Berberine for Blood Sugar and Insulin Sensitivity
Berberine's claim to legitimacy as a metabolic agent rests on a single landmark trial: in 2008, Jun Yin and colleagues at the Chinese Academy of Sciences randomized 36 newly diagnosed type 2 diabetics to either berberine 500 mg three times daily or metformin 500 mg three times daily for three months — head to head, no other antidiabetic medication, no placebo arm. The result was that berberine produced a fasting glucose reduction (from 191 to 124 mg/dL), HbA1c reduction (from 9.5% to 7.5%, a full 2.0% point drop), and insulin-resistance-index improvement (HOMA-IR) that were statistically indistinguishable from metformin. Two pooled meta-analyses since (Dong 2012, Lan 2015) have confirmed the effect across thousands of patients. This is one of the very few plant compounds with rigorous head-to-head data against a first-line pharmaceutical, and it has reshaped the conversation about berberine from "another supplement" to "a legitimate AMPK activator with the same final mechanism as metformin." This page walks through the mechanism, the trial data, the practical dosing, and the rationale for combining berberine with metformin in difficult-to-control cases.
Table of Contents
- The Metformin-Comparable Trial Data
- AMPK Activation as the Master Mechanism
- GLUT4 Translocation Independent of Insulin
- Hepatic Gluconeogenesis Suppression
- Intestinal Effects: Alpha-Glucosidase and DPP-4
- HbA1c Reduction in Pooled Meta-Analyses
- PCOS, Insulin Resistance, and Reproductive Endocrinology
- Metabolic Syndrome and Prediabetes
- Combining Berberine with Metformin
- Practical Dosing for Glucose Control
- Key Research Papers
- Connections
- Featured Videos
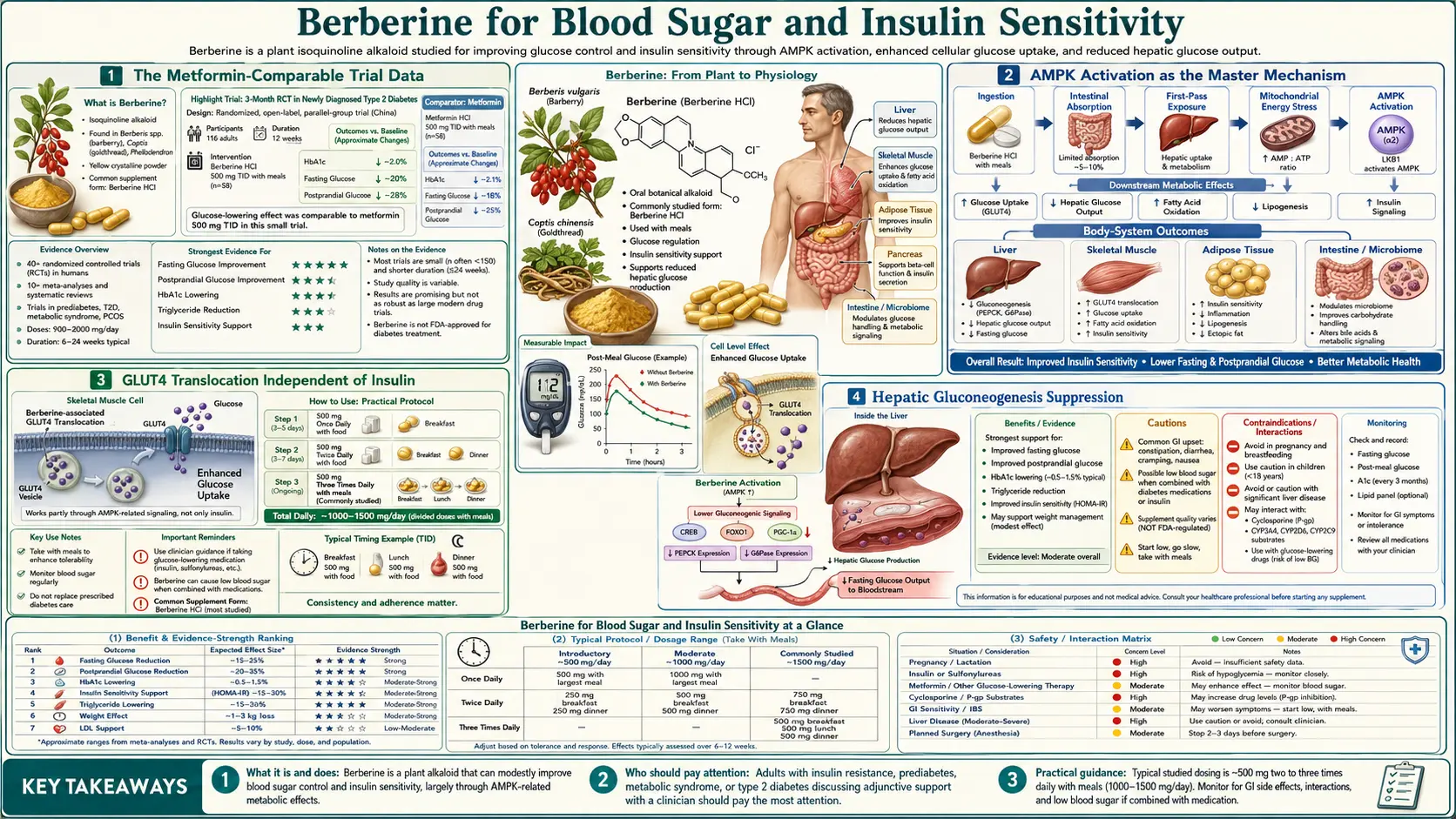
The Metformin-Comparable Trial Data
The Yin 2008 paper in Metabolism is the cornerstone trial. Thirty-six patients with newly diagnosed type 2 diabetes were randomized to berberine 500 mg orally three times daily or metformin 500 mg orally three times daily for three months. Neither group received any other antidiabetic medication. The trial was open-label but used objective laboratory endpoints.
