Sulfur Deficiency: What the Evidence Shows
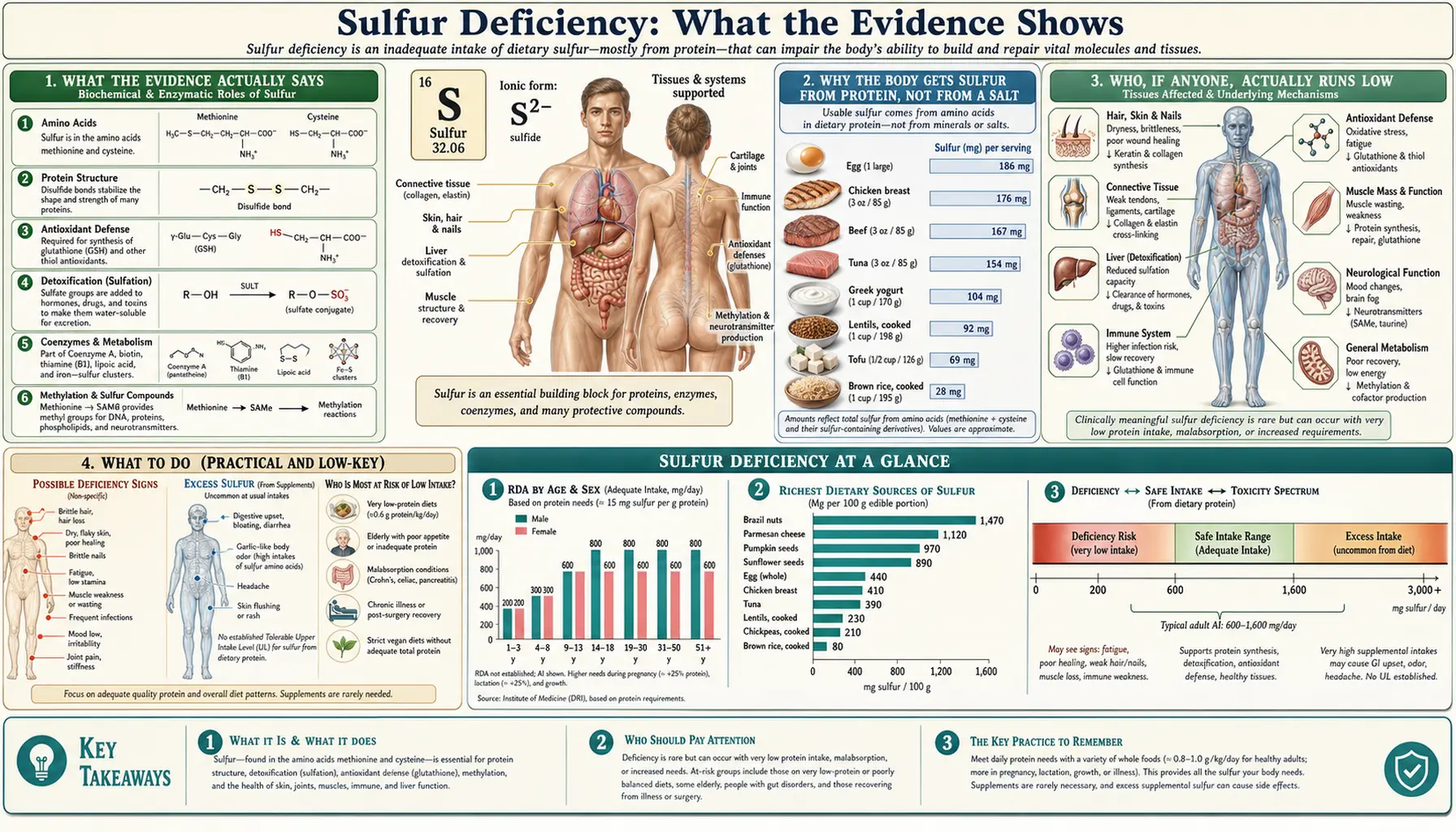
Here is the honest bottom line, stated up front: there is no recognized clinical syndrome called "sulfur deficiency." Sulfur is one of the most abundant minerals in the body, but you do not get it the way you get iron or calcium — there is no Recommended Dietary Allowance for elemental sulfur, no blood test for it, and no defined deficiency disease. The reason is that almost all of the sulfur your body uses arrives bound inside two amino acids — methionine and cysteine — which come from the protein in your food. In practical terms, your sulfur status simply tracks whether you are eating enough good-quality protein. A person eating adequate protein is not short of sulfur, and a person who is short of these amino acids is, by definition, short of protein — a problem doctors diagnose and treat as protein-energy malnutrition, not as a mineral deficiency. This page explains what the evidence actually says, why the biology works this way, the rare edge cases where sulfur amino acid supply genuinely runs low, and the simple, low-key thing to do about it — which is mostly to eat enough protein.
