Berberine Dosing, Forms, and Cautions
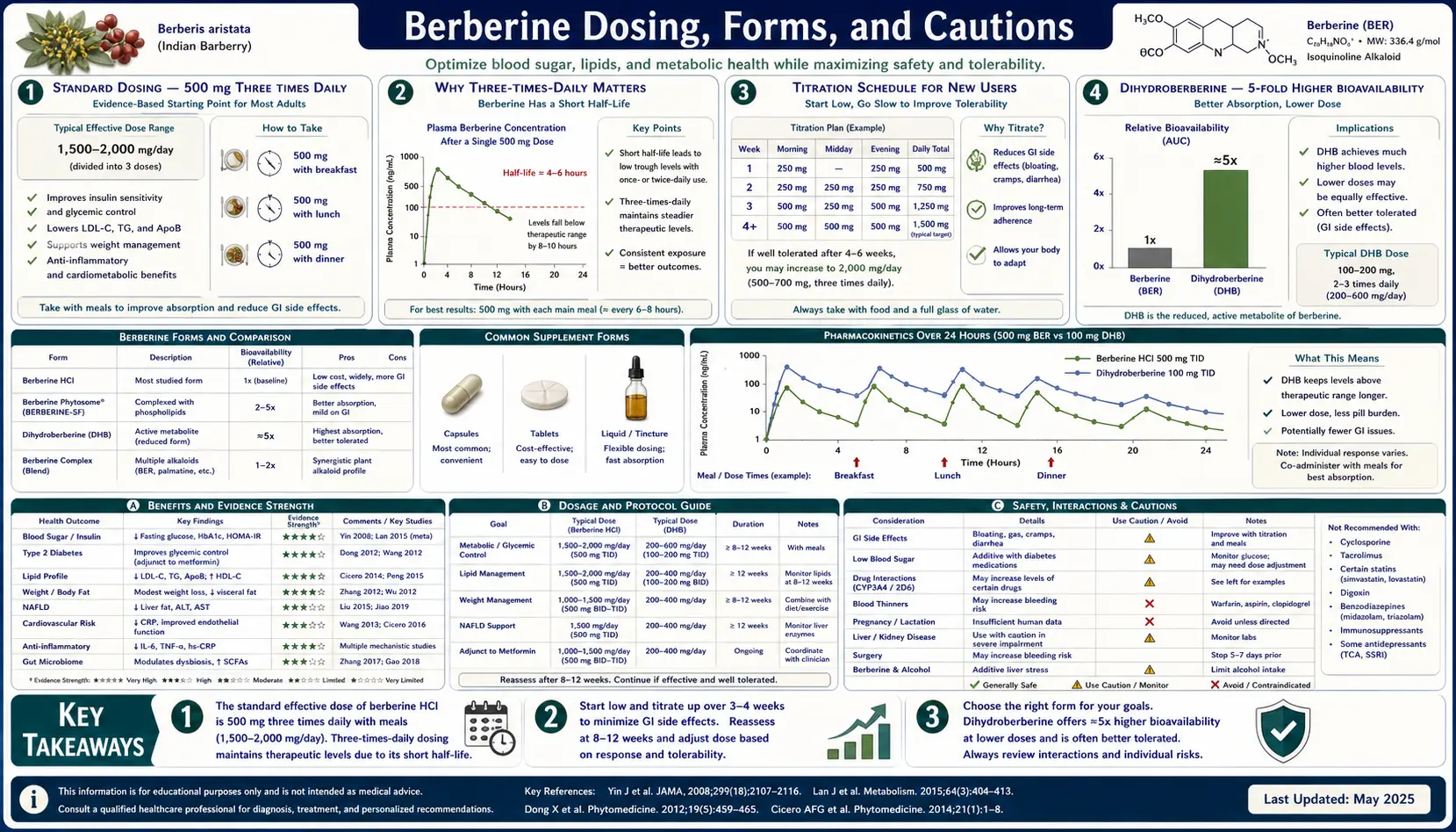
The standard berberine regimen used in essentially every positive clinical trial is 500 mg three times daily, taken with meals, for a total of 1,500 mg/day. This protocol is non-negotiable for matching the trial efficacy — once-daily dosing produces approximately half the clinical effect because of berberine's 4-hour half-life. Within this standard regimen, however, a number of practical questions matter: which berberine salt or formulation is preferable, when is dihydroberberine's 5-fold higher bioavailability worth the price premium, how to titrate to minimize GI symptoms, and most importantly which patients should NOT take berberine. The absolute contraindications are pregnancy (kernicterus risk in neonates from bilirubin displacement at the albumin binding site), breastfeeding (same mechanism, transferred via breast milk), and jaundiced infants of any age. The relative contraindications driven by CYP2D6 and CYP3A4 inhibition are numerous but manageable with proper drug-interaction review. This page walks through dosing, formulations, titration strategy, drug interactions, and the specific patient populations where berberine should be avoided or dose-modified.