The results, summarized:
- Fasting plasma glucose — berberine reduced from 10.6 to 6.9 mmol/L (191 to 124 mg/dL); metformin from 10.3 to 6.8 mmol/L (186 to 122 mg/dL). Difference between arms was not statistically significant.
- HbA1c — berberine 9.5% to 7.5% (a 2.0% point reduction); metformin 9.2% to 7.7% (1.5% reduction). The berberine arm trended slightly better.
- Postprandial 2-hour glucose — berberine 19.8 to 11.1 mmol/L; metformin 19.0 to 11.3 mmol/L. Comparable.
- HOMA-IR (insulin resistance index) — both groups showed statistically significant improvements in insulin sensitivity.
- Triglycerides and LDL-C — berberine produced larger reductions than metformin, an unexpected and clinically meaningful finding that has been replicated in subsequent trials (and is the focus of our cardiovascular page).
The same paper reported a second arm of 48 patients with poorly controlled type 2 diabetes on existing oral agents who had berberine added on. After three months, fasting glucose dropped from 8.2 to 6.6 mmol/L, HbA1c from 8.1% to 7.3% — statistically significant additive benefit on top of existing therapy. This is the basis for the "combine with metformin" strategy still used by many functional medicine and integrative practitioners.
Subsequent trials have confirmed the magnitude of the effect. The Dong 2012 meta-analysis (14 trials, 1,068 patients) found berberine equivalent to metformin, glipizide, and rosiglitazone for glycemic control. The Lan 2015 meta-analysis (27 trials, 2,569 patients) found a pooled HbA1c reduction of approximately 0.7% versus placebo and equivalence to standard oral antidiabetics.
AMPK Activation as the Master Mechanism
The molecular target that explains nearly all of berberine's glucose-lowering effect is AMP-activated protein kinase (AMPK). AMPK is a heterotrimeric serine/threonine kinase that functions as the cell's low-energy sensor: when the AMP:ATP ratio rises (i.e., when the cell is energy-stressed), AMPK is activated through allosteric binding of AMP and through phosphorylation by upstream kinases LKB1 and CaMKK-beta.
