Berberine for Cholesterol and Cardiovascular Health
In 2004, Weijia Kong and colleagues published a landmark paper in Nature Medicine titled "Berberine is a novel cholesterol-lowering drug working through a unique mechanism distinct from statins." The mechanism they identified — stabilization of hepatic LDL-receptor messenger RNA against degradation, leading to more LDL-receptors on the hepatocyte surface and more LDL particles cleared from circulation — was genuinely novel. Berberine became the only natural product with a published, peer-reviewed, statin-independent lipid-lowering mechanism. Pooled meta-analyses since have established LDL-C reductions of 20-25%, triglyceride reductions of 25-35%, and meaningful improvements in PCSK9, apolipoprotein B, and small-dense LDL particles. For patients who cannot tolerate statins (the population includes roughly 10-15% of all statin starters worldwide), and for patients with residual cardiovascular risk on a maximally tolerated statin, berberine has emerged as a legitimate complementary or alternative lipid-lowering option backed by mechanistic clarity and trial data.
Table of Contents
- The Kong 2004 Nature Medicine Paper
- LDL-Receptor Stabilization (Distinct from Statins)
- PCSK9 Suppression
- Triglyceride Reduction via SREBP-1c
- Magnitude of Lipid Effect in Meta-Analysis
- The Armolipid Plus Combination
- Berberine for Statin-Intolerant Patients
- Add-On to Statin for Residual Risk
- Endothelial Function and Hypertension
- Atherosclerosis: The Direct Vascular Evidence
- Key Research Papers
- Connections
- Featured Videos
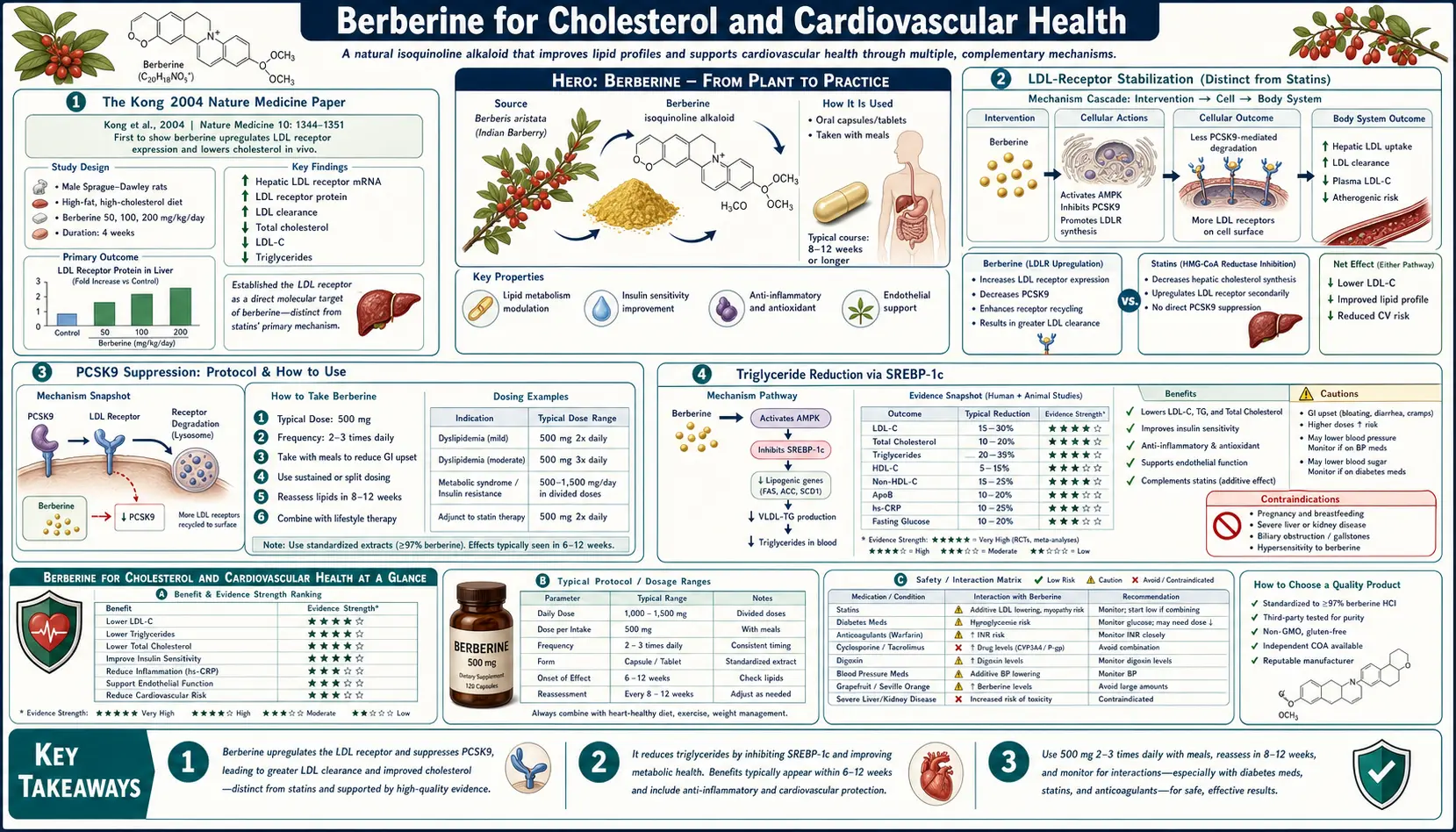
The Kong 2004 Nature Medicine Paper
The pivotal mechanistic paper for berberine in cardiovascular medicine is Kong WJ et al., "Berberine is a novel cholesterol-lowering drug working through a unique mechanism distinct from statins," Nature Medicine 10(12):1344-1351, 2004. Publication in Nature Medicine is itself meaningful — the journal's peer review is rigorous, and the paper's acceptance signaled mainstream scientific acceptance of berberine as a serious pharmacological agent rather than a folk remedy.