Table of Contents
- Standard Dosing: 500 mg Three Times Daily
- Why Three-Times-Daily Matters
- Titration Schedule for New Users
- Dihydroberberine: 5-Fold Higher Bioavailability
- Berberine Phytosome and Silymarin-Paired Formulations
- Berberine Hydrochloride vs Sulfate vs Citrate
- GI Tolerance and Side Effects
- The Pregnancy Contraindication (Kernicterus Risk)
- CYP2D6 and CYP3A4 Drug Interactions
- Special Populations: CKD, Elderly, Liver Disease
- Duration of Therapy and Monitoring
- Key Research Papers
- Connections
- Featured Videos
Standard Dosing: 500 mg Three Times Daily
The cumulative trial evidence converges on a single regimen: 500 mg of berberine hydrochloride three times daily, with meals, for a total of 1,500 mg/day. This is the dose used in:
- The Yin 2008 metformin-comparison diabetes trial (defining the metabolic efficacy)
- The Kong 2004 Nature Medicine paper's clinical arm (defining the lipid efficacy)
- The Zhang 2008 JCEM metabolic syndrome trial
- The vast majority of subsequent confirmatory and mechanistic trials
Doses below 1,000 mg/day total typically produce only partial benefit. Doses above 2,000 mg/day total produce more GI side effects without commensurate additional benefit. The 1,500 mg/day in three divided doses is the demonstrated sweet spot.
Timing with meals matters for two reasons: (1) reduces the GI symptoms of fasting-state berberine administration, and (2) maximizes the postprandial alpha-glucosidase and DPP-4 inhibition effects covered on the Blood Sugar page. For patients who eat fewer than three meals per day, taking berberine alongside any food (even a small snack) is preferable to taking it on an empty stomach.
For patients taking berberine primarily for cholesterol (not glucose) effects, a slightly modified regimen of 500 mg twice daily is sometimes used — this is the Kong 2004 trial dose — and produces approximately 80% of the LDL-C reduction of the three-times-daily regimen. The trade-off is acceptable if compliance is the limiting factor.
Why Three-Times-Daily Matters
The pharmacokinetic basis for three-times-daily dosing is berberine's short plasma half-life. The terminal half-life of berberine in healthy human subjects is approximately 4 hours (some sources report 3-6 hours depending on assay method). With a 4-hour half-life:
- Once daily (1,500 mg single dose) — peak concentration is high but the molecule clears within ~16 hours, leaving 8 hours per day with sub-therapeutic concentration. Effective steady-state is poor.
- Twice daily (750 mg per dose) — produces better steady-state coverage but still has 12-hour gaps with declining concentration.
- Three times daily (500 mg per dose) — with 8-hour dose intervals, the concentration troughs are at approximately 25% of peak, and steady-state coverage is maintained throughout the day. This matches the experimental conditions of the positive trials.
- Four times daily (375 mg per dose) — slightly better steady-state coverage but the marginal benefit is small and compliance suffers.
The compliance challenge of three-times-daily dosing is real — many patients struggle to remember the noon dose. Practical strategies:
- Pill organizer with morning, noon, and evening compartments
- Phone alarm specifically for the noon dose
- Linking the noon dose to a daily ritual (immediately after lunch, before afternoon coffee)
- For patients who cannot manage three doses per day, dihydroberberine at twice-daily dosing (covered below) is a reasonable alternative with comparable steady-state coverage
Titration Schedule for New Users
Approximately 20-30% of new berberine users experience meaningful GI symptoms in the first 1-2 weeks — primarily diarrhea, cramping, bloating, and occasionally constipation (some patients oscillate between the two as the gut microbiome remodels). These symptoms typically self-resolve within 2-4 weeks as the microbiome reaches a new equilibrium, but the initial intolerance is the principal reason new users discontinue.