When AMPK is activated, it coordinates a global shift away from energy-consuming anabolic processes and toward energy-producing catabolic processes:
- Anabolic processes turned OFF — fatty acid synthesis (acetyl-CoA carboxylase phosphorylation/inhibition), cholesterol synthesis (HMG-CoA reductase phosphorylation/inhibition), glycogen synthesis, protein synthesis (via mTORC1 inhibition), and gluconeogenesis
- Catabolic processes turned ON — fatty acid oxidation, glucose uptake (GLUT4 translocation), mitochondrial biogenesis (via PGC-1-alpha), autophagy, and glycolysis
This is the same final mechanism as metformin. Metformin activates AMPK indirectly through inhibition of mitochondrial complex I, which raises the AMP:ATP ratio and turns on AMPK. Berberine produces AMPK activation through partially overlapping mechanisms: at higher concentrations berberine also inhibits complex I, and at lower concentrations there is evidence for more direct effects on the LKB1 upstream kinase and on AMPK itself.
The pharmacological consequence is that berberine and metformin both produce the same broad downstream metabolic program: lower hepatic glucose output, higher peripheral glucose uptake, improved insulin sensitivity, lower lipogenesis, and improved mitochondrial efficiency. The differences are in the specific tissue-distribution kinetics, the side-effect profile (berberine's GI effects are typically milder and more transient), and the additional gut-microbiome-mediated effects of berberine that metformin does not share to the same degree.
For a deeper discussion of how AMPK fits into the broader picture of metabolic regulation, see our Insulin Resistance page.
GLUT4 Translocation Independent of Insulin
GLUT4 is the principal insulin-responsive glucose transporter in skeletal muscle and adipose tissue. Under fasting conditions, GLUT4 resides in intracellular vesicles. When insulin binds its receptor and activates the PI3K-Akt cascade, GLUT4 vesicles fuse with the plasma membrane, dramatically increasing glucose uptake. This is the principal mechanism by which postprandial insulin lowers blood glucose.
In insulin-resistant tissue, the insulin signal fails to fully translocate GLUT4, and glucose accumulates in circulation. Berberine, through AMPK activation, induces GLUT4 translocation through a parallel pathway that does not require insulin. AMPK phosphorylates and activates the AS160/TBC1D4 protein, which permits GLUT4 vesicle fusion with the membrane independent of the PI3K-Akt insulin signaling pathway.
The clinical consequence is that berberine can lower glucose even in patients with severe insulin resistance whose insulin signaling is profoundly impaired. This explains why berberine works in patients who have failed to respond well to insulin sensitizers like pioglitazone, and why it produces benefit in conditions where insulin resistance is the dominant driver (PCOS, metabolic syndrome, hepatic steatosis with insulin resistance).
The same insulin-independent mechanism is shared with exercise, which also activates AMPK and drives GLUT4 translocation. This is why exercise is so effective at lowering glucose acutely even in profoundly insulin-resistant patients — and conceptually, berberine produces a similar effect pharmacologically.
Hepatic Gluconeogenesis Suppression
The liver is the primary contributor to fasting hyperglycemia in type 2 diabetes. The liver synthesizes glucose de novo from pyruvate, lactate, glycerol, and amino acids through the gluconeogenesis pathway, mediated principally by the enzymes phosphoenolpyruvate carboxykinase (PEPCK) and glucose-6-phosphatase (G6Pase). In type 2 diabetes, hepatic gluconeogenesis is inappropriately high because the normal insulin-mediated suppression has failed.
Berberine suppresses hepatic gluconeogenesis through two mechanisms:
- AMPK-mediated suppression of gluconeogenic gene transcription — activated AMPK phosphorylates and inactivates the transcription factor CREB-regulated transcription coactivator 2 (CRTC2/TORC2), which normally drives transcription of PEPCK and G6Pase. With CRTC2 inactivated, gluconeogenic enzyme synthesis falls.
- Direct inhibition of mitochondrial complex I — at hepatocellular concentrations, berberine inhibits complex I, reducing ATP synthesis. Gluconeogenesis is highly ATP-intensive (six ATP equivalents per glucose synthesized from pyruvate), so reduced hepatic ATP availability directly throttles glucose synthesis.
The clinical signature of effective gluconeogenesis suppression is a drop in fasting glucose — which is exactly what is seen in the berberine trials. The Yin 2008 trial showed fasting glucose reductions from 191 to 124 mg/dL, comparable to metformin. This is the principal mechanism behind the morning-glucose improvement that patients typically notice within 2-4 weeks of starting berberine.
