Sulfur for Detoxification
Phase II detoxification has six chemistries — glucuronidation, sulfation, methylation, glutathione conjugation, acetylation, and amino acid conjugation — and three of the six depend directly on sulfur. The SULT family of sulfotransferase enzymes uses PAPS (3'-phosphoadenosine-5'-phosphosulfate) as the universal sulfate donor for conjugation of acetaminophen, steroid hormones, dopamine, thyroxine, neurotransmitters, and hundreds of xenobiotics. The GST family of glutathione S-transferases uses cysteine-bearing glutathione as conjugation substrate. The methylation pathway consumes SAMe, itself derived from the sulfur amino acid methionine. When dietary sulfur is marginal, when MTHFR variants slow methionine synthesis, or when xenobiotic load overwhelms PAPS production, the entire phase II system bottlenecks. This deep-dive walks through SULT enzymology, the PAPS supply chain, the specific drug and hormone sulfation reactions that matter clinically, the sulfation pathway bottleneck in autism documented by Rosemary Waring, and the gasotransmitter signaling roles of hydrogen sulfide.
Table of Contents
- Phase I vs Phase II Detoxification
- The SULT Family of Sulfotransferase Enzymes
- PAPS: The Universal Sulfate Donor
- Drug Sulfation: Acetaminophen, Steroids, Thyroxine
- Neurotransmitter Sulfation: Dopamine, Catecholamines
- Glutathione S-Transferases (GST)
- The Sulfation Bottleneck in Autism (Waring)
- Hydrogen Sulfide Gasotransmitter Signaling
- Clinical Applications and Support Protocols
- Cautions
- Key Research Papers
- Connections
- Featured Videos
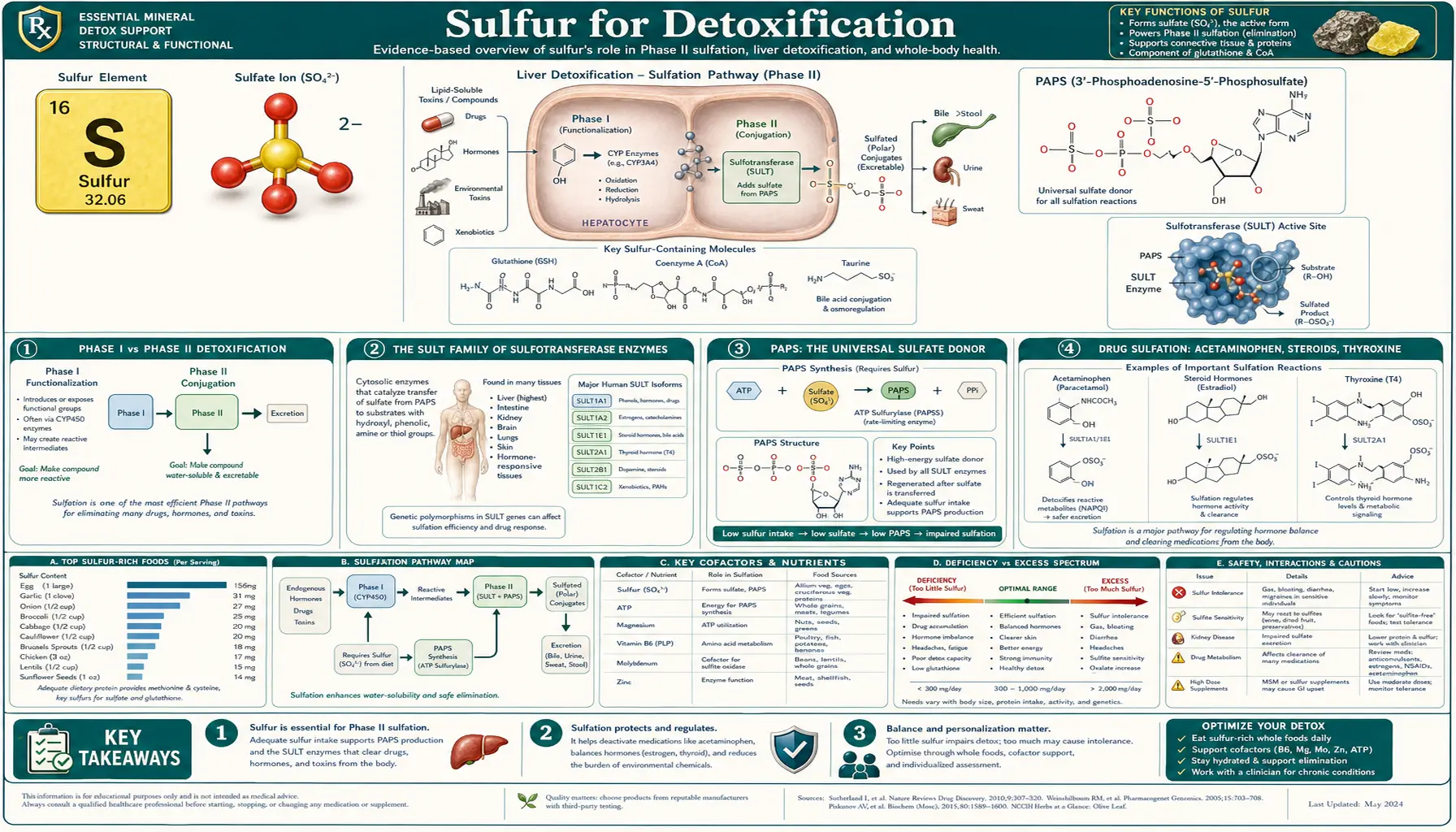
Phase I vs Phase II Detoxification
The classical model of xenobiotic metabolism divides the process into two phases. Phase I (functionalization) adds a polar functional group to lipophilic compounds — usually a hydroxyl group via cytochrome P450 oxidation, sometimes a reduction or hydrolysis. Phase I makes a compound chemically reactive (often more toxic than the parent compound). Phase II (conjugation) takes the phase I metabolite and conjugates it to a large, water-soluble carrier — sulfate, glucuronide, glutathione, glycine, taurine, or acetate — producing a non-reactive, water-soluble, excretable conjugate.