Table of Contents
- What the Evidence Actually Says
- Why the Body Gets Sulfur From Protein, Not From a Salt
- Who, If Anyone, Actually Runs Low
- What to Do (Practical and Low-Key)
- A Word on "Sulfur Deficiency" Claims and MSM
- Related Pages and Where to Read More
- Key Research Papers
- Connections
- Featured Videos
What the Evidence Actually Says
It is worth being candid about something the internet often gets wrong. You will find pages, products, and videos warning about an epidemic of "sulfur deficiency." The mainstream nutrition science does not recognize this. There is no defined human deficiency disease for elemental sulfur, no Dietary Reference Intake (DRI) for sulfur as a mineral, and no routine clinical test that measures your "sulfur level." This is not an oversight — it reflects how sulfur is actually handled in the body.
Sulfur is genuinely essential. By weight it is among the most plentiful elements in the body, after the obvious ones like calcium and phosphorus. It sits at the heart of proteins, of the master antioxidant glutathione, of connective tissue, and of countless enzymes. None of that is in dispute. What is settled is the route by which the body obtains it. As the major nutrition reviews put it, humans meet essentially all of their sulfur needs through the sulfur amino acids — methionine and cysteine — rather than from inorganic sulfur in food or water. Brosnan and Brosnan, in a widely cited overview of the sulfur-containing amino acids, frame methionine and cysteine as the body's working currency of sulfur; Stipanuk's reviews trace how the sulfur in dietary methionine is passed along to make cysteine and then everything downstream.
So the question "am I sulfur deficient?" almost always collapses into a different, well-understood question: "am I eating enough protein, and is it good-quality protein?" Methionine is an indispensable (essential) amino acid — the body cannot make it, so it must come from food. Cysteine is usually called conditionally dispensable: the body can manufacture it, but only by spending methionine to do so. Reeds' classic paper on dispensable and indispensable amino acids lays out exactly this kind of dependency. If protein intake is adequate, both amino acids — and therefore sulfur — are supplied in abundance, with the surplus simply broken down and the sulfur excreted in the urine as sulfate. If protein intake is grossly inadequate, the person has protein-energy malnutrition, which is diagnosed and treated as such; "sulfur deficiency" adds nothing to that picture.
Why the Body Gets Sulfur From Protein, Not From a Salt
It helps to see the plumbing. Picture sulfur arriving at a busy port not as loose cargo but pre-packed inside two shipping containers — methionine and cysteine. The body almost never unloads loose sulfur from the diet; it works with the containers.
The flow, in plain language, goes like this. You eat protein. Digestion releases its amino acids, including methionine and cysteine. Methionine does double duty: some is used directly to build new proteins, and some enters a hub called the methionine cycle, where it becomes S-adenosylmethionine (SAMe), the body's universal "methyl donor" that helps switch genes on and off and build many small molecules. After methionine donates its methyl group, what remains is homocysteine — and homocysteine can be permanently routed down the transsulfuration pathway, where its sulfur is handed off to make cysteine. Stipanuk's Annual Review of Nutrition paper on sulfur amino acid metabolism maps these pathways for producing and removing homocysteine and cysteine in detail. This is the key fact: the body makes its cysteine out of methionine's sulfur. That is why methionine is essential and cysteine is only conditionally so.
Cysteine is then the launch pad for nearly everything people associate with "sulfur." It is the rate-limiting building block of glutathione, the small molecule that does the bulk of the cell's antioxidant and detoxification work (Pizzorno and Katzinger review glutathione's physiological and clinical importance). Cysteine's sulfur also goes into taurine, into the iron-sulfur clusters that power energy metabolism, and into sulfate — which the body uses to "tag" hormones, drugs, and components of cartilage and connective tissue. Courtney-Martin and Pencharz trace this whole arc from protein synthesis through to glutathione. Importantly, the body tightly regulates this system based on supply: when cysteine is plentiful, the enzyme that disposes of it (cysteine dioxygenase) is turned up, and when cysteine is scarce it is turned down, so the body conserves what it has. Cresenzi and colleagues showed that cysteine itself is the metabolic signal driving this dietary regulation.
The upshot is that the body has no need for, and no machinery dedicated to, absorbing free elemental sulfur from the diet. It gets all the sulfur it requires by unpacking dietary protein. That single design choice is why "sulfur" does not behave like a classic dietary mineral and why there is no deficiency disease named for it.
Who, If Anyone, Actually Runs Low
Saying there is no recognized "sulfur deficiency" is not the same as saying sulfur amino acid supply can never run short. It can — but the situations are specific, uncommon, and almost always recognized first as protein problems or as defined medical conditions. Being honest about these edge cases is more useful than either inventing a syndrome or pretending shortage is impossible.
- Protein-energy malnutrition. This is the real-world face of "not enough sulfur amino acids." In severe undernutrition — famine, anorexia nervosa, advanced illness, neglect — intake of all essential amino acids, methionine included, falls short. The clinical problem is malnutrition, and it is diagnosed and treated as such. Nimni, Han, and Cordoba argued in Nutrition & Metabolism that some older adults eating low-protein diets may take in less methionine and cysteine than is ideal for making glutathione — an interesting hypothesis about diet quality, but again a protein-adequacy issue, not a stand-alone mineral deficiency.