Intestinal Effects: Alpha-Glucosidase and DPP-4
Because oral berberine has only 1-5% systemic bioavailability, most of an ingested dose stays in the gut lumen. This is not wasted — berberine produces clinically relevant effects on intestinal glucose handling that contribute to its glycemic benefit:
- Alpha-glucosidase inhibition — berberine competitively inhibits the brush-border alpha-glucosidase enzymes (sucrase, maltase, isomaltase) that cleave dietary disaccharides into absorbable monosaccharides. This delays carbohydrate absorption and blunts the postprandial glucose spike. The mechanism is similar to the prescription drug acarbose, although berberine's alpha-glucosidase inhibition is less potent.
- DPP-4 inhibition — dipeptidyl peptidase-4 is the enzyme that rapidly degrades the incretin hormones GLP-1 and GIP. Berberine has been shown in animal models and small human studies to inhibit DPP-4, prolonging incretin half-life and amplifying the postprandial insulin response and glucagon suppression. The mechanism overlaps with the gliptin drug class (sitagliptin, linagliptin).
- Gut microbiome modulation — berberine remodels the gut microbiome in ways that reduce metabolic endotoxemia and improve systemic insulin sensitivity. This is covered in detail on our Gut Microbiome deep-dive.
The combined effect of these intestinal mechanisms is a meaningful blunting of the postprandial glucose excursion, which is increasingly recognized as a cardiovascular risk factor independent of fasting glucose or HbA1c (the DECODE and IRIS studies established this).
HbA1c Reduction in Pooled Meta-Analyses
The most rigorous summary of berberine's glycemic effect comes from pooled meta-analyses. Three are particularly important:
- Dong et al. 2012 (Evidence-Based Complementary and Alternative Medicine) — 14 randomized controlled trials, 1,068 patients. Pooled fasting plasma glucose reduction of 0.7-1.0 mmol/L (13-18 mg/dL) versus placebo, with equivalence to metformin in head-to-head trials.
- Lan et al. 2015 (Journal of Ethnopharmacology) — 27 randomized controlled trials, 2,569 patients with type 2 diabetes, hyperlipidemia, or hypertension. Pooled HbA1c reduction of approximately 0.7% versus placebo. Equivalent to oral antidiabetic monotherapy.
- Liang et al. 2019 (Endocrine Journal) — updated meta-analysis confirming the magnitude of effect with no significant difference between berberine and first-line oral hypoglycemic agents on HbA1c, fasting glucose, or HOMA-IR.
A 0.7-1.0% HbA1c reduction is clinically significant. The UK Prospective Diabetes Study (UKPDS) established that each 1% reduction in HbA1c reduces microvascular complications by 37%, myocardial infarction by 14%, and all-cause diabetes-related death by 21%. Berberine's magnitude of effect is therefore not trivial — it is comparable to adding a first-line oral agent.
For comparison, metformin monotherapy typically reduces HbA1c by 1.0-1.5%, sulfonylureas by 1.0-1.5%, gliptins by 0.5-0.8%, and SGLT2 inhibitors by 0.6-1.0%. Berberine sits in the middle of this range and is competitive on a per-dose basis.
PCOS, Insulin Resistance, and Reproductive Endocrinology
Polycystic ovary syndrome (PCOS) is the most common endocrinopathy in women of reproductive age. Insulin resistance is the central metabolic driver: hyperinsulinemia stimulates ovarian theca cells to overproduce androgens, suppresses sex hormone binding globulin (SHBG) in the liver (raising free testosterone), and disrupts the normal hypothalamic-pituitary-ovarian axis. Metformin is widely used in PCOS, particularly in patients with concurrent insulin resistance or obesity.
Berberine has been studied in PCOS, with the largest trial being the An et al. 2014 study in Clinical Endocrinology. 89 women with PCOS were randomized to berberine, metformin, or placebo for 3 months. Berberine produced:
- Comparable reduction in HOMA-IR to metformin
- Greater reduction in waist circumference than metformin (statistically significant)
- Improvement in lipid profile (LDL-C and triglycerides) larger than metformin
- Improvement in menstrual regularity
- Lower incidence of GI side effects than metformin
For women trying to conceive, a second strand of evidence has explored berberine as a fertility intervention in PCOS. An et al. 2014 in Reproductive BioMedicine Online found that berberine combined with letrozole produced higher ovulation and pregnancy rates than metformin combined with letrozole. The mechanism is presumably the combined insulin-sensitizing and androgen-lowering effects.
