Aluminum Toxicity: Sources, Symptoms, Diagnosis, and Treatment
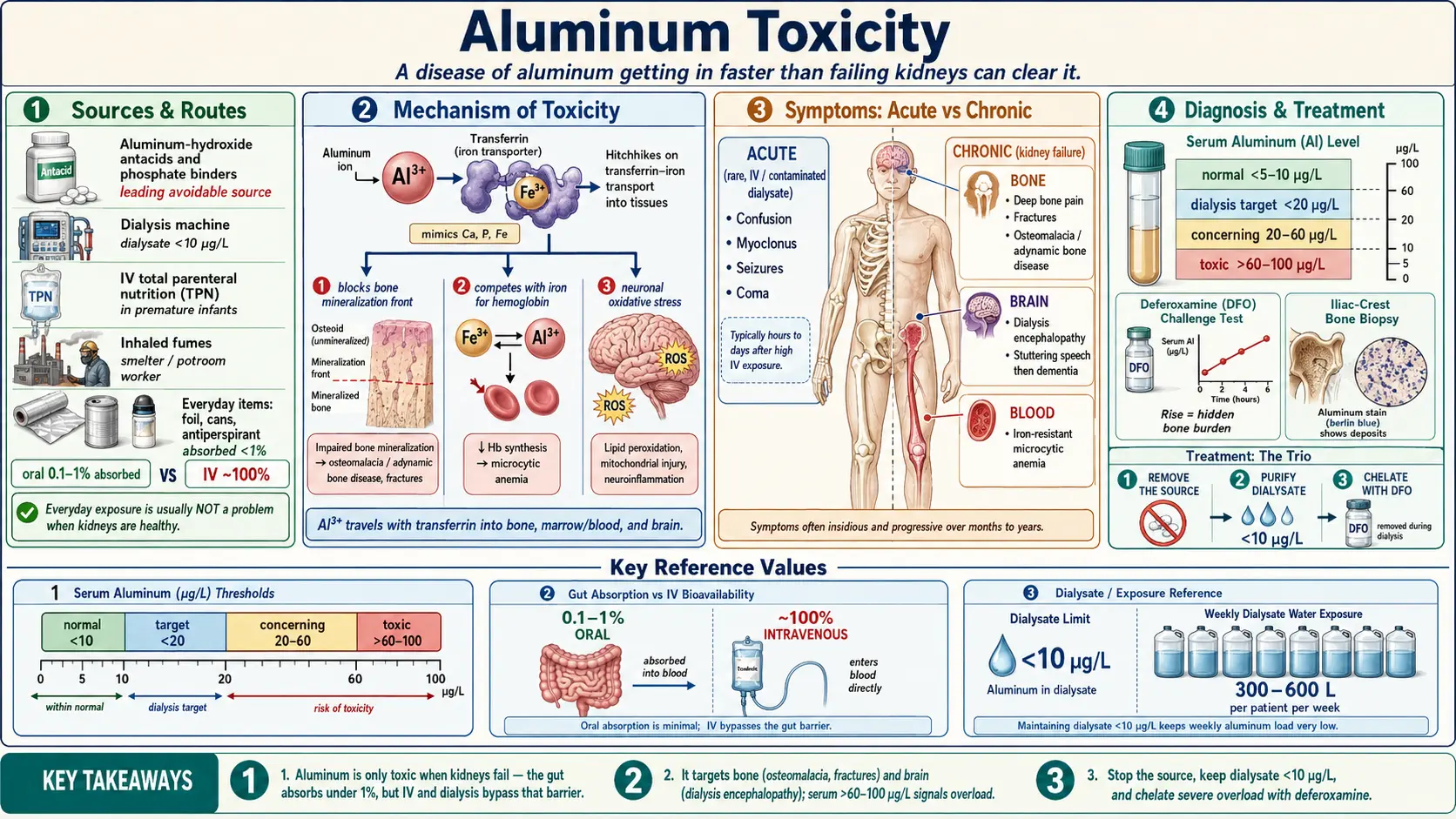
Table of Contents
- Overview
- Sources & Routes of Exposure
- Toxicokinetics
- Mechanism of Toxicity
- Symptoms & Health Effects
- Diagnosis & Laboratory Testing
- Treatment & Management
- Prevention & Risk Reduction
- Related Topics
- Key Research Papers
- Connections
- Featured Videos
1. Overview
Aluminum is the most abundant metal in the Earth's crust, and small traces of it are in almost everything you eat, drink, and breathe. For the vast majority of healthy people, this everyday background exposure is harmless: the gut absorbs only a tiny fraction of the aluminum in food, and healthy kidneys quietly clear what little does get into the blood. Aluminum is not an essential nutrient — your body has no use for it — but in ordinary circumstances it simply passes through without causing harm.
Aluminum toxicity is therefore not a disease of the general population. It is, overwhelmingly, a disease of aluminum getting in faster than the kidneys can clear it, or of the kidneys being unable to clear it at all. The single most important risk group is people with advanced chronic kidney disease (CKD), especially those on dialysis, because aluminum is eliminated almost entirely by the kidneys. When kidney function fails and aluminum keeps arriving — historically from contaminated dialysis water, and still today from aluminum-based antacids and phosphate binders — it accumulates in the bones, brain, and blood-forming tissue and causes real, sometimes devastating, harm.
The classic example is “dialysis encephalopathy,” sometimes called dialysis dementia, an epidemic of progressive brain disease that struck dialysis units in the 1970s and 1980s before the aluminum in dialysis water and oral binders was recognized as the cause. Once water-purification standards and aluminum-free binders were adopted, this devastating syndrome largely disappeared — one of the clearer success stories in toxicology. The same population can also develop a crumbling, painful bone disease and a stubborn anemia from aluminum overload.
This page explains where aluminum exposure comes from, how the body handles it, what it actually does at the cellular level, and — in plain language but with real numbers — how doctors recognize and treat aluminum overload. It also addresses two questions that worry many people: whether aluminum in antiperspirants causes breast cancer (the evidence does not show that it does), and whether aluminum causes Alzheimer's disease (a long-debated idea that mainstream science has not been able to confirm).
2. Sources & Routes of Exposure
Aluminum can reach the body by mouth (the most common route), through the bloodstream when it bypasses the gut entirely, or by breathing dust and fumes at work. Understanding which route matters helps explain why some exposures are trivial and others are dangerous: the gut is a strong barrier, so swallowing aluminum is far safer than having it injected or inhaled.
Medicines: the leading avoidable source
The biggest controllable source of a meaningful aluminum load is medication. Aluminum hydroxide is the active ingredient in some antacids and, more importantly, in phosphate binders — pills given to people with kidney failure to soak up dietary phosphate in the gut. A person with healthy kidneys absorbs almost none of this; a person on dialysis absorbs a little, cannot excrete it, and can slowly build up a toxic body burden over months and years. Because of this, aluminum-based binders have largely been replaced by calcium-, lanthanum-, or sevelamer-based binders in modern kidney care, and are used — if at all — only briefly.
Dialysis water: the historical disaster, now largely solved
A dialysis patient's blood is exposed to roughly 300–600 liters of water-based dialysate every week, separated from the blood only by a thin membrane. If that water contains aluminum — as municipal water often did, partly because aluminum salts are used to purify drinking water — the metal crosses straight into the bloodstream, completely bypassing the protective gut. This was the cause of the 1970s–1980s epidemic of dialysis encephalopathy and aluminum bone disease. The fix was engineering: modern units treat dialysis water with reverse osmosis and deionization, and regulations cap aluminum in dialysate at very low levels (commonly under 10 µg/L). This single change is why severe aluminum toxicity is now rare.
Intravenous nutrition in newborns
Premature and critically ill infants who are fed entirely through a vein (total parenteral nutrition, or TPN) are vulnerable because the nutrient solutions themselves can be contaminated with aluminum, and an infant's immature kidneys clear it poorly. Aluminum delivered this way bypasses the gut barrier entirely. Studies have documented aluminum loading and associated bone and possible neurodevelopmental effects in this group, which is why the U.S. FDA set limits on aluminum content in parenteral nutrition components and pharmacies now monitor it closely.
Occupational exposure
Workers who smelt aluminum or work in “potrooms” (where molten aluminum is produced by electrolysis), as well as aluminum welders and those exposed to certain aluminum-containing dusts, can inhale aluminum fumes and fine particles. Heavy, long-term inhalation has been linked to lung effects and, in some reports, neurological symptoms. Occupational limits (set by agencies such as OSHA) and respiratory protection are the main safeguards.
The Camelford incident
In July 1988, around 20 tonnes of aluminum sulfate were accidentally dumped into the public drinking-water supply at Camelford, in Cornwall, UK, briefly contaminating tap water for thousands of residents. The episode became a long-running case study in possible health effects of a sudden, high oral aluminum exposure in people with normal kidneys, and follow-up research reported some neurological complaints among the exposed — though interpreting these is complicated by the alarm and stress the incident caused.
Everyday exposures that are usually reassuring
- Cookware, foil, and beverage cans: Cooking acidic foods in aluminum pots or foil can transfer small amounts of aluminum into food, but the increase is modest and the gut absorbs little of it. In people with healthy kidneys this is not considered a meaningful health risk.
- Food additives: Some baking powders, processed cheeses, and other foods contain aluminum-based additives (such as sodium aluminum phosphate). These add to total dietary intake but, again, are poorly absorbed.
- Antiperspirants: Aluminum salts plug sweat ducts to reduce perspiration. Despite persistent online claims, well-designed epidemiologic research has not found that antiperspirant use causes breast cancer; this is discussed further in the Symptoms section.
- Drinking water: Aluminum is used to clarify municipal water; the U.S. EPA sets a secondary (aesthetic) standard of 0.05–0.2 mg/L, mainly to limit discoloration rather than because of toxicity at those levels.
The common thread: oral and everyday exposures are buffered by poor gut absorption and good kidney clearance, while injected, inhaled, and dialysis exposures — or any exposure in someone with failing kidneys — are the ones that cause toxicity.
3. Toxicokinetics
Toxicokinetics is simply the story of what the body does to a substance: how much gets in, where it goes, and how it leaves. For aluminum, that story explains almost everything about who gets sick and who doesn't.
Absorption: a very leaky-on-paper, tight-in-practice gut
When aluminum is swallowed, only about 0.1–1% is actually absorbed from the gut into the bloodstream — the rest passes out in stool. The exact fraction depends on the chemical form and what it is taken with; for example, citrate (found in citrus juices and some supplements) can substantially increase aluminum absorption, which is why taking aluminum-containing antacids together with citrate-rich drinks is discouraged. By contrast, aluminum delivered by vein (dialysis or TPN) is essentially 100% “absorbed,” because it skips the gut entirely. This contrast — under 1% by mouth versus all of it by vein — is the single most important fact in aluminum toxicology.
Distribution: a hitchhiker on iron's transport system
Once in the blood, most aluminum binds to transferrin, the same protein the body uses to carry iron. Because aluminum and iron behave somewhat alike chemically (both are trivalent metal ions), aluminum effectively rides iron's transport and uptake machinery into tissues. Over time it deposits preferentially in bone and brain, and also in the liver and parathyroid glands. In bone it lodges at the mineralization front, the very surface where new bone is being laid down; in the brain it can reach regions involved in memory and cognition. This bone-and-brain targeting is why chronic aluminum overload shows up as bone disease and encephalopathy rather than, say, kidney or heart damage.
Elimination: almost entirely the kidneys
The body's main exit door for absorbed aluminum is the kidney, with a small contribution from bile. In a person with normal renal function, aluminum that reaches the blood is filtered and excreted in urine, keeping the body burden low. But the corollary is stark: if the kidneys fail, that exit door closes. Aluminum then has nowhere to go and accumulates in bone and brain. This is precisely why chronic kidney disease and dialysis transform aluminum from a harmless trace metal into a genuine poison — not because exposure rises dramatically, but because clearance collapses.
4. Mechanism of Toxicity
Aluminum has no normal job in the body, so its harm comes from impersonating and interfering with metals and minerals the body does use — chiefly calcium, phosphate, magnesium, and iron. Several overlapping mechanisms have been described.
Disrupting bone mineralization
Healthy bone is constantly remodeled: old bone is removed and new bone is laid down and then hardened by depositing calcium and phosphate as a mineral crystal. Aluminum collects at the mineralization front and physically and chemically blocks this hardening step. The result is bone that is built but never properly mineralized — soft, weak, and painful. In some patients aluminum also suppresses the bone-building cells (osteoblasts) and dampens the entire remodeling cycle, producing adynamic (low-turnover) bone disease, in which bone barely renews itself at all. Aluminum further interferes with the parathyroid gland and with calcium handling, compounding the bone problem.
Interfering with iron handling and red-blood-cell production
Because aluminum competes with iron for transferrin and for cellular iron-binding sites, it can hijack iron's pathways and impair the use of iron in making hemoglobin. This produces a microcytic anemia (small, pale red cells) that can look like iron-deficiency anemia but does not improve with iron, and that contributes to resistance to erythropoietin, the hormone used to treat anemia in dialysis patients.
Neuronal disruption and oxidative stress
In the brain, aluminum is thought to interfere with the normal signaling and metabolism of nerve cells, disturb the handling of phosphate-containing molecules essential to brain energy and structure, and promote oxidative stress — an excess of reactive, tissue-damaging molecules. Although aluminum is not a classic Fenton-reaction metal like iron or copper, it can amplify oxidative damage indirectly and may promote the aggregation of certain brain proteins in laboratory studies. These mechanisms underlie the encephalopathy seen in severe overload. Whether they contribute to common, age-related Alzheimer's disease is a separate and unsettled question, addressed below.
The unifying theme is mimicry and obstruction: aluminum slips into systems built for other metals and jams them, with the visible damage appearing wherever it concentrates most — bone, blood, and brain.
5. Symptoms & Health Effects
Aluminum toxicity is overwhelmingly a chronic problem of slow accumulation in vulnerable people, not a sudden poisoning. It is useful, though, to separate the rare acute picture from the classic chronic syndromes, and to think about chronic toxicity organ system by organ system.
Acute toxicity
True acute aluminum poisoning is uncommon. It is seen mainly when a large amount of soluble aluminum enters the bloodstream over a short period — for example, contaminated dialysis fluid, or accidental high intravenous exposure. The picture can include rapidly worsening confusion, agitation, slurred or halting speech, muscle twitching or jerks (myoclonus), and seizures, sometimes progressing to coma. A sudden, large oral exposure in people with normal kidneys — as in the Camelford water incident — more often produces transient gastrointestinal upset and a constellation of neurological and general complaints that are harder to interpret. Acute heavy inhalation at work can cause respiratory irritation and, with extreme exposure, lung injury.
Chronic toxicity by organ system
The classic targets of long-term aluminum overload — almost always in the setting of kidney failure — are bone, brain, and blood.
Bone (the skeleton)
- Aluminum bone disease takes two main forms: osteomalacia (soft, poorly mineralized bone) and adynamic bone disease (bone that has nearly stopped remodeling).
- Symptoms include deep, persistent bone pain (often in the back, ribs, and hips), muscle weakness, difficulty walking, and a markedly increased risk of fractures from minor trauma. Fractures may heal slowly.
- This bone disease can be painful and disabling, and historically was a leading cause of suffering in long-term dialysis patients before aluminum exposure was controlled.
Brain and nervous system
- Dialysis encephalopathy (“dialysis dementia”) is the hallmark of severe chronic brain involvement. It typically begins with a distinctive speech disturbance (stuttering, hesitancy, difficulty finding words), then progresses to memory loss, personality change, disorientation, muscle jerks (myoclonus), seizures, and ultimately profound dementia. Before its cause was understood, it was usually fatal.
- Milder cognitive slowing and concentration problems can occur with lesser degrees of overload.
Blood and bone marrow
- Microcytic anemia — small, pale red cells producing fatigue, pallor, and breathlessness — that characteristically does not respond to iron and that worsens resistance to erythropoietin therapy in dialysis patients.
Two questions people ask most
Does aluminum in antiperspirant cause breast cancer?
This is a common and understandable worry, fueled by the fact that antiperspirants are applied near breast tissue. The reassuring answer from the research is no: large epidemiologic studies have not found that antiperspirant or deodorant use causes breast cancer, and major cancer organizations do not consider it a risk factor. There is no established causal link. (Laboratory studies on aluminum and breast cells exist and keep the topic under study, but they do not amount to evidence that everyday antiperspirant use causes cancer in people.)
Does aluminum cause Alzheimer's disease?
This idea has a long and complicated history. Early hypotheses arose decades ago from observations that aluminum could be found in the brains of people with Alzheimer's, from the brain damage seen in dialysis encephalopathy, and from some ecological studies linking aluminum in drinking water to dementia rates. Presented honestly: the overall body of evidence does not establish aluminum as a cause of Alzheimer's disease. The mainstream scientific position is that an aluminum cause is not proven; the studies are inconsistent, often confounded, and have not demonstrated that ordinary aluminum exposure causes the disease. Aluminum remains a topic of legitimate ongoing research, but it should not be presented to the public as a confirmed cause of Alzheimer's.
6. Diagnosis & Laboratory Testing
Diagnosing aluminum toxicity combines the clinical picture (who is at risk and what symptoms they have) with specific laboratory tests. Because aluminum is everywhere in the environment and in laboratory equipment, samples must be collected in special aluminum-free (trace-element) tubes to avoid falsely high readings — a real and common pitfall.
Serum (blood) aluminum
The first-line test is a serum aluminum level, drawn in a trace-metal tube. Approximate reference ranges (laboratories vary, so always use your lab's stated ranges and units):
- Normal, healthy person: typically below about 5–10 µg/L (micrograms per liter; some labs report in µg/dL, where the numbers are 10× smaller).
- Dialysis patients — target/acceptable: guidelines generally aim to keep levels under about 20 µg/L.
- Concerning / suggests accumulation: roughly 20–60 µg/L — prompts investigation and source removal.
- Toxic / overload range: generally above 60–100 µg/L, with the risk of symptomatic bone and brain disease rising as levels climb higher.
An important limitation: a single blood level reflects recent exposure and circulating aluminum, but most of the body's aluminum is locked away in bone and tissue, so a near-normal blood level does not rule out a large stored body burden. That is exactly why the next two tests exist.
24-hour urine aluminum
A 24-hour urine aluminum collection measures how much aluminum the body is excreting and helps gauge recent exposure, particularly in people with working kidneys (it is less useful in dialysis patients, who make little urine). It is interpreted alongside the blood level and the clinical history.
The deferoxamine (DFO) challenge test
To uncover hidden aluminum stored in bone and tissue — the burden a resting blood level can miss — doctors use the deferoxamine (DFO) challenge test. Deferoxamine is a drug that binds aluminum and pulls it out of tissues into the blood. In the test, a measured dose of DFO is given (for dialysis patients, often during or before a dialysis session), and the serum aluminum is measured before and after (commonly a baseline level and a level drawn a set interval later, such as before the next dialysis session). A large rise in serum aluminum after DFO indicates a significant stored body burden — in essence, the drug “flushes out” hidden aluminum so it becomes measurable. The size of the increase guides both diagnosis and treatment decisions. (Because DFO can have side effects and can even provoke neurological symptoms in heavily loaded patients, the test is done carefully and under supervision.)
Bone biopsy — the definitive test for bone disease
The most definitive way to diagnose aluminum bone disease is a bone biopsy (usually from the iliac crest, the rim of the hip bone) with special aluminum staining (such as aluminon or solochrome azurine stains). Aluminum is seen lining the mineralization front, and the pattern distinguishes aluminum-related osteomalacia and adynamic bone disease from other forms of renal bone disease. Because biopsy is invasive, it is reserved for cases where the diagnosis is unclear or treatment decisions depend on it; many patients are managed on the basis of history, blood levels, and the DFO challenge.
Supporting tests
Doctors also look at the whole picture: a complete blood count may show microcytic anemia; iron studies help separate aluminum-related anemia from true iron deficiency; kidney function tests confirm the at-risk setting; and parathyroid hormone (PTH) is checked because aluminum bone disease often coexists with — and must be distinguished from — the bone disease of secondary hyperparathyroidism.
7. Treatment & Management
Treatment rests on three pillars: stop the aluminum coming in, remove what is already stored, and support the kidneys' replacement (dialysis) so it is not itself a source.
1. Remove the source
The first and most important step is to identify and stop the exposure. In practice this means discontinuing aluminum-containing antacids and phosphate binders and switching to aluminum-free alternatives (calcium-based, sevelamer, or lanthanum binders), and for infants, using parenteral nutrition components with low aluminum content. For many people with milder accumulation and functioning kidneys, simply removing the source allows the body to slowly clear aluminum on its own.
2. Ensure dialysate purity
For dialysis patients, the dialysis machine's water must be scrupulously clean. Modern units use reverse osmosis and deionization and routinely test the water, keeping aluminum in the dialysate to very low levels (commonly under 10 µg/L). Getting this right was the decisive intervention that ended the dialysis-encephalopathy epidemic, and maintaining it prevents recurrence. This is as much a treatment as any drug, because it removes the largest historical source.
3. Chelation with deferoxamine (DFO)
For patients with symptomatic aluminum overload — bone disease, encephalopathy, or aluminum-related anemia, typically in the setting of renal failure — the specific treatment is chelation with deferoxamine. Deferoxamine binds aluminum to form a complex (aluminoxamine) that is larger and water-soluble; this complex can then be removed from the blood during dialysis (modern high-flux dialyzers or specialized adsorption columns clear it). Treatment is given in repeated cycles, often weekly, over months, with the serum aluminum (and DFO-challenge response) tracked to judge progress. As stored aluminum is removed, bone pain and anemia can improve and, if caught early enough, neurological decline may stabilize.
Deferoxamine is a powerful drug and is used carefully. It can cause low blood pressure during infusion, eye and hearing effects with prolonged use, and — importantly — it can transiently worsen neurological symptoms in heavily loaded patients by mobilizing aluminum, and it raises the risk of certain serious infections. For these reasons, dosing has shifted toward lower, carefully titrated regimens rather than the high doses once used, and treatment is supervised by a nephrology team.
4. Supportive care
Alongside source removal and chelation, patients receive supportive treatment for the consequences of overload: pain management and fracture care for bone disease; correction of mineral and parathyroid abnormalities; and management of anemia (which often improves as aluminum is removed and erythropoietin works better). Neurological symptoms are managed supportively, with the understanding that prevention — not waiting for symptoms — is far more effective than rescue once severe encephalopathy has set in.
8. Prevention & Risk Reduction
The most encouraging fact about aluminum toxicity is that it is largely preventable, and the public-health measures that prevent it have already worked dramatically. Prevention is matched to the level of risk.
For people with healthy kidneys (almost everyone)
If your kidneys work normally, you do not need to fear ordinary aluminum exposure. Cooking in aluminum pans, using foil, drinking from cans, eating foods with aluminum-based additives, and using antiperspirants are not known to cause aluminum toxicity, because your gut absorbs little and your kidneys clear the rest. Sensible, low-effort steps if you wish to reduce intake include not routinely cooking highly acidic foods (like tomato sauce) in bare aluminum for long periods, and not taking aluminum-containing antacids together with citrate-rich drinks. Beyond that, no special precautions are warranted for the general population.
For people with chronic kidney disease or on dialysis (the high-risk group)
- Avoid aluminum-containing phosphate binders and antacids unless a kidney specialist specifically prescribes them for a short, defined period; use calcium, sevelamer, or lanthanum binders instead.
- Insist that dialysis water is purified and monitored — this is standard in modern units, with aluminum kept very low (commonly under 10 µg/L).
- Have aluminum levels checked periodically as part of routine dialysis care, so accumulation is caught early, before symptoms appear.
- Be cautious with citrate (including some supplements and citrus juices) if also taking any aluminum-containing product, since citrate sharply increases aluminum absorption.
For vulnerable infants
Premature and sick newborns on intravenous nutrition are protected by using parenteral-nutrition components with documented low aluminum content, by following the FDA's limits on aluminum in these products, and by minimizing the duration of intravenous feeding where clinically possible.
For workers
People in aluminum smelting, potroom, and welding environments are protected by occupational exposure limits, engineering controls (ventilation, dust suppression), and respiratory protection, along with health surveillance where indicated.
The big-picture lesson
Severe aluminum toxicity is now uncommon precisely because it was understood and engineered out — aluminum was removed from dialysis water and from routine binders, and limits were set for infant nutrition. It is a reminder that the dose, the route, and the state of the kidneys — not the mere presence of aluminum in modern life — determine the risk.
9. Related Topics
- Heavy Metals: An Overview of Toxic Metal Exposure
- Chronic Kidney Disease (the key high-risk setting for aluminum overload)
- Phosphorus and Phosphate Binders
- Alzheimer's Disease (and the unproven aluminum hypothesis)
- Osteoporosis and Bone Health
- Anemia (including microcytic anemia)
- Lab Tests: Blood and Urine Testing
10. Key Research Papers
- Alfrey AC, LeGendre GR, Kaehny WD. The Dialysis Encephalopathy Syndrome. New England Journal of Medicine. 1976;294(4):184-188.
- Alfrey AC. Dialysis Encephalopathy Syndrome. Annual Review of Medicine. 1978;29(1):93-98.
- Andress DL, Maloney NA, Coburn JW. Aluminum Bone Disease in Chronic Renal Failure. Seminars in Dialysis. 1990;3(1):27-32.
- Drüeke TB. Adynamic bone disease, anaemia, resistance to erythropoietin and iron–aluminium interaction. Nephrology Dialysis Transplantation. 1993;8(suppl 1):12-16.
- Kan WC, Chien CC, Wu CC, et al. Comparison of low-dose deferoxamine versus standard-dose deferoxamine for treatment of aluminium overload among haemodialysis patients. Nephrology Dialysis Transplantation. 2009;25(5):1604-1608.
- Altmann P, Cunningham J, Dhanesha U, et al. Disturbance of cerebral function in people exposed to drinking water contaminated with aluminium sulphate: retrospective study of the Camelford water incident. BMJ. 1999;319(7213):807-811.
- Moreno A, Domínguez C, Ballabriga A. Aluminium in the neonate related to parenteral nutrition. Acta Paediatrica. 1994;83(1):25-29.
- Krewski D, Yokel RA, Nieboer E, et al. Human Health Risk Assessment for Aluminium, Aluminium Oxide, and Aluminium Hydroxide. Journal of Toxicology and Environmental Health, Part B. 2007;10(suppl 1):1-269.
- Mirick DK, Davis S, Thomas DB. Antiperspirant Use and the Risk of Breast Cancer. Journal of the National Cancer Institute. 2002;94(20):1578-1580.
- Exley C. The Chemistry of Human Exposure to Aluminium. Advances in Experimental Medicine and Biology. 2018;1091:33-37.
- Exley C, House E. The coordination chemistry of aluminium in neurodegenerative disease. Coordination Chemistry Reviews. 2012;256(19-20):2142-2146.
- Agency for Toxic Substances and Disease Registry (ATSDR). Toxicological Profile for Aluminum. U.S. Department of Health and Human Services. Full profile (PDF).
- U.S. National Library of Medicine, MedlinePlus. Aluminum (overexposure and toxicity). MedlinePlus Medical Encyclopedia.
- U.S. Environmental Protection Agency (EPA). Secondary Drinking Water Standards: Guidance for Nuisance Chemicals (aluminum 0.05–0.2 mg/L). EPA guidance.
- U.S. Occupational Safety and Health Administration (OSHA). Aluminum — Chemical Sampling Information. OSHA occupational data.
Connections
- All Toxic Minerals
- Heavy Metals Overview
- Lead Toxicity
- Mercury Toxicity
- Cadmium Toxicity
- Arsenic Toxicity
- Fluoride
- All Minerals
- Phosphorus
- Calcium
- Iron
- Magnesium
- Chronic Kidney Disease
- Alzheimer's Disease
- Anemia
- Lab Tests