The interplay matters clinically. If phase I outpaces phase II, the reactive intermediates accumulate and cause oxidative damage. This is the mechanism of acetaminophen hepatotoxicity (CYP2E1 produces NAPQI faster than glutathione can conjugate it), of many chemical carcinogens (CYP1A1/1A2 activates polycyclic aromatic hydrocarbons faster than GST can quench them), and of "paradoxical" reactions to estrogen or drug exposures in patients with impaired sulfation or glutathione status.
The six phase II conjugation chemistries are:
- Glucuronidation (UGT enzymes, uses UDP-glucuronic acid)
- Sulfation (SULT enzymes, uses PAPS) — sulfur-dependent
- Methylation (methyltransferases, uses SAMe) — sulfur-dependent
- Glutathione conjugation (GST enzymes, uses glutathione) — sulfur-dependent
- Acetylation (NAT enzymes, uses acetyl-CoA)
- Amino acid conjugation (uses glycine, taurine, glutamine) — taurine is sulfur-derived
Three of the six chemistries (sulfation, methylation, glutathione conjugation) plus the taurine arm of amino acid conjugation all depend on adequate dietary sulfur. When sulfur is marginal, four of the six phase II pathways operate below capacity simultaneously.
The SULT Family of Sulfotransferase Enzymes
The cytosolic sulfotransferase (SULT) enzyme family in humans has 13 known members organized into four sub-families: SULT1 (phenolic, aromatic substrates), SULT2 (alcoholic, steroid substrates), SULT4, and SULT6. Each isoform has its preferred substrate spectrum and tissue distribution, and together they conjugate sulfate to hundreds of endogenous and exogenous compounds.
- SULT1A1 — the major hepatic phenol sulfotransferase. Conjugates acetaminophen, dopamine, 4-nitrophenol, 17-beta-estradiol, ethinyl estradiol, and numerous dietary phenolics (apigenin, quercetin, resveratrol). Highly polymorphic in human populations — the *2 variant has approximately 50% reduced activity.
- SULT1A3 and SULT1A4 — the catecholamine-specific sulfotransferases. Conjugate dopamine, norepinephrine, epinephrine, and the related catechol estrogens. SULT1A3 is the dominant gut and platelet isoform; SULT1A4 is enriched in brain.
- SULT1B1 — the thyroid hormone sulfotransferase. Conjugates T3 and reverse T3, an important pathway for thyroid hormone clearance.
- SULT1E1 — the estrogen sulfotransferase. The principal route for estrogen inactivation in liver, breast, and endometrium. SULT1E1 polymorphisms have been associated with breast cancer risk in some populations.
- SULT2A1 (DHEA-sulfotransferase) — conjugates DHEA to DHEA-sulfate, the most abundant circulating steroid in adult humans (DHEA-S serves as a reservoir from which active steroids can be regenerated by tissue-specific sulfatases).
- SULT2B1 — cholesterol and pregnenolone sulfotransferase. Important for cholesterol homeostasis and adrenal steroid metabolism.
- SULT4A1 — brain-specific, function not fully characterized; SULT4A1 knockout mice show neurological abnormalities.
PAPS: The Universal Sulfate Donor
All cytosolic SULT enzymes use a single high-energy sulfate donor: 3'-phosphoadenosine-5'-phosphosulfate (PAPS). PAPS is the "ATP-equivalent" for sulfation — analogous to how UDP-glucuronic acid is the activated donor for glucuronidation and SAMe is the activated donor for methylation.
PAPS is synthesized in two ATP-consuming steps from inorganic sulfate (SO42-):
- ATP sulfurylase activates inorganic sulfate to adenosine 5'-phosphosulfate (APS), consuming one ATP.
- APS kinase phosphorylates APS to PAPS, consuming a second ATP.
In mammals, both steps are catalyzed by a single bifunctional enzyme, PAPS synthase (PAPSS1 in most tissues, PAPSS2 in cartilage, skin, and adrenal). PAPSS2 loss-of-function mutations cause spondyloepimetaphyseal dysplasia (SEMD-PAPSS2 type), a recessive skeletal disorder with markedly reduced chondroitin sulfation in cartilage — direct human evidence for the essentiality of PAPS in connective tissue.
The inorganic sulfate that feeds PAPS synthesis comes from three sources:
- Trans-sulfuration of methionine and cysteine — the largest source under normal conditions. Cysteine is oxidized by cysteine dioxygenase to cysteine sulfinate, then by sulfinate decarboxylase to taurine OR by aspartate aminotransferase to 3-sulfinopyruvate, which spontaneously releases sulfite. Sulfite oxidase (a molybdenum-dependent enzyme) oxidizes sulfite to sulfate.
- Direct dietary sulfate — trace amounts in some mineral waters, brassica vegetables. Not significant clinically.
- Sodium sulfate ingestion — some functional medicine protocols use Epsom salt (magnesium sulfate) baths to deliver transcutaneous sulfate, though absorption data are limited and contested.
PAPS pools are small (sulfate is toxic at high concentrations, so storage is limited) and turnover is rapid. Any acute increase in sulfation demand — a paracetamol dose, an estrogen surge, a heavy meal of catecholamine-rich foods — transiently depletes PAPS and can saturate the sulfation pathway. This is one mechanism behind individual variation in drug clearance and hormone metabolism.
Drug Sulfation: Acetaminophen, Steroids, Thyroxine
- Acetaminophen (paracetamol) — metabolized by three parallel pathways: glucuronidation (50%), sulfation (30%), and CYP2E1 oxidation to NAPQI (5-10%, plus more under high-dose conditions). Sulfation is the dominant pathway in young children (the glucuronidation system matures slowly through childhood) — making PAPS supply particularly important for pediatric acetaminophen safety. When sulfation saturates (single doses above ~1 g in adults), the shift toward CYP2E1 oxidation increases NAPQI production. NAPQI is detoxified by glutathione conjugation; if glutathione is depleted, NAPQI binds hepatocyte proteins and causes hepatic necrosis. The entire safety architecture of acetaminophen rests on adequate sulfation + adequate glutathione status.
- Estrogens — 17-beta-estradiol, estrone, estriol, and their hydroxylated metabolites (2-OH-estradiol, 4-OH-estradiol, 16-OH-estradiol) are conjugated by SULT1E1 and SULT1A1 to sulfate esters that are inactive at estrogen receptors and excreted in urine and bile. The 4-OH-estradiol pathway is particularly important — 4-OH-estradiol is genotoxic (forms DNA adducts in breast tissue) and its rapid sulfation or methylation is protective against estrogen-driven carcinogenesis.