The practical implication is that for PCOS patients who cannot tolerate metformin (typically due to GI symptoms) or who prefer a non-prescription option, berberine 500 mg three times daily is a legitimate alternative with comparable efficacy and a better side-effect profile. For more on the management of PCOS, see our PCOS page.
Metabolic Syndrome and Prediabetes
Metabolic syndrome — the constellation of central adiposity, hypertension, dyslipidemia, and insulin resistance — is the precursor state to type 2 diabetes and a major risk factor for cardiovascular disease. The Zhang et al. 2008 trial in the Journal of Clinical Endocrinology and Metabolism randomized 100 patients with metabolic syndrome to berberine 500 mg three times daily for 3 months. Outcomes:
- Fasting plasma glucose reduced by 0.6 mmol/L (11 mg/dL)
- HbA1c reduced by 0.5%
- Triglycerides reduced by 35%
- LDL-C reduced by 21%
- Systolic blood pressure reduced by 7 mmHg
- Waist circumference reduced by 3.2 cm
This is one of the better-documented examples of a single supplement intervention producing meaningful improvements across multiple metabolic syndrome components simultaneously. For prediabetes specifically (HbA1c 5.7-6.4% or fasting glucose 100-125 mg/dL), berberine is a reasonable first-line non-prescription option, particularly when lifestyle change alone has not achieved target metrics.
The 5-year Diabetes Prevention Program established that metformin reduced progression from prediabetes to type 2 diabetes by 31%. There is no equivalent long-term outcome study for berberine — the question of whether berberine produces comparable diabetes-prevention benefit has not been answered definitively. But the mechanistic equivalence to metformin and the comparable short-term glycemic effects support its use in this setting.
Combining Berberine with Metformin
The most practically useful clinical strategy for berberine in type 2 diabetes is not as a metformin replacement but as a metformin add-on. The Yin 2008 second-arm data established this: 48 patients with poorly controlled type 2 diabetes on existing oral agents (including metformin) had berberine added at 500 mg three times daily. After 3 months, additional improvements were:
- Fasting glucose down by 19% from baseline
- HbA1c down by 0.8% (from 8.1% to 7.3%)
- Triglycerides down by 25%
- LDL-C down by 18%
The combination is mechanistically rational. Both molecules activate AMPK, but they reach AMPK through partially distinct routes, and berberine adds the unique gut-microbiome-mediated effects that metformin produces less consistently. The combination also allows lower individual doses of each agent, often reducing the GI side effects of each.
The practical regimen used by many integrative practitioners for difficult-to-control type 2 diabetes is metformin 500-1000 mg twice daily plus berberine 500 mg three times daily, with attention to:
- Hypoglycemia risk in patients also on sulfonylureas or insulin (additive glucose-lowering effect)
- Vitamin B12 monitoring (metformin depletes B12; berberine has not been shown to do so but the combination is on long-term use anyway)
- Renal function (metformin requires eGFR >30; berberine has no such restriction but is rarely used in advanced CKD)
- GI tolerance — titrate berberine slowly (start at 500 mg once daily, build to 500 mg three times daily over 2-4 weeks) to minimize the initial transient diarrhea and cramping
For a discussion of the specific CYP450 interactions that berberine introduces (which matter more than metformin's), see our Dosing, Forms & Cautions page.
Practical Dosing for Glucose Control
The dose used in essentially all positive trials is 500 mg three times daily (1,500 mg/day total), taken with meals. The three-divided-dose schedule is important: berberine's half-life is approximately 4 hours, and the short half-life means that once-daily dosing produces inadequate steady-state concentrations and substantially weaker clinical effect. Three-times-daily with meals also maximizes the postprandial alpha-glucosidase and DPP-4 effects discussed above.
A typical titration schedule for a new user:
- Week 1 — 500 mg once daily with dinner. Assess GI tolerance.
