Thiamine deficiency and refeeding
- PubMed: L-Glutamine and gut mucosa
- PubMed: Fasting microbiome refeed
Connections
- Fat Burning & Ketosis — interactive animation
- Fasting Benefits Hub
- Fasting Overview
- Time-Restricted Eating 16:8
- Extended Fasts (24-72h)
- Autophagy & mTOR
- L-Glutamine (Gut Refeed)
- Bone Broth (Refeed Starter)
- Vitamin B1 (Thiamine)
- Magnesium
- Potassium
- Sodium
- Phosphorus
- Type 2 Diabetes
- All Remedies
- Eggs (Refeed Protein)