- Thyroxine (T4) and triiodothyronine (T3) — SULT1B1 conjugates thyroid hormones to T4-sulfate and T3-sulfate, the dominant route for thyroid hormone clearance in fetal and infant liver and a significant route in adults. Sulfated thyroid hormones are biologically inactive at thyroid receptors but can be deconjugated by tissue sulfatases as needed — making sulfation a reversible storage and regulatory mechanism, not just clearance.
- DHEA and DHEA-sulfate — SULT2A1 conjugates DHEA to DHEA-sulfate, creating the major circulating reservoir of adrenal steroid precursor. DHEA-S levels are roughly 1000-fold higher than free DHEA. Tissue sulfatases regenerate active DHEA locally as needed for downstream synthesis of testosterone, estradiol, and other steroids. DHEA-S is the steroid that declines most dramatically with aging — a marker of overall adrenal output and a frequent functional medicine target.
- Bile acids — secondary bile acids are sulfated by SULT2A1 as part of the enterohepatic recirculation regulation. Excess unsulfated bile acid accumulation contributes to hepatobiliary disease in some clinical scenarios.
- Minoxidil — the topical hair-growth drug requires conversion to minoxidil sulfate by SULT1A1 in the hair follicle to become active. Individuals with low SULT1A1 activity are minoxidil non-responders — one of the few documented "pharmacogenomic" failures based on sulfation phenotype.
Neurotransmitter Sulfation: Dopamine, Catecholamines
Dopamine, norepinephrine, and epinephrine are inactivated by two parallel routes: oxidative deamination by MAO (monoamine oxidase) and methylation by COMT (catechol-O-methyltransferase). The methylated metabolites are then sulfated by SULT1A3 to produce the dominant excreted metabolites (vanillylmandelic acid sulfate, homovanillic acid sulfate, normetanephrine sulfate, metanephrine sulfate).
- SULT1A3 and dopamine clearance — SULT1A3 is the dominant catecholamine sulfotransferase in human gut and platelets. It conjugates ingested dopamine (from fava beans, certain meats, banana peel) preventing it from entering systemic circulation — one reason fava beans cause minimal blood pressure effects in most people despite high L-dopa content. Individuals with SULT1A3 polymorphism plus MAO-A deficiency can have outsize pressor responses to dietary dopamine precursors.
- Catechol estrogen sulfation — the same SULT1A enzymes that handle catecholamines also conjugate catechol estrogens (2-OH-estradiol and 4-OH-estradiol). The competition between catecholamines and catechol estrogens for SULT and COMT has been hypothesized as one mechanism behind the "estrogen-PMS-catecholamine" symptom complex.
- Polyphenols and competitive inhibition — many dietary polyphenols (quercetin, resveratrol, EGCG, curcumin) are sulfated by SULT1A1. High intake of these compounds competitively inhibits sulfation of other substrates (acetaminophen, steroids), which can be a clinically significant drug-supplement interaction.
- Cholecystokinin sulfation — the gut hormone CCK requires tyrosine sulfation for full receptor activity. CCK-8 (the active octapeptide) is sulfated by a Golgi tyrosylprotein sulfotransferase, a different enzyme system from the cytosolic SULTs but still PAPS-dependent.
Glutathione S-Transferases (GST)
The glutathione S-transferase (GST) family conjugates electrophilic xenobiotics and endogenous reactive metabolites to glutathione, neutralizing their reactivity and generating water-soluble mercapturic acid derivatives for renal excretion. GSTs are the workhorse phase II enzymes for detoxifying chemical carcinogens, drug metabolites (NAPQI, ethylene oxide), and reactive products of lipid peroxidation (4-hydroxynonenal).
- GST classes — human cytosolic GSTs are grouped into eight classes (alpha, mu, pi, theta, zeta, omega, sigma, kappa). The most studied clinically are GSTM1, GSTT1, and GSTP1, all of which are polymorphic in human populations with significant impacts on chemical carcinogenesis susceptibility.