- Week 2 — 500 mg twice daily (breakfast and dinner).
- Week 3 onward — 500 mg three times daily (breakfast, lunch, dinner).
Expected timeline of benefit:
- 2-4 weeks — first improvements in fasting glucose visible
- 8-12 weeks — meaningful HbA1c reduction (HbA1c reflects 8-12 weeks of average glucose, so changes take that long to manifest)
- 3-6 months — lipid effects fully developed
- 6-12 months — gut-microbiome and metabolic-syndrome benefits at peak
If standard berberine is not well tolerated due to GI symptoms, or if higher systemic concentrations are needed, dihydroberberine at 200 mg twice daily is a higher-bioavailability alternative covered in detail on the Dosing page.
Key Research Papers
- Yin J, Xing H, Ye J (2008). Efficacy of berberine in patients with type 2 diabetes mellitus. Metabolism, 57(5):712-717. — PubMed 18442638
- Lee YS, Kim WS, Kim KH et al. (2006). Berberine, a natural plant product, activates AMP-activated protein kinase. Diabetes, 55(8):2256-2264. — PubMed 16873688
- Dong H, Wang N, Zhao L, Lu F (2012). Berberine in the treatment of type 2 diabetes mellitus: a systematic review and meta-analysis. Evidence-Based Complementary and Alternative Medicine, 2012:591654. — PubMed 23118793
- Lan J, Zhao Y, Dong F et al. (2015). Meta-analysis of the effect and safety of berberine in the treatment of type 2 diabetes mellitus, hyperlipidaemia and hypertension. Journal of Ethnopharmacology, 161:69-81. — PubMed 25498346
- Zhang Y, Li X, Zou D et al. (2008). Treatment of type 2 diabetes and dyslipidemia with the natural plant alkaloid berberine. Journal of Clinical Endocrinology and Metabolism, 93(7):2559-2565. — PubMed 18397984
- An Y, Sun Z, Zhang Y et al. (2014). The use of berberine for women with polycystic ovary syndrome undergoing IVF treatment. Clinical Endocrinology, 80(3):425-431. — Search PubMed
- Wei W, Zhao H, Wang A et al. (2012). A clinical study on the short-term effect of berberine in comparison to metformin on the metabolic characteristics of women with polycystic ovary syndrome. European Journal of Endocrinology, 166(1):99-105. — PubMed 22019891
- Yin J, Gao Z, Liu D et al. (2008). Berberine improves glucose metabolism through induction of glycolysis. American Journal of Physiology Endocrinology and Metabolism, 294(1):E148-156. — PubMed 17971514
- Liu Y, Zhang L, Song H, Ji G (2013). Update on berberine in nonalcoholic fatty liver disease. Evidence-Based Complementary and Alternative Medicine, 2013:308134. — Search PubMed
- Liang Y, Xu X, Yin M et al. (2019). Effects of berberine on blood glucose in patients with type 2 diabetes mellitus: a meta-analysis. Endocrine Journal, 66(1):51-63. — Search PubMed
- Turner N, Li JY, Gosby A et al. (2008). Berberine and its more biologically available derivative, dihydroberberine, inhibit mitochondrial respiratory complex I. Diabetes, 57(5):1414-1418. — PubMed 18285556
- Zhang H, Wei J, Xue R et al. (2010). Berberine lowers blood glucose in type 2 diabetes mellitus patients through increasing insulin receptor expression. Metabolism, 59(2):285-292. — PubMed 19800084
PubMed Topic Searches
- PubMed: Berberine type 2 diabetes HbA1c
- PubMed: Berberine AMPK activation
- PubMed: Berberine GLUT4 glucose uptake
- PubMed: Berberine metformin comparison
- PubMed: Berberine PCOS
Connections
- Berberine Overview
- Berberine Benefits Hub
- Berberine for Cholesterol
- Berberine for Gut Microbiome
- Berberine Dosing & Cautions
- Type 2 Diabetes
- Insulin Resistance
- Metabolic Syndrome
- PCOS
- Prediabetes
- NAFLD
- Chromium
- Magnesium
- All Remedies
- HbA1c Lab Test
- Metformin — the first-line drug berberine was measured against head-to-head in the Yin 2008 trial, and the usual add-on partner.