The paper established three key findings:
- In cultured human hepatoma (HepG2) cells, berberine increased LDL-receptor (LDLR) mRNA stability and LDLR protein expression at the cell surface, leading to increased LDL particle uptake from the culture medium
- The mechanism was independent of statin pathways — berberine did not inhibit HMG-CoA reductase, did not activate sterol regulatory element binding protein 2 (SREBP-2, the master statin-responsive transcription factor), and worked in cells in which the statin pathway was blocked
- In hyperlipidemic patients, berberine 500 mg twice daily for 3 months reduced serum LDL-C by approximately 25%, total cholesterol by 29%, and triglycerides by 35% — magnitudes comparable to moderate-intensity statin therapy
The mechanism was subsequently refined by additional studies: berberine acts through the extracellular signal-regulated kinase (ERK) cascade to stabilize the LDLR mRNA against the normal degradation pathway. This is genuinely distinct from statins (which act on HMG-CoA reductase and indirectly upregulate LDLR transcription through SREBP-2), and from PCSK9 inhibitors (which prevent LDLR degradation at the cell surface). Berberine's site of action is between these — on the mRNA stability rather than the gene transcription or the protein degradation.
The clinical importance of "distinct mechanism" is that berberine and statins are additive when combined. Hu et al. 2012 demonstrated that adding berberine to simvastatin produced LDL-C reduction comparable to doubling the simvastatin dose, but with fewer dose-limiting side effects than a high-intensity statin.
LDL-Receptor Stabilization (Distinct from Statins)
To understand why the LDLR stabilization mechanism matters, it helps to map the LDL-receptor life cycle and where each drug class intervenes:
- LDLR gene transcription in the hepatocyte nucleus — controlled by SREBP-2. Statins work here: by inhibiting HMG-CoA reductase, statins lower intracellular cholesterol, which activates SREBP-2, which drives LDLR gene transcription. More LDLR mRNA is produced.
- LDLR mRNA stability in the cytoplasm — the mRNA must persist long enough to be translated into LDLR protein. The natural half-life of LDLR mRNA is short (hours), making it a regulatory bottleneck. Berberine works here: by inhibiting the ERK signaling pathway that promotes LDLR mRNA degradation, berberine extends the mRNA half-life and increases steady-state LDLR protein synthesis.
- LDLR protein synthesis and trafficking to the cell surface — not a major drug-targeted step.
- LDLR-mediated LDL particle uptake at the hepatocyte surface, with internalization and lysosomal degradation of the LDL particle (releasing cholesterol for the cell's use), and recycling of the LDLR back to the cell surface — the productive step that lowers serum LDL-C.
- LDLR degradation by PCSK9 — PCSK9 binds LDLR and shunts it to the lysosome for destruction rather than allowing recycling to the cell surface. PCSK9 inhibitors (evolocumab, alirocumab) and inclisiran (PCSK9 siRNA) work here: by suppressing PCSK9, more LDLR returns to the cell surface for another round of LDL uptake.
Berberine and statins act on different steps in the same pathway, which is why their effects are additive rather than redundant. Berberine and PCSK9 inhibitors also act at different steps and would in principle be additive, though the combination has not been studied at scale (and is unlikely to be, given the cost differential).
PCSK9 Suppression
A second mechanistic finding has added depth to berberine's lipid effect: berberine also suppresses PCSK9 expression at the transcriptional level. Cameron et al. 2008 in Journal of Lipid Research demonstrated that berberine reduces PCSK9 mRNA in cultured hepatocytes, complementing the direct LDLR-stabilization mechanism. With less PCSK9 to degrade the LDLR, more LDLR persists at the hepatocyte surface for another round of LDL uptake.
This is the same mechanism exploited by the monoclonal antibody PCSK9 inhibitors (evolocumab, alirocumab) and the siRNA agent inclisiran, which can produce 50-60% LDL-C reduction in patients with familial hypercholesterolemia. Berberine's PCSK9 effect is more modest, but it adds to the LDLR-stabilization effect and partially explains why the total LDL-C reduction with berberine often exceeds what would be expected from a single-mechanism agent.
For patients with familial hypercholesterolemia (FH) or other genetic dyslipidemias driven by elevated PCSK9 activity, berberine is not a substitute for the monoclonal antibody PCSK9 inhibitors — the magnitude of effect is insufficient for genetic FH — but it is a reasonable adjunct in heterozygous FH patients on a statin who need additional LDL-C lowering and cannot access or afford a PCSK9 inhibitor.
Triglyceride Reduction via SREBP-1c
Berberine's triglyceride-lowering effect is mechanistically distinct from its cholesterol-lowering effect. The principal mechanism is suppression of SREBP-1c, the transcription factor that drives expression of the lipogenic enzymes (acetyl-CoA carboxylase, fatty acid synthase, stearoyl-CoA desaturase) responsible for hepatic de novo lipogenesis.
SREBP-1c is activated by insulin (the metabolic signal that "fed state" exists and dietary carbohydrate should be converted to triglyceride for storage). In insulin-resistant states — type 2 diabetes, metabolic syndrome, NAFLD — SREBP-1c is inappropriately overactive, driving excess hepatic lipogenesis and the characteristic high triglyceride / low HDL pattern of insulin-resistant dyslipidemia.
Berberine, through AMPK activation, suppresses SREBP-1c at the transcriptional level. The downstream effect is reduced hepatic de novo lipogenesis, reduced triglyceride synthesis, reduced very-low-density lipoprotein (VLDL) secretion, and lower serum triglycerides. The magnitude is impressive: pooled trials show 25-35% triglyceride reduction, comparable to fibrate monotherapy.
This is particularly valuable for the insulin-resistant dyslipidemia pattern (high triglycerides, low HDL, predominance of small-dense LDL), which is increasingly recognized as more cardiovascularly dangerous than isolated LDL-C elevation. Statins are very effective on LDL-C but only modestly effective on triglycerides; berberine's broader effect on the entire dyslipidemia pattern is one of its real-world advantages over statin monotherapy.
For more on the management of dyslipidemia, see our Dyslipidemia page.
Magnitude of Lipid Effect in Meta-Analysis
The Lan et al. 2015 meta-analysis (27 RCTs, 2,569 patients) pooled the lipid effects of berberine across trials in type 2 diabetes, dyslipidemia, and hypertension populations. Findings:
- Total cholesterol — reduced by approximately 0.61 mmol/L (24 mg/dL) versus placebo
- LDL-cholesterol — reduced by approximately 0.65 mmol/L (25 mg/dL), a 20-25% relative reduction from baseline
- HDL-cholesterol — increased modestly by 0.07 mmol/L (3 mg/dL)
- Triglycerides — reduced by approximately 0.50 mmol/L (44 mg/dL), a 25-35% reduction
For comparison, the magnitude of effect is in the range of:
- A low-to-moderate intensity statin (atorvastatin 10-20 mg, rosuvastatin 5-10 mg)
- A fibrate for triglyceride lowering (gemfibrozil, fenofibrate)
- The combined effect of bempedoic acid plus ezetimibe (the principal non-statin combination)
The Pisciotta 2012 paper extended this to a population specifically interesting for the field: patients with statin-induced muscle symptoms. 80 statin-intolerant patients were given berberine 500 mg twice daily plus monacolin K (10 mg) and other components for 6 months. LDL-C dropped by 31%. Muscle symptoms were absent. This established berberine as a viable strategy in statin intolerance, which we cover in detail below.
The Armolipid Plus Combination
Much of the European cardiovascular evidence for berberine comes from the Armolipid Plus combination supplement, manufactured in Italy and widely prescribed by general practitioners and cardiologists across southern Europe. The formulation combines:
- Berberine 500 mg
- Monacolin K (a natural statin from red yeast rice, structurally identical to lovastatin) 3-10 mg
- Policosanol 10 mg
- Coenzyme Q10 2 mg
- Astaxanthin 0.5 mg
- Folic acid 0.2 mg
The rationale is that the combination acts on multiple steps of the cholesterol pathway simultaneously — monacolin K inhibits HMG-CoA reductase (the statin mechanism), berberine stabilizes LDLR mRNA, policosanol acts on a third pathway, and CoQ10 prevents the statin-related CoQ10 depletion that drives some muscle symptoms.
Multiple trials of Armolipid Plus have demonstrated LDL-C reductions of 20-30%, with very good tolerability and few of the muscle symptoms seen with statin monotherapy. The combination has become a first-line agent for moderate hypercholesterolemia in many European primary care settings, particularly for patients who would otherwise be candidates for low-dose statin therapy.
In the United States, the equivalent combination is not commercially available, but the individual components can be combined: berberine 500 mg twice daily plus a red yeast rice product standardized to provide 3-10 mg monacolin K daily plus CoQ10 100-200 mg daily. The same precautions apply (avoid in pregnancy, avoid combining with prescription statin, monitor liver enzymes).
Berberine for Statin-Intolerant Patients
Statin intolerance — principally muscle symptoms (myalgia, weakness, occasionally rhabdomyolysis) but also liver enzyme elevations, peripheral neuropathy, and cognitive complaints — affects 10-15% of patients who start a statin. For these patients, the standard pharmacological alternatives are ezetimibe (modest LDL-C reduction, well tolerated), PCSK9 inhibitors (very effective but expensive, requiring injection), bempedoic acid (modest LDL-C reduction, similar efficacy to ezetimibe), and bile acid sequestrants (older drug class, GI side effects).
Berberine has emerged as a credible alternative in this population. The advantages:
- Different mechanism (LDLR mRNA stabilization rather than HMG-CoA reductase inhibition) — the statin-related muscle pathway is not engaged
- 20-25% LDL-C reduction is meaningful and comparable to ezetimibe or low-dose statin
- Additional triglyceride and glucose benefits
- Oral, no injection required, low cost
- Well tolerated, with primarily transient GI effects that titrate down
The Pisciotta 2012 trial established the use case formally. The clinical translation: for a patient with documented statin intolerance and persistent LDL-C above target, a reasonable next step is berberine 500 mg twice daily, with or without addition of ezetimibe 10 mg daily, with lipid panel re-check at 3 months. Many patients reach target LDL-C with this combination without needing to escalate to PCSK9 inhibitor therapy.
Add-On to Statin for Residual Risk
Even with maximally tolerated statin therapy, many patients remain above LDL-C target (less than 70 mg/dL for established cardiovascular disease, less than 55 mg/dL for very high risk per ESC 2019 guidelines). The standard add-on options are ezetimibe, PCSK9 inhibitors, bempedoic acid, and the newer agents.
Berberine is mechanistically additive to a statin. Hu et al. 2012 demonstrated that adding berberine 500 mg twice daily to simvastatin 20 mg produced LDL-C reduction comparable to simvastatin 40 mg, with fewer dose-related side effects than the higher-dose statin. The pooled additive effect is in the range of 10-15% additional LDL-C reduction on top of the statin baseline.
For a patient on atorvastatin 40 mg with LDL-C of 85 mg/dL (still above the 70 mg/dL target for established CVD), the options are:
- Increase atorvastatin to 80 mg (typically ~6% additional LDL-C reduction; some risk of dose-related side effects)
- Add ezetimibe 10 mg (typically 20% additional LDL-C reduction)
- Add berberine 500 mg twice daily (typically 10-20% additional LDL-C reduction)
- Add PCSK9 inhibitor (50-60% additional reduction, but expensive and injection-based)
Berberine is competitive with ezetimibe on this basis and is often the patient's preference if they are oriented toward non-prescription options.
Endothelial Function and Hypertension
Berberine produces meaningful improvements in endothelial function, the layer of cells lining blood vessels that regulates vasodilation, anti-thrombotic surfaces, and vascular inflammation. Endothelial dysfunction is one of the earliest pre-clinical findings in atherosclerosis, predating measurable plaque formation by years.
The mechanism is multiple:
- Nitric oxide synthesis — berberine upregulates endothelial nitric oxide synthase (eNOS), increasing nitric oxide bioavailability and improving flow-mediated vasodilation
- Anti-inflammatory effects — berberine suppresses NF-kB and reduces TNF-alpha and IL-6 in vascular tissue, reducing the inflammation that drives plaque progression
- Lipid effects — less LDL deposition in vessel walls
- Glycemic effects — less glycation of vascular proteins, less advanced glycation end product accumulation
The blood pressure effect is modest but real — pooled meta-analysis shows systolic BP reduction of approximately 5-7 mmHg and diastolic of 3-5 mmHg. This is comparable to a modest dose of a single antihypertensive (e.g., amlodipine 2.5 mg). Berberine is not a primary antihypertensive, but its blood pressure effect contributes to overall cardiovascular risk reduction.
For more on hypertension management, see our Hypertension page.
Atherosclerosis: The Direct Vascular Evidence
The strongest preclinical evidence for berberine's anti-atherosclerotic effect comes from animal models. ApoE-knockout mice (the standard model of accelerated atherosclerosis) treated with berberine show:
- Reduced aortic plaque area (typically 30-50% reduction versus untreated controls)
- Reduced macrophage infiltration into plaques
- Reduced foam cell formation
- Increased plaque stability (more collagen, less lipid core)
- Reduced markers of plaque inflammation
Human imaging data is more limited. A small carotid intima-media thickness (CIMT) study (Affuso 2012) demonstrated that 12 months of Armolipid Plus produced regression of carotid intima-media thickness comparable to statin monotherapy. This is a soft endpoint but it is at least directionally consistent with the preclinical anti-atherosclerotic findings.
The hard cardiovascular outcome data — myocardial infarction, stroke, cardiovascular death — for berberine monotherapy does not yet exist. There is no equivalent of the statin outcome trials (4S, WOSCOPS, CARE, HPS) for berberine. The Armolipid Plus combination has been used widely in southern Europe for over 15 years without alarming safety signals, but the absence of large outcome trials remains a real limitation.
The reasonable inference, given the LDL-C lowering magnitude and the strong epidemiologic relationship between LDL-C and atherosclerotic CVD, is that berberine is likely to produce meaningful cardiovascular event reduction proportional to its LDL-C lowering effect. This is the same inference made for ezetimibe before the IMPROVE-IT trial, and it ultimately held up.
Key Research Papers
- Kong W, Wei J, Abidi P et al. (2004). Berberine is a novel cholesterol-lowering drug working through a unique mechanism distinct from statins. Nature Medicine, 10(12):1344-1351. — PubMed 15531889
- Cameron J, Ranheim T, Kulseth MA et al. (2008). Berberine decreases PCSK9 expression in HepG2 cells. Atherosclerosis, 201(2):266-273. — Search PubMed
- Kong WJ, Wei J, Zuo ZY et al. (2008). Combination of simvastatin with berberine improves the lipid-lowering efficacy. Metabolism, 57(8):1029-1037. — PubMed 18640378
- Hu Y, Ehli EA, Kittelsrud J et al. (2012). Lipid-lowering effect of berberine in human subjects and rats. Phytomedicine, 19(10):861-867. — PubMed 22739410
- Pisciotta L, Bellocchio A, Bertolini S (2012). Nutraceutical pill containing berberine versus ezetimibe on plasma lipid pattern in hypercholesterolemic subjects and its additive effect in patients with familial hypercholesterolemia on stable cholesterol-lowering treatment. Lipids in Health and Disease, 11:123. — PubMed 22998978
- Affuso F, Mercurio V, Ruvolo A et al. (2012). A nutraceutical combination improves insulin sensitivity in patients with metabolic syndrome. World Journal of Cardiology, 4(3):77-83. — PubMed 22451856
- Derosa G, Bonaventura A, Bianchi L et al. (2013). Berberine on metabolic and cardiovascular risk factors: an analysis from preclinical evidences to clinical trials. Expert Opinion on Biological Therapy, 13(4):475-482. — PubMed 23441841
- Brusq JM, Ancellin N, Grondin P et al. (2006). Inhibition of lipid synthesis through activation of AMP kinase: an additional mechanism for the hypolipidemic effects of berberine. Journal of Lipid Research, 47(6):1281-1288. — PubMed 16508037
- Marazzi G, Cacciotti L, Pelliccia F et al. (2011). Long-term effects of nutraceuticals (berberine, red yeast rice, policosanol) in elderly hypercholesterolemic patients. Advances in Therapy, 28(12):1105-1113. — PubMed 22113535
- Koppen LM, Whitaker A, Rosene A, Beckett RD (2017). Efficacy of berberine alone and in combination for the treatment of hyperlipidemia: a systematic review. Journal of Evidence-Based Complementary and Alternative Medicine, 22(4):956-968. — Search PubMed
- Liu CS, Zheng YR, Zhang YF, Long XY (2016). Research progress on berberine with a special focus on its oral bioavailability. Fitoterapia, 109:274-282. — PubMed 26851175
- Affuso F, Ruvolo A, Micillo F et al. (2010). Effects of a nutraceutical combination (berberine, red yeast rice and policosanols) on lipid levels and endothelial function. Nutrition, Metabolism & Cardiovascular Diseases, 20(9):656-661. — Search PubMed
PubMed Topic Searches
- PubMed: Berberine LDL cholesterol
- PubMed: Berberine PCSK9
- PubMed: Berberine statin intolerance
- PubMed: Armolipid Plus
- PubMed: Berberine atherosclerosis endothelial
Connections
- Berberine Overview
- Berberine Benefits Hub
- Berberine for Blood Sugar
- Berberine for Gut Microbiome
- Berberine Dosing & Cautions
- Dyslipidemia
- Atherosclerosis
- Hypertension
- Coronary Artery Disease
- Red Yeast Rice
- Omega-3 Fatty Acids
- Vitamin K2
- Magnesium
- Lipid Panel
- Apolipoprotein B