- Total parenteral nutrition (TPN) in newborns. Cysteine is unstable in intravenous feeding solutions, and very premature infants have an immature transsulfuration pathway and so make cysteine poorly from methionine. For this narrow group, cysteine is treated as effectively essential and is sometimes added to their IV nutrition. This is the clearest genuine example of a clinically managed sulfur amino acid shortfall — and it is a hospital matter, not something that applies to healthy people.
- Severe liver disease. The transsulfuration enzymes that convert methionine to cysteine live largely in the liver. In advanced liver failure this conversion can falter, which is part of why cysteine and its products can become limiting in some patients with serious liver disease.
- Rare inborn errors of metabolism. A handful of genetic enzyme deficiencies disturb sulfur amino acid metabolism — for example homocystinuria (a block in transsulfuration that causes homocysteine to build up) and molybdenum-cofactor or sulfite-oxidase deficiency (which disrupt the final disposal of sulfur). These are serious, individually rare conditions managed by metabolic specialists, and they are problems of processing sulfur, not of dietary lack.
- Very low-protein therapeutic or fad diets. Medically supervised low-protein diets (used in some kidney disorders) and extreme self-imposed low-protein eating can, in theory, narrow the margin of sulfur amino acid intake. In practice this is monitored as protein adequacy by the clinician overseeing the diet.
Notice the common thread: every real scenario is either frank protein malnutrition or a specific, named disease of metabolism. None of them is a free-standing "sulfur deficiency" that an otherwise well-fed adult develops and self-treats. That distinction matters, because it points anyone with vague symptoms toward the right evaluation rather than toward an imaginary diagnosis.
What to Do (Practical and Low-Key)
Because there is no sulfur deficiency syndrome to chase, the practical advice is refreshingly simple and not at all alarming: eat enough good-quality protein, and your sulfur needs take care of themselves. The sulfur amino acids are concentrated in exactly the foods you would expect to supply protein.
- Animal proteins are the richest, most reliable source. Methionine and cysteine are abundant in eggs (egg protein is a classic reference for sulfur amino acid quality), in meat, poultry, and fish, and in dairy. If you eat these in normal amounts, you are comfortably covered.
- Plant sources work too — with a little more attention. Many legumes are relatively lower in methionine, while grains, nuts, and seeds tend to be higher in it. Eating a variety across the day (the familiar "beans plus grains" idea) supplies the full set. Whole-food, sulfur-rich vegetables such as broccoli and other cruciferous vegetables, and the allium family like onions and garlic, contribute additional sulfur compounds — valued more for their plant chemistry than as a way to prevent any deficiency.
- You do not need a "sulfur supplement" to meet a requirement. There is no requirement set for elemental sulfur to meet. Supplements such as MSM (methylsulfonylmethane) or N-acetylcysteine are sometimes taken for specific reasons (see the next section and the linked pages), but they are not treatments for a deficiency that mainstream medicine recognizes.
- If you are worried about your protein intake, that is the useful question to ask — and to act on. Older adults, people recovering from illness, those with poor appetite, and people on restrictive diets are the groups most likely to fall short on protein generally. A dietitian or doctor can assess protein adequacy; there is no separate "sulfur test" to order. A standard comprehensive metabolic panel includes total protein and albumin, which speak to overall protein-nutrition status far better than any sulfur measurement could.
In short: this is not a problem to manage with a mineral. It is, at most, a reminder to eat enough protein — advice that is good for many reasons and that quietly settles the sulfur question along the way.
A Word on "Sulfur Deficiency" Claims and MSM
A fair amount of the "sulfur deficiency" messaging online exists to sell MSM (methylsulfonylmethane), an organic sulfur compound. It is worth separating two different claims so you can weigh them honestly.
The first claim — that modern diets cause widespread sulfur deficiency, so people need supplemental MSM to correct it — is not supported. As covered above, there is no recognized deficiency state, and protein-eating people are not short of sulfur. MSM does deliver bioavailable sulfur, but "delivering sulfur" is not the same as "correcting a deficiency" when no deficiency exists.
The second, narrower claim — that MSM may help symptoms such as joint pain in osteoarthritis — rests on a different kind of evidence and should not be confused with the deficiency argument. Small trials have looked at this. Kim and colleagues ran a pilot randomized trial in knee osteoarthritis and reported modest improvements in pain and function with MSM over placebo. A systematic review by Brien and colleagues of MSM and the related compound DMSO concluded the data were promising but limited, with studies generally short and small, so firm conclusions were not yet warranted. In other words, MSM may have a role as a symptom-oriented supplement for some people — a question of efficacy for a condition — which is wholly separate from the false premise that you are deficient in sulfur. If MