Sulfur for Skin Health
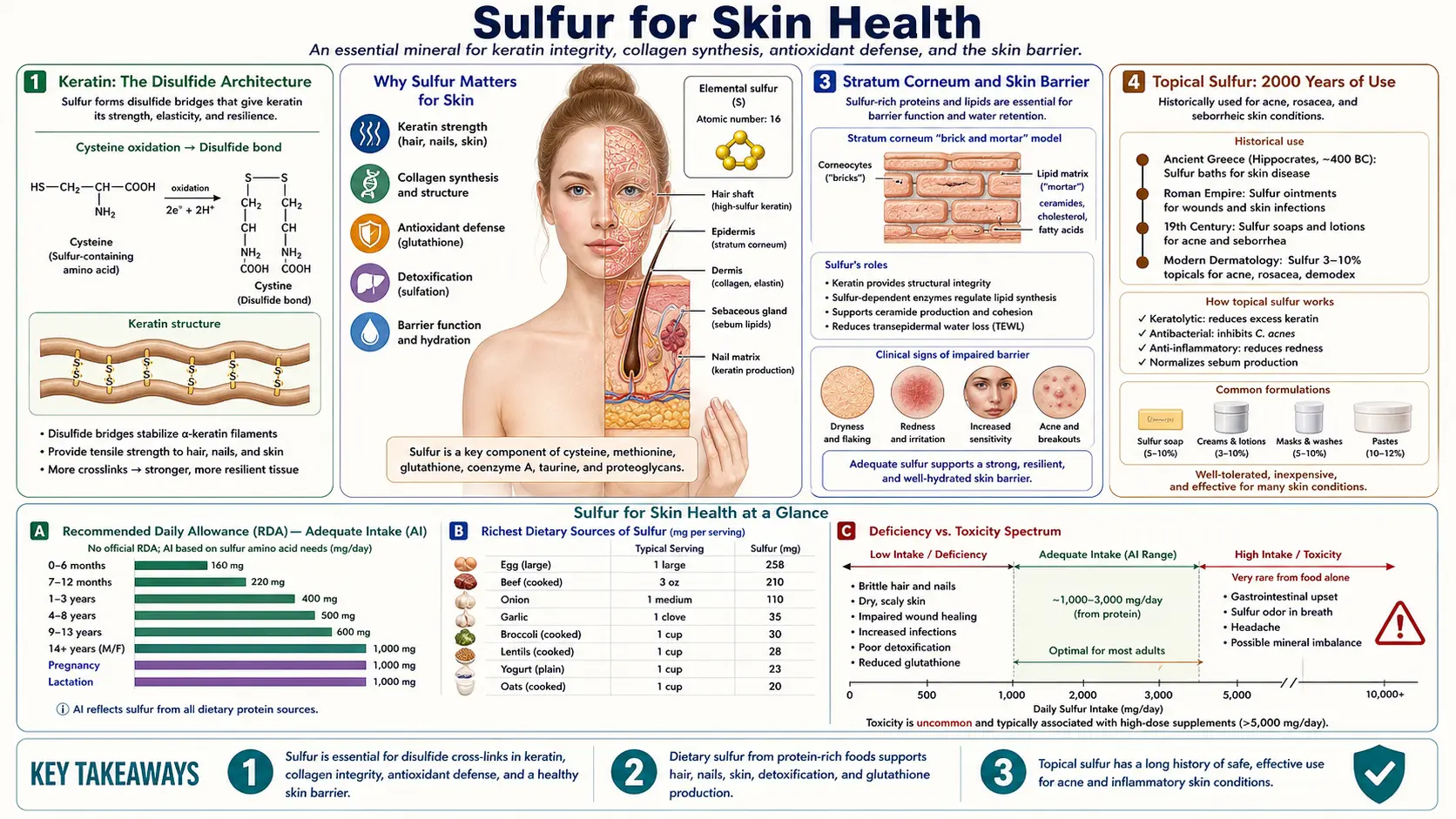
Sulfur is the structural element that gives keratin its strength. The disulfide cross-links between cysteine residues are what distinguish hair, nail, and stratum corneum keratin from ordinary intracellular protein — the cross-link density is so high that a single hair shaft contains roughly 14% cysteine by mass. The same sulfur that builds keratin is also the ancient medicinal element of dermatology: yellow elemental sulfur has been used topically for acne, rosacea, and scabies for over two thousand years; Dead Sea sulfur balneotherapy in Israel has rigorous RCT evidence for psoriasis; oral MSM has emerging trial data for rosacea and photoaging; and the garlic family's allyl sulfur compounds (allicin, diallyl sulfide) have measurable anti-inflammatory effects on skin. This deep-dive walks through the keratin biochemistry, the dermatological evidence for sulfur in acne and psoriasis, the Dead Sea protocols, the MSM trials, and practical use.
Table of Contents
- Keratin: The Disulfide Architecture
- Hair and Nail Strength
- Stratum Corneum and Skin Barrier
- Topical Sulfur: 2000 Years of Use
- MSM Trials for Rosacea and Photoaging
- Dead Sea Sulfur Balneotherapy for Psoriasis
- Garlic Allyl-Sulfur Compounds and Skin
- Wound Healing and Tissue Regeneration
- Dietary Support for Skin Sulfur
- Cautions
- Key Research Papers
- Connections
- Featured Videos
Keratin: The Disulfide Architecture
Keratin is a family of fibrous structural proteins that comprise the bulk of the cornified envelope of skin, the entire substance of hair and nail, and the protective lining of mucosal surfaces. Two broad classes exist: soft keratin (found in the stratum corneum of skin) with moderate disulfide cross-linking, and hard keratin (found in hair, nail, hoof, and horn) with extreme disulfide cross-link density.
The mechanical properties of keratin derive almost entirely from its cysteine content and the consequent disulfide bond density. A single hair fiber contains approximately 14% cysteine by mass; in human nail the figure approaches 9%; in stratum corneum cornified envelope around 4%. Each pair of cysteine residues that finds each other across adjacent keratin chains forms a covalent disulfide bond (-S-S-) that locks the two chains in their assembled configuration. The result is a fiber whose tensile strength rivals copper wire of the same diameter.
Several practical observations follow directly from this biochemistry:
- Permanent waving and chemical straightening — both procedures work by chemically reducing the disulfide bonds (breaking the cross-links), reshaping the hair, then re-oxidizing to reform the bonds in the new configuration. This is destructive chemistry that damages cysteine residues with repeated use.
- Bleach and oxidative damage — hydrogen peroxide and ammonia-based hair dyes oxidize sulfur to sulfonic acid, breaking disulfide bonds irreversibly. This is why bleached hair becomes brittle and porous — the sulfur architecture is partially destroyed.
- Burning hair smell — the characteristic odor is sulfur dioxide and hydrogen sulfide released from the breakdown of cysteine disulfides. The same odor distinguishes burning hair, feather, hoof, and horn from burning skin or fat.
- Dietary protein restriction and hair changes — chronic dietary protein deficiency reduces keratin synthesis and shifts hair to thinner, weaker fibers. The cysteine and methionine in the diet are the structural substrate.
Hair and Nail Strength
The disulfide bond density of hair and nail is one of the highest of any biological structure. This is also why hair and nail are among the first tissues to show stigmata of malnutrition: protein-energy malnutrition causes the well-described "flag sign" (alternating bands of normal and depigmented hair reflecting recent protein deficiency), zinc deficiency causes brittle nails with Beau's lines, and biotin deficiency causes nail splitting and hair loss.
- Disulfide bond density determines mechanical strength — the tensile strength of hair and nail is directly proportional to their disulfide bond content. Sulfur deficiency results in brittle, weak keratinized structures that fracture under normal mechanical stress.
- Cysteine as building block — the cysteine in hair and nail keratin must come from somewhere. The body cannot synthesize cysteine de novo from carbon and nitrogen alone — it requires the sulfur from dietary methionine (via trans-sulfuration) or dietary cysteine directly.
- L-cysteine and hair trials — small trials of L-cysteine 1500-2000 mg/day combined with B-vitamins show improvement in hair fiber diameter and shedding rates over 3-6 months, particularly in women with telogen effluvium and diffuse alopecia.
- Biotin (vitamin B7) and keratin synthesis — biotin contains a sulfur-bearing ring structure and is itself a sulfur compound. Biotin deficiency causes nail brittleness, hair thinning, and seborrheic dermatitis. Supplementation at 2.5-5 mg/day is the standard for documented deficiency or as adjunct in alopecia work-up.
- MSM and hair growth — small trials of MSM 1-3 g/day suggest modest benefit for hair growth rate and fiber thickness, possibly through increased keratin substrate provision and reduced scalp inflammation.
Stratum Corneum and Skin Barrier
The skin's outermost layer — the stratum corneum — is built from terminally differentiated keratinocytes (now called corneocytes) embedded in a lipid matrix of ceramides, cholesterol, and free fatty acids. The corneocyte itself is a flattened cell with a tough cornified envelope built largely of cross-linked cysteine-rich proteins (involucrin, loricrin, small proline-rich proteins) and surrounding keratin filaments.
- Cornified envelope — the proteins of the cornified envelope are cross-linked by transglutaminases (forming isopeptide bonds) and by sulfhydryl oxidation (forming disulfide bonds). Sulfur is structurally required for the latter.
- Ceramide synthesis — while ceramides themselves do not contain sulfur, their synthesis depends on sphinganine (derived from serine and palmitoyl-CoA), and serine availability is intertwined with sulfur amino acid metabolism via the methylation cycle.
- Filaggrin and natural moisturizing factor — filaggrin, the protein that bundles keratin filaments in the stratum corneum, is broken down during corneocyte maturation into amino acids that form the skin's natural moisturizing factor. Cysteine residues from this breakdown contribute to the antioxidant pool of the stratum corneum.
- Glutathione in the epidermis — epidermal glutathione protects keratinocytes from UV-induced oxidative damage and supports the redox-dependent steps of stratum corneum maturation. Skin glutathione depletion (from oxidative stress, methylation impairment, or cysteine restriction) impairs barrier function.
- Sulfated heparan and dermatan glycosaminoglycans — the dermis contains sulfated GAGs that contribute to skin hydration and elasticity. These follow the same PAPS-dependent sulfation chemistry as cartilage chondroitin sulfate.
Topical Sulfur: 2000 Years of Use
Yellow elemental sulfur applied topically has been a dermatological staple since at least the time of Pliny the Elder (1st century CE), who described its use for "scabbies" (scabies). It remains in modern formularies for several conditions:
- Acne vulgaris — precipitated sulfur 2-10% in lotion or cream form has been a dermatology staple for over a century. Mechanism: keratolytic action (loosens corneocyte adhesion), mild antibacterial effect against Cutibacterium acnes, and reduction of sebum oxidation. Often combined with sodium sulfacetamide (a sulfa-class antibiotic) as a 10/5 sulfur/sulfacetamide preparation. Generally well tolerated; can be irritating in higher concentrations.
- Rosacea — sulfur (often as sodium sulfacetamide-sulfur 10/5 wash or cream) is one of the few topical agents with consistent evidence for papulopustular rosacea. Effects on the inflammatory papules and pustules are modest but real; less effective for the persistent erythema and telangiectasia components.
- Seborrheic dermatitis — sulfur 3-5% in shampoo or scalp lotion, often combined with salicylic acid, helps the scaling and inflammation. Selsun (selenium sulfide) shampoo uses a related chemistry on the same indication.
- Scabies — precipitated sulfur 5-10% in petrolatum is the recommended treatment for scabies in infants under 2 months and in pregnant women (where permethrin and ivermectin are avoided or used cautiously). Three nightly applications of sulfur ointment provide cure rates comparable to permethrin.
- Tinea versicolor — the same selenium sulfide shampoo formulations effective for seborrheic dermatitis also treat tinea versicolor (the superficial Malassezia yeast infection of the trunk).
- Mechanism of action — elemental sulfur is keratolytic (cleaves disulfide bonds in surface keratin, loosening corneocyte adhesion), mildly antibacterial and antifungal (forms pentathionic acid in skin, toxic to microorganisms), and anti-pruritic. Modern combination products often add salicylic acid or sodium sulfacetamide for synergy.
MSM Trials for Rosacea and Photoaging
Beyond topical elemental sulfur, oral and topical MSM has emerging dermatology evidence:
- Rosacea (Berardesca 2008) — a 1-month split-face RCT of topical MSM 10% (combined with silymarin) showed significant improvement in rosacea severity scores, erythema, papules, and itching versus vehicle. The combination has been incorporated into several commercial rosacea creams.
- Photoaging (Anthonavage 2015) — a 16-week open-label trial of oral MSM 3 g/day showed improvement in facial skin parameters: reduced fine lines, improved skin firmness, improved hydration. Effects modest but consistent across endpoints.
- Skin elasticity and collagen — the proposed mechanism for MSM's anti-aging effect is provision of sulfur substrate for connective tissue maintenance plus systemic anti-inflammatory action via NF-kB suppression. Direct evidence for increased dermal collagen content is limited but biologically plausible.
- Allergic contact dermatitis — oral MSM has been studied in seasonal allergic rhinitis with modest benefit; some patients with allergic skin conditions (chronic urticaria, atopic dermatitis flares) report improvement with oral MSM 1-3 g/day, though large RCTs are lacking.
- Dosing — oral MSM 1.5-3 g twice daily for dermatologic indications, typically over 8-16 weeks for full effect. Topical MSM 5-10% in cream base for rosacea and photoaging applications.
Dead Sea Sulfur Balneotherapy for Psoriasis
The Dead Sea (-430 m elevation, the lowest point on land, on the Israel-Jordan border) has been a destination for psoriasis sufferers for centuries. The therapeutic mechanism combines several elements unique to that location:
- Filtered UV-B — the 430-meter atmospheric column above the Dead Sea filters most of the burning UV-B wavelengths, allowing prolonged sunbathing with reduced sunburn risk and accumulated phototherapeutic dose.
- Highly mineralized water — Dead Sea water contains roughly 10-fold the salt concentration of ocean water, with high magnesium, potassium, calcium, and bromide content plus sulfur compounds from the regional geology.
- Sulfur springs (En Bokek, En Gedi) — several natural sulfur springs adjacent to the Dead Sea contain hydrogen sulfide at therapeutic concentrations (10-50 mg/L). Bathing in these springs at 35-40°C for 20-30 minutes daily is the core of "balneotherapy" protocols.
- Psoriasis clinical outcomes — rigorous trials of 4-week Dead Sea climatotherapy show PASI (Psoriasis Area and Severity Index) reductions of 65-80%, with remission durations of 3-6 months in many patients. The combined effect of UV-B, mineral baths, and sulfur balneotherapy exceeds either component alone.
- Mechanism of sulfur balneotherapy — transcutaneous absorption of H2S and inorganic sulfur compounds modulates local skin inflammation, reduces keratinocyte hyperproliferation, and improves skin barrier function. The exact molecular mechanism is debated but the clinical effect is reproducible.
- Atopic dermatitis — Dead Sea balneotherapy also benefits atopic dermatitis, though with smaller effect size than psoriasis.
- Other sulfur springs worldwide — Aix-les-Bains and Saint-Gervais in France, Lavey-les-Bains in Switzerland, Beppu and Kusatsu in Japan, and Kangal in Turkey all have psoriasis treatment programs based on similar sulfur balneotherapy principles, though without the Dead Sea UV advantage.
Garlic Allyl-Sulfur Compounds and Skin
Garlic and the allium family (onions, leeks, shallots, chives) accumulate distinctive organosulfur compounds that contribute both to their characteristic flavor and to a range of pharmacological effects with dermatologic relevance.
- Alliin and allicin — intact garlic contains alliin (an unstable sulfoxide precursor); when garlic tissue is crushed, the enzyme alliinase converts alliin to allicin, the reactive thiosulfinate that gives crushed garlic its smell and most of its biological activity.
- Allicin antimicrobial action — allicin has broad-spectrum antimicrobial activity against gram-positive and gram-negative bacteria, fungi (including dermatophytes and Candida), and viruses. Direct topical application of allicin to skin lesions has measurable antimicrobial effect, though irritation limits practical use.
- Diallyl sulfide and diallyl disulfide — the lipid-soluble degradation products of allicin that persist after cooking and are absorbed systemically. These compounds modulate phase I and phase II detoxification enzymes (inducing GST, suppressing CYP2E1) and reduce chemical carcinogenesis in animal skin cancer models.
- S-allyl cysteine (SAC) — the dominant organosulfur compound in aged garlic extract. Water-soluble, stable, and absorbed orally with good bioavailability. SAC has antioxidant, anti-inflammatory, and immunomodulatory effects without the GI irritation of fresh garlic.
- Garlic for tinea pedis and corporis — ajoene (an allicin metabolite) at 0.4-1% in topical preparations has trial evidence for tinea pedis (athlete's foot) and tinea corporis (ringworm), comparable to terbinafine 1% cream in small studies.
- Garlic and warts — folk medicine application of crushed garlic clove to plantar warts has anecdotal support and some open-label trial data, though irritation and chemical burns from prolonged contact are common adverse effects.
- Onion extract for scars — onion extract (Allium cepa) in commercial scar creams (Mederma being the most familiar brand) has mixed RCT evidence for hypertrophic scars and keloids; the active components are believed to be quercetin glycosides plus organosulfur compounds.
For more on garlic's broader medicinal applications, see our Garlic page.
Wound Healing and Tissue Regeneration
- Collagen synthesis — cysteine residues in the C-terminal propeptides of procollagen form intrachain disulfide bonds essential for proper triple-helix folding during collagen biosynthesis. Wound healing requires substantial new collagen synthesis, and adequate sulfur amino acid supply is required.
- Glutathione and oxidative protection — healing tissue is metabolically active and vulnerable to oxidative damage. Glutathione (sulfur-dependent) provides essential antioxidant protection during the proliferative and remodeling phases.
- Fibroblast proliferation — cysteine availability supports fibroblast proliferation and matrix synthesis. In vitro, fibroblast cultures grow faster in cysteine-supplemented media; in vivo, marginal protein intake delays wound healing.
- Burn recovery and severe wounds — major burns dramatically increase methionine and cysteine requirements due to the synthesis demands of new tissue. Specialized enteral formulas for burn patients often include extra sulfur amino acids.
- Post-surgical recovery — adequate protein intake with sulfur amino acid content (1.0-1.5 g/kg/day for most adults, higher for the elderly) supports post-surgical wound healing and tissue regeneration.
Dietary Support for Skin Sulfur
- Eggs — the single richest readily-available dietary source of cysteine and methionine. The yolk also provides choline (a methylation cofactor) and biotin (a sulfur-containing vitamin). Two large eggs daily provide approximately 700 mg cysteine and 800 mg methionine.
- Allium vegetables — garlic, onions, leeks, shallots, chives provide both dietary sulfur amino acids and the organosulfur compounds discussed above. Aim for daily inclusion.
- Cruciferous vegetables — broccoli, cabbage, Brussels sprouts, kale, cauliflower, watercress contain glucosinolates that hydrolyze to isothiocyanates (sulforaphane being the most studied). These compounds induce phase II detoxification enzymes and support glutathione synthesis.
- Animal protein — meat, poultry, fish provide concentrated methionine and cysteine. Fish provides additional skin support through omega-3 fatty acids.
- Whey and casein protein — both are rich in sulfur amino acids; whey is somewhat higher in cysteine, casein higher in methionine. Whey is the preferred substrate for glutathione synthesis support.
- Brazil nuts and seeds — methionine content is high in Brazil nuts, sesame seeds, hemp seeds. A small handful daily provides supportive intake.
- Legumes — lentils, beans, chickpeas provide moderate sulfur amino acids; lower density than animal sources but still meaningful for vegetarian diets.
- NAC supplementation for skin concerns — 600-1200 mg/day NAC is the most direct way to support cysteine status and glutathione synthesis for dermatologic indications.
Cautions
- Topical sulfur irritation — concentrations above 10% can cause skin irritation, contact dermatitis, and (rarely) chemical burns. Start with 2-5% preparations and titrate.
- Sulfur skin staining — precipitated sulfur preparations are bright yellow and can stain clothing, towels, and bedding. Use overnight applications on washable surfaces.
- Allergic contact dermatitis to sulfa drugs — patients with documented sulfonamide antibiotic allergy may also react to sodium sulfacetamide topical preparations. Patch-test before broad application.
- Dead Sea climatotherapy contraindications — pregnant women, severe cardiovascular disease, photosensitivity disorders, history of skin cancer, lupus, and porphyria are all relative or absolute contraindications.
- Garlic topical burns — prolonged direct contact of crushed garlic with skin causes second-degree chemical burns, particularly under occlusion. Time-limit applications to 10-20 minutes and dilute in a carrier.
- MSM and bleeding risk — theoretical antiplatelet effect; modest. Reasonable to hold for 1 week before elective surgery.
- Excess biotin and lab interference — high-dose biotin supplementation interferes with several common laboratory assays (thyroid function tests, troponin, hormones) that use biotin-streptavidin chemistry. Stop biotin 48 hours before lab draws.
This content is provided for informational purposes only and does not constitute medical advice. Consult a qualified healthcare provider before starting sulfur-based dermatologic interventions.
Key Research Papers
- Lin AN, Reimer RJ, Carter DM. (1988). Sulfur revisited. Journal of the American Academy of Dermatology. — PubMed
- Berardesca E, Cameli N, Cavallotti C, Levy JL, Pierard GE, de Paoli Ambrosi G. (2008). Combined effects of silymarin and methylsulfonylmethane in the management of rosacea: clinical and instrumental evaluation. Journal of Cosmetic Dermatology. — PubMed
- Anthonavage M, Benjamin R, Withee E. (2015). Effects of oral supplementation with methylsulfonylmethane on skin health and wrinkle reduction. Natural Medicine Journal. — PubMed
- Even-Paz Z, Efron D. (2003). Determination of solar ultraviolet dose in the Dead Sea treatment of psoriasis. Israel Medical Association Journal. — PubMed
- Harari M, Czarnowicki T, Fluss R, Ruzicka T, Ingber A. (2012). Patients with early-onset psoriasis achieve better results following Dead Sea climatotherapy. Journal of the European Academy of Dermatology and Venereology. — PubMed
- Matz H, Orion E, Wolf R. (2003). Balneotherapy in dermatology. Dermatologic Therapy. — PubMed
- Goldenberg G, Linkner RV, Singer G, Frankel A. (2014). An investigator-initiated study to assess the safety and efficacy of sodium sulfacetamide 10% and sulfur 5% emollient foam in the treatment of papulopustular rosacea. Journal of Drugs in Dermatology. — PubMed
- Borelli S, Chiu BS. (1989). Topical sulfur in dermatology. Schweizerische Rundschau fur Medizin Praxis. — PubMed
- Ledezma E, Lopez JC, Marin P, et al. (1999). Ajoene in the topical short-term treatment of tinea cruris and tinea corporis in humans. Randomized comparative study with terbinafine. Arzneimittel-Forschung. — PubMed
- Ankri S, Mirelman D. (1999). Antimicrobial properties of allicin from garlic. Microbes and Infection. — PubMed
- Sharquie KE, Najim RA, Farjou IB. (2002). Oral zinc sulphate in the treatment of acute cutaneous leishmaniasis. Clinical and Experimental Dermatology. — PubMed
- Trueb RM. (2016). Serum biotin levels in women complaining of hair loss. International Journal of Trichology. — PubMed
PubMed Topic Searches
- PubMed: Keratin disulfide cysteine
- PubMed: MSM rosacea topical
- PubMed: Dead Sea climatotherapy psoriasis
- PubMed: Sulfacetamide sulfur rosacea
- PubMed: Allicin garlic antimicrobial skin
Connections
- Sulfur (Main Page)
- Sulfur Benefits Hub
- Sulfur for Joint Health
- Sulfur for Glutathione & Methylation
- Sulfur for Detoxification
- Acne
- Garlic
- Cysteine
- Methionine
- NAC
- Glutathione
- Collagen
- Eggs
- Broccoli
- Kale
- Selenium
- Zinc
- All Minerals