A graduated titration substantially reduces the dropout rate:
- Week 1 — 500 mg once daily with dinner. Assess GI tolerance. If well tolerated, proceed.
- Week 2 — 500 mg twice daily (breakfast and dinner). Continue monitoring.
- Week 3 onward — 500 mg three times daily (breakfast, lunch, dinner). This is the steady-state regimen for ongoing use.
For unusually sensitive patients, an even slower titration may be needed:
- Week 1-2 — 250 mg once daily with dinner
- Week 3-4 — 500 mg once daily
- Week 5-6 — 500 mg twice daily
- Week 7 onward — 500 mg three times daily
250 mg capsules are commercially available; alternatively, opening a 500 mg capsule and splitting the contents (berberine is a yellow powder, not unstable, no special handling) accomplishes the same. The taste is intensely bitter, so consumption as a powder is unpleasant — capsule administration is strongly preferable.
For patients who still cannot tolerate berberine at full dose, dihydroberberine at 100-200 mg twice daily is typically better tolerated and provides comparable clinical effect (covered below).
Dihydroberberine: 5-Fold Higher Bioavailability
Dihydroberberine is the reduced form of berberine — with an additional hydrogen across the C7-C8 bond, converting the quaternary ammonium of berberine into the tertiary amine of dihydroberberine. Critically, this single chemical change dramatically improves oral absorption.
The Turner 2008 paper in Diabetes compared berberine and dihydroberberine pharmacokinetics in rats. Dihydroberberine produced:
- Plasma area under the curve (AUC) approximately 5-fold higher than equivalent oral berberine
- Higher tissue concentration in liver, muscle, and adipose — the AMPK-target tissues
- Greater glucose-lowering effect at equivalent oral doses in diabetic animal models
The clinical translation is that dihydroberberine 100-200 mg twice daily produces approximately the same systemic effect as berberine 500 mg three times daily, but with fewer GI side effects and a more convenient dosing schedule. The trade-offs:
- Cost — dihydroberberine is typically 2-3x the price per dose of standard berberine; the cost-per-clinical-effect is comparable but the per-bottle price is higher
- Less gut-microbiome effect — because more drug is absorbed, less remains in the lumen to remodel the microbiome. For patients whose principal indication is systemic (glucose, lipids), this is a non-issue. For patients whose principal indication is SIBO or other gut conditions, standard berberine is preferable because the gut-luminal action is what they need.
- Less long-term safety data — dihydroberberine has fewer human trials and a shorter track record than standard berberine
Practical recommendation: standard berberine 500 mg TID is the default for most patients. Dihydroberberine 200 mg BID is the right choice for patients who (a) cannot tolerate the GI effects of standard berberine even after careful titration, or (b) cannot adhere to a three-times-daily schedule, or (c) have a strong preference for higher systemic exposure.
Berberine Phytosome and Silymarin-Paired Formulations
Two formulation strategies seek to improve berberine's oral absorption without the chemistry change to dihydroberberine:
- Berberine phytosome — berberine complexed with phospholipids (typically phosphatidylcholine from soy or sunflower lecithin). The phospholipid carrier improves berberine's passage across the intestinal epithelium by enhancing membrane interaction. Indena's Berberine Phytosome formulation reports approximately 10-fold higher AUC than equivalent free berberine.
- Berberine plus silymarin (milk thistle extract) — silymarin inhibits intestinal P-glycoprotein, the efflux pump that pumps absorbed berberine back into the gut lumen. Co-administration of silymarin 100-200 mg with berberine doses produces approximately 2-3x higher berberine plasma concentrations. The Italian Berberis aristata standardized extract Berberol is formulated as berberine 588 mg + silymarin 105 mg per tablet.
For most patients, the standard berberine 500 mg TID regimen is sufficient and the enhanced-bioavailability formulations are not necessary. The principal use case for the enhanced formulations is patients who have demonstrated suboptimal response to standard berberine (poor HbA1c or lipid response despite full compliance), or patients with documented malabsorption (post-bariatric surgery, advanced Crohn's) where conventional oral absorption is impaired.
The Italian Berberol clinical trials (Derosa 2013, 2015) have demonstrated that berberine + silymarin produces glucose and lipid effects comparable to standard berberine at substantially lower berberine doses (typically 588 mg twice daily of the combination matches 1,500 mg/day of free berberine).
Berberine Hydrochloride vs Sulfate vs Citrate
Berberine in supplements is sold as one of several salt forms. The active berberine cation is the same; only the counter-ion differs. The salt form affects solubility, taste, and to a small extent absorption kinetics, but does not affect overall clinical efficacy.
- Berberine hydrochloride (BBR HCl) — the most common form, used in essentially all clinical trials. Yellow crystalline solid, modest water solubility, intensely bitter taste. The HCl salt is what is meant by "berberine 500 mg" on a supplement label unless specified otherwise.
- Berberine sulfate — older form, less commonly available now
- Berberine citrate — somewhat better water solubility than the HCl form, marketed in some products for purported faster onset
The practical recommendation is to use berberine hydrochloride because the clinical trial evidence is built on this form. The other salts are not problematic; the dose adjustment for equivalent berberine content can be calculated from the molecular weights (BBR HCl molecular weight 371.8; berberine free base 336.4; so 500 mg BBR HCl = 452 mg berberine free base).
Labeling practice varies by manufacturer. Some labels report the berberine HCl content (which is what was in the trials), some report the berberine free base equivalent. For trial-equivalent dosing, the goal is 1,500 mg/day of berberine HCl, which is approximately 1,355 mg/day of berberine free base.
GI Tolerance and Side Effects
The principal side effect profile of berberine, in roughly decreasing frequency:
- Diarrhea (10-20% in first 2 weeks, < 5% long-term) — mechanism: gut microbiome remodeling and direct intestinal motility effect. Typically transient and self-resolving.
- Abdominal cramping (5-10%) — mechanism: intestinal smooth muscle effect of high luminal berberine concentration
- Constipation (3-5%) — some patients experience this paradoxical effect, particularly during the microbiome transition period
- Bloating and flatulence (5-10%) — gas production by the remodeled microbiome
- Nausea (2-3%) — usually responds to taking with food
- Headache (1-2%) — uncommon, mechanism uncertain
- Hypoglycemia in patients also taking sulfonylureas or insulin — additive glucose-lowering effect; doses of those agents may need to be reduced when berberine is added
Serious adverse events are very rare. Long-term safety (years of continuous use) has not been formally studied in large cohorts, but the Italian Armolipid Plus combination has been used widely in primary care for over 15 years without alarming signals, and traditional Chinese use of berberine-containing plants (Huang Lian) over centuries has not produced documented chronic toxicity at culinary or therapeutic doses.
Drug-induced hepatotoxicity from berberine is rare but has been reported. Routine liver enzyme monitoring is reasonable for patients on long-term berberine, particularly when combined with other hepatically-cleared agents (red yeast rice, statins).
The Pregnancy Contraindication (Kernicterus Risk)
The single most important safety issue with berberine is the absolute contraindication in pregnancy and in breastfeeding. The mechanism is bilirubin displacement from serum albumin.
Background: bilirubin is a yellow breakdown product of heme that is bound to serum albumin during transport from the reticuloendothelial system to the liver for conjugation. In adults, the liver can handle conjugation easily. In newborns, particularly premature newborns, hepatic UGT1A1 (the enzyme that conjugates bilirubin) is immature and not yet at full capacity. Unconjugated bilirubin can cross the blood-brain barrier and deposit in the basal ganglia, producing the neurological syndrome called kernicterus — a permanent, devastating injury producing cerebral palsy, deafness, and cognitive impairment.
Several drugs displace bilirubin from albumin binding, freeing it to cross the blood-brain barrier. Sulfonamide antibiotics are the classic example (the original sulfonamide tragedy of the 1940s). Berberine also has this property — it competes with bilirubin for the same albumin binding site.
The teratogenic and neonatal risks:
- Berberine taken during pregnancy can cross the placenta and reach the fetal circulation, where the immature fetal liver and BBB create kernicterus risk
- Berberine taken during breastfeeding is transferred in breast milk and reaches the newborn, who is the highest-risk individual for kernicterus
- Berberine should not be given to any jaundiced infant regardless of age, and should be avoided in infants under one year as a precaution
This contraindication is non-negotiable. Patients of reproductive age should be specifically counseled to discontinue berberine if pregnancy is planned or detected, and to avoid berberine throughout breastfeeding. For women with PCOS who use berberine for fertility (where the use is for the trying-to-conceive period), berberine should be discontinued at the time of positive pregnancy test.
CYP2D6 and CYP3A4 Drug Interactions
Berberine is a moderately potent inhibitor of two major cytochrome P450 enzymes:
- CYP2D6 — metabolizes approximately 25% of commonly used drugs, including many antidepressants, antipsychotics, opioids, and beta-blockers
- CYP3A4 — metabolizes approximately 50% of commonly used drugs, including statins, calcium channel blockers, immunosuppressants, many antibiotics, and many antivirals
Drugs with potentially clinically meaningful interactions with berberine include:
- Cyclosporine (transplant immunosuppressant) — berberine increases cyclosporine plasma concentrations 1.5-2 fold. This interaction has been formally documented and can produce nephrotoxicity. The combination should be avoided or carefully monitored.
- Tacrolimus, sirolimus (other immunosuppressants) — same CYP3A4 mechanism, same caution
- Statins metabolized by CYP3A4 (atorvastatin, simvastatin, lovastatin) — berberine may modestly increase statin concentrations, potentially increasing rhabdomyolysis risk. The combination is widely used (and the Armolipid Plus combination is explicitly this) but liver enzymes and CK should be checked periodically.
- Calcium channel blockers (amlodipine, felodipine, verapamil) — potential for increased hypotensive effect
- Antidepressants metabolized by CYP2D6 (paroxetine, fluoxetine, venlafaxine, duloxetine) — potential for increased plasma concentrations and side effects
- Antipsychotics (risperidone, haloperidol, olanzapine) — same mechanism, same caution
- Beta-blockers (metoprolol, propranolol, carvedilol) — potential for increased plasma concentrations
- Opioids (codeine, tramadol — both CYP2D6-activated prodrugs) — berberine may reduce conversion to active metabolites, potentially reducing analgesic effect
- Warfarin — berberine may increase warfarin effect; INR should be monitored more frequently
- Metformin — berberine slows metformin absorption and reduces its peak plasma concentration, though steady-state remains adequate. The two are widely used together; the practical impact is modest.
A medication reconciliation should always precede initiating berberine. For patients on multiple medications, particularly transplant patients, mental health patients on stable psychotropic regimens, or patients on warfarin, the practical recommendation is either avoidance of berberine or close monitoring with willingness to adjust other medications.
Special Populations: CKD, Elderly, Liver Disease
Chronic kidney disease — berberine is primarily metabolized in the liver and gut, not renally cleared, so it does not accumulate in CKD. The eGFR >30 restriction that limits metformin does not apply to berberine. However, the CKD population is also typically polypharmacy and the CYP450 interaction risk is elevated; medication reconciliation is essential.
Elderly patients (>75 years) — berberine is generally well tolerated, but the higher prevalence of polypharmacy creates more drug interaction risk. Starting dose should be lower (250 mg once daily for the first week) and titration slower. Cognitive screening should be considered before initiating because some elderly patients with subclinical kernicterus-like risk factors (low albumin, multiple displacing drugs) may be vulnerable.
Liver disease — berberine has been studied in NAFLD with benefit and no safety signal. In advanced cirrhosis (Child-Pugh B or C), the limited hepatic reserve makes CYP450 interactions more clinically meaningful, and the principle of starting low and titrating slowly applies. Bilirubin displacement in jaundiced patients is theoretically a concern though has not been documented in adults; conservative practice is to avoid berberine in patients with significantly elevated bilirubin.
Cardiac arrhythmias — berberine has historically been used in China for cardiac arrhythmias (ventricular tachycardia) at higher doses. At standard 1,500 mg/day doses, no clinically meaningful effect on QT interval or other arrhythmia markers has been documented, but the molecule is a class III antiarrhythmic at high doses. For patients on QT-prolonging medications (azithromycin, fluconazole, quetiapine), the combination is reasonable but warrants attention.
Bariatric surgery — absorption is typically impaired after gastric bypass and duodenal switch. Standard berberine doses may produce reduced systemic effect; consider dihydroberberine or higher doses with monitoring.
Duration of Therapy and Monitoring
Berberine is appropriate for long-term use in patients with chronic indications (type 2 diabetes, dyslipidemia, metabolic syndrome, NAFLD, recurrent SIBO). Unlike antibiotics, there is no concern about driving resistance with chronic use, and the metabolic mechanisms continue to provide benefit indefinitely.
Recommended monitoring schedule:
- Baseline — lipid panel, HbA1c, comprehensive metabolic panel (including liver enzymes and creatinine), TSH if reasonable, medication reconciliation
- 3 months — lipid panel, HbA1c, liver enzymes. Adjust dose if needed.
- 6 months — same panel
- Annually thereafter — lipid panel, HbA1c, liver enzymes, complete blood count
If the principal indication is SIBO, a course of 4-8 weeks is typical, followed by prokinetic maintenance therapy to prevent relapse. Long-term berberine for SIBO maintenance is reasonable but the metabolic-target population is the more typical long-term user.
The most common reason for discontinuation is intolerable GI symptoms in the first month, which is largely preventable with careful titration. The second most common reason is loss of clinical benefit, which typically indicates either non-adherence or a need to switch to dihydroberberine for better systemic exposure.
Key Research Papers
- Turner N, Li JY, Gosby A et al. (2008). Berberine and its more biologically available derivative, dihydroberberine, inhibit mitochondrial respiratory complex I: a mechanism for the action of berberine. Diabetes, 57(5):1414-1418. — PubMed 18285556
- Liu YT, Hao HP, Xie HG et al. (2010). Extensive intestinal first-pass elimination and predominant hepatic distribution of berberine explain its low plasma levels in rats. Drug Metabolism and Disposition, 38(10):1779-1784. — PubMed 20634337
- Chan E (1993). Displacement of bilirubin from albumin by berberine. Biology of the Neonate, 63(4):201-208. — PubMed 8513024
- Guo Y, Chen Y, Tan ZR et al. (2012). Repeated administration of berberine inhibits cytochromes P450 in humans. European Journal of Clinical Pharmacology, 68(2):213-217. — PubMed 21870106
- Wu X, Li Q, Xin H et al. (2005). Effects of berberine on the blood concentration of cyclosporin A in renal transplanted recipients: clinical and pharmacokinetic study. European Journal of Clinical Pharmacology, 61(8):567-572. — PubMed 16133554
- Hua W, Ding L, Chen Y et al. (2007). Determination of berberine in human plasma by liquid chromatography-electrospray ionization-mass spectrometry. Journal of Pharmaceutical and Biomedical Analysis, 44(4):931-937. — PubMed 17531424
- Derosa G, Bonaventura A, Bianchi L et al. (2013). Berberis aristata combined with Silybum marianum on lipid profile in patients not tolerating statins at high doses. Atherosclerosis, 230(2):298-302. — Search PubMed
- Petrangolini G, Corti F, Ronchi M et al. (2021). Development of an innovative berberine food-grade formulation with an ameliorated absorption: in vitro evidence confirmed by healthy human volunteers pharmacokinetic study. Evidence-Based Complementary and Alternative Medicine, 2021:7563889. — Search PubMed
- Pan GY, Wang GJ, Liu XD et al. (2002). The involvement of P-glycoprotein in berberine absorption. Pharmacology and Toxicology, 91(4):193-197. — PubMed 12530470
- Wu CY, Hsu CY (2014). Cautionary notes on berberine for the treatment of hyperlipidemia. Journal of Clinical Lipidology, 8(3):348-349. — Search PubMed
- Imenshahidi M, Hosseinzadeh H (2019). Berberine and barberry (Berberis vulgaris): a clinical review. Phytotherapy Research, 33(3):504-523. — PubMed 30637820
- Habtemariam S (2016). Berberine and inflammatory bowel disease: a concise review. Pharmacological Research, 113(Pt A):592-599. — PubMed 27697643
PubMed Topic Searches
- PubMed: Berberine pharmacokinetics
- PubMed: Dihydroberberine absorption
- PubMed: Berberine bilirubin displacement
- PubMed: Berberine CYP3A4 interactions
- PubMed: Berberine phytosome and silymarin
Connections
- Berberine Overview
- Berberine Benefits Hub
- Berberine for Blood Sugar
- Berberine for Cholesterol
- Berberine for Gut Microbiome
- Berberine and Iron Overload
- Milk Thistle (Silymarin)
- Goldenseal (Hydrastis canadensis)
- Red Yeast Rice (Monacolin K)
- Type 2 Diabetes
- Dyslipidemia
- SIBO
- NAFLD
- HbA1c Lab Test
- Lipid Panel Lab Test