- GSTM1 null and GSTT1 null genotypes — complete gene deletion is common (GSTM1 null in 30-50% of populations; GSTT1 null in 10-25%). Null genotype carriers have measurably reduced detoxification capacity for substrates of those isoforms, with increased risk for some chemical carcinogenesis and increased susceptibility to acute oxidative injury.
- GST induction by sulforaphane — sulforaphane (from broccoli sprouts and cruciferous vegetables) is one of the most potent known inducers of GST and other phase II enzymes via Nrf2/Keap1/ARE activation. This is a major mechanism behind the chemopreventive effects of cruciferous vegetable consumption.
- Glutathione conjugation of NAPQI — the rapid GST-catalyzed conjugation of acetaminophen's reactive metabolite is the safety valve that prevents hepatic necrosis. NAC works by restoring the glutathione substrate for this reaction.
- Mercapturic acid biosynthesis — glutathione-xenobiotic conjugates are processed through gamma-glutamyl transpeptidase (removing glutamate), dipeptidase (removing glycine), and N-acetyltransferase (acetylating the remaining cysteine) to yield N-acetyl-cysteinyl-xenobiotic mercapturic acids that are excreted in urine.
The Sulfation Bottleneck in Autism (Waring)
Dr. Rosemary Waring at the University of Birmingham conducted a series of investigations from the 1990s through the 2010s documenting a striking pattern in children with autism spectrum disorders: significantly reduced sulfation capacity compared to typically developing children. The original observation was published in 1997 in Lancet (correspondence) and developed in subsequent papers.
- Reduced plasma sulfate — Waring's group documented that children with autism have plasma sulfate levels approximately 50% of typically developing controls.
- Reduced sulfation phenotype — using probe substrates like paracetamol (acetaminophen), Waring's group documented that autistic children sulfate the probe substrate at significantly reduced rates and shift conjugation toward the glucuronide pathway in compensation.
- PST (phenol sulfotransferase) deficiency hypothesis — Waring proposed that reduced PST (SULT1A1) activity, plus reduced plasma sulfate availability, plus reduced PAPS regeneration capacity, together created a "sulfation bottleneck" with downstream implications for catecholamine metabolism, phenol detoxification, and possibly gastrointestinal mucin sulfation (gut barrier integrity).
- Clinical implications proposed — sensitivity to acetaminophen (and a tentative link to acetaminophen exposure in early life), sensitivity to dietary phenols (food coloring, salicylates), altered catecholamine metabolism, altered estrogen and steroid handling, and increased gastrointestinal symptoms.
- Therapeutic protocols (functional medicine) — the Waring findings spawned a generation of functional medicine sulfation-support protocols: Epsom salt baths, MSM supplementation, methionine and cysteine optimization, B6/molybdenum support for the sulfite-oxidase step, and avoidance of high-phenol foods that compete for limited sulfation capacity.
- Independent confirmation status — the sulfation reduction finding has been independently replicated in several cohorts. The mechanistic causes (whether genetic, environmental, or both) remain incompletely characterized. The clinical implications and therapeutic value of the proposed support protocols remain debated.
- Broader implications — the Waring work raised the more general principle that population-level variation in sulfation capacity may explain individual variation in xenobiotic sensitivity, drug response, and environmental chemical tolerance — with implications well beyond autism.
Hydrogen Sulfide Gasotransmitter Signaling
Hydrogen sulfide (H2S) is best known as the toxic rotten-egg gas, lethal at high concentrations through cytochrome c oxidase inhibition. The biological revelation of the past 25 years is that the same molecule, at endogenous nanomolar concentrations, is one of three established gasotransmitters — freely-diffusing gaseous signaling molecules — alongside nitric oxide (NO) and carbon monoxide (CO).
- Endogenous synthesis — H2S is produced from cysteine by three enzymes: cystathionine beta-synthase (CBS), cystathionine gamma-lyase (CGL/CSE), and 3-mercaptopyruvate sulfurtransferase (3-MST). CBS dominates in brain and nervous system; CGL/CSE dominates in cardiovascular system and liver; 3-MST is widely distributed.
- Vascular signaling — endogenous H2S is a potent vasodilator, opening ATP-sensitive potassium channels (K-ATP) on vascular smooth muscle. Knockout of CSE in mice produces hypertension. H2S complements NO in cardiovascular tone regulation.
- Anti-inflammatory effects — H2S modulates NF-kB signaling, leukocyte adhesion, and the inflammatory cytokine cascade. Slow-release H2S donors are being developed as anti-inflammatory therapeutics.
- Mitochondrial effects — at very low concentrations, H2S supports mitochondrial respiration as an alternative electron donor at sulfide quinone reductase (SQR). At higher concentrations, it inhibits cytochrome c oxidase (the toxic mechanism). The therapeutic window matters.
- Gut microbiome production — sulfate-reducing bacteria (Desulfovibrio species) produce substantial H2S in the colon from dietary sulfate and sulfur amino acids. Excess H2S production has been implicated in some forms of inflammatory bowel disease and "sulfur intolerance" syndromes.
- Cellular signaling via persulfidation — H2S modifies protein cysteines by adding a sulfhydryl group (forming persulfides, -SSH), analogous to how phosphorylation modifies serine/threonine. This persulfidation is increasingly recognized as a major post-translational modification.
- Garlic and H2S — the cardiovascular benefits of garlic are partly explained by allicin-derived H2S production in vascular tissue. Diallyl trisulfide and other garlic organosulfides release H2S over hours, providing a sustained vasodilator effect.
Clinical Applications and Support Protocols
- Heavy metal chelation — sulfur-rich foods and supplements (cilantro, chlorella, NAC, MSM, glutathione) support the body's natural detoxification of heavy metals. Cysteine's thiol group has high affinity for mercury, cadmium, and lead. Formal chelation with DMSA or DMPS (both sulfur-containing) is the medical standard for documented heavy metal toxicity.
- Hormone metabolism optimization — sulfation supports clearance of estrogens, androgens, thyroid hormones, and corticosteroids. Cruciferous vegetables (DIM, indole-3-carbinol from broccoli), adequate methionine, B-vitamin sufficiency, and NAC support the integrated phase II hormone-handling system.
- Post-mold exposure recovery — mycotoxin clearance depends on glutathione conjugation and sulfation. NAC, glutathione, glycine, and methylation cofactor support are commonly used in functional medicine mold-illness protocols.
- Acetaminophen safety — chronic acetaminophen users (especially in the context of alcohol use, malnutrition, or pre-existing liver disease) benefit from NAC support to maintain glutathione reserves. Many clinicians recommend NAC 600 mg/day prophylactically for patients taking 2-4 g acetaminophen daily.
- Chemotherapy support — some chemotherapy agents (cisplatin, ifosfamide, cyclophosphamide) are protected against by sulfur amino acid support — though the timing matters because excessive glutathione during chemotherapy can also reduce drug efficacy. Coordination with oncology is essential.
- Epsom salt baths — magnesium sulfate baths (1-2 cups dissolved in warm bathwater, 20-30 minutes) are widely used in functional medicine for sulfur support, muscle relaxation, and detoxification. Transcutaneous absorption of sulfate has been documented in some studies, though the magnitude and clinical significance remain debated. Generally safe and pleasant, often included as adjunctive support.
- Sauna and sweat-mediated detoxification — some xenobiotics (BPA, certain pesticides, heavy metals) are excreted in sweat. The Niigata Minamata data suggest sweat heavy metal excretion can be a meaningful adjunct, particularly with concurrent sulfur amino acid optimization to support reabsorption-prevention via gut binding.
Cautions
- Sulfur intolerance syndrome — some patients (often with CBS gene variants, gut dysbiosis with sulfate-reducing bacteria overgrowth, or molybdenum deficiency) report symptoms (brain fog, headache, body odor, GI upset) with high sulfur intake. Pragmatic management: reduce dose, ensure molybdenum sufficiency (sulfite oxidase cofactor), test and treat SIBO if relevant.
- Hydrogen sulfide SIBO — a subset of SIBO patients have hydrogen-sulfide-producing bacterial overgrowth, identified by elevated H2S on a tri-smart breath test. These patients typically tolerate high-sulfur foods and supplements poorly. Management requires SIBO-specific treatment plus often a temporary low-sulfur diet.
- Sulfite oxidase deficiency — rare genetic disorder causing severe neurological disease in infancy. Sulfite oxidase requires the molybdenum cofactor (MoCo) plus molybdenum itself. Some patients with milder MoCo synthesis defects present in adulthood with sulfite sensitivity and accumulation.
- "Detox reactions" — aggressive initiation of detox protocols (high-dose NAC, glutathione, MSM, glycine, methylation cofactors) can precipitate symptoms attributed to "detox" reactions: fatigue, headache, GI upset, rash. Pragmatic management: titrate slowly, ensure binders (charcoal, chlorella, modified citrus pectin) are available, monitor for actual hepatic or renal stress.
- Drug interactions through sulfation competition — high-dose polyphenols (quercetin, resveratrol, EGCG, curcumin) compete for SULT enzymes and can alter clearance of acetaminophen, estrogens, dopamine. Significant for clinical pharmacology but rarely accounted for.
- Pregnancy — routine functional medicine "detox protocols" are generally avoided during pregnancy. Methylation cofactor support (folate, B12, choline) is established and recommended; aggressive sulfur supplementation is not.
- Chronic kidney disease — magnesium sulfate (Epsom salt) ingestion can be hazardous in advanced CKD due to magnesium accumulation. Baths are safer than oral use in this population.
This content is provided for informational purposes only and does not constitute medical advice. Consult a qualified healthcare provider before beginning detoxification protocols, especially in the context of underlying medical conditions, prescription medications, or pregnancy.
Key Research Papers
- Waring RH, Klovrza LV. (2000). Sulphur metabolism in autism. Journal of Nutritional & Environmental Medicine. — PubMed
- Alberti A, Pirrone P, Elia M, Waring RH, Romano C. (1999). Sulphation deficit in "low-functioning" autistic children: a pilot study. Biological Psychiatry. — PubMed
- Glatt H, Meinl W. (2004). Pharmacogenetics of soluble sulfotransferases (SULTs). Naunyn-Schmiedeberg's Archives of Pharmacology. — PubMed
- Klaassen CD, Boles JW. (1997). The importance of 3'-phosphoadenosine 5'-phosphosulfate (PAPS) in the regulation of sulfation. FASEB Journal. — PubMed
- Hayes JD, Flanagan JU, Jowsey IR. (2005). Glutathione transferases. Annual Review of Pharmacology and Toxicology. — PubMed
- Mitchell JR, Jollow DJ, Potter WZ, Davis DC, Gillette JR, Brodie BB. (1973). Acetaminophen-induced hepatic necrosis. I. Role of drug metabolism. Journal of Pharmacology and Experimental Therapeutics. — PubMed
- Wang R. (2002). Two's company, three's a crowd: can H2S be the third endogenous gaseous transmitter? FASEB Journal. — PubMed
- Kabil O, Banerjee R. (2010). Redox biochemistry of hydrogen sulfide. Journal of Biological Chemistry. — PubMed
- Yang G, Wu L, Jiang B, et al. (2008). H2S as a physiologic vasorelaxant: hypertension in mice with deletion of cystathionine gamma-lyase. Science. — PubMed
- Falany CN. (1997). Enzymology of human cytosolic sulfotransferases. FASEB Journal. — PubMed
- Strott CA. (2002). Sulfonation and molecular action. Endocrine Reviews. — PubMed
- Coughtrie MW. (2002). Sulfation through the looking glass — recent advances in sulfotransferase research for the curious. Pharmacogenomics Journal. — PubMed
PubMed Topic Searches
- PubMed: SULT phase II conjugation
- PubMed: PAPS universal sulfate donor
- PubMed: GST xenobiotic conjugation
- PubMed: H2S gasotransmitter signaling
- PubMed: Waring autism sulfation bottleneck
Connections
- Sulfur (Main Page)
- Sulfur Benefits Hub
- Sulfur for Joint Health
- Sulfur for Glutathione & Methylation
- Sulfur for Skin Health
- NAC (N-Acetylcysteine)
- Glutathione
- Cysteine
- Methionine
- Taurine
- Glycine
- Molybdenum for Detoxification
- Homocysteine
- Heavy Metals
- Oxidative Stress
- Detoxification
- Garlic
- Broccoli
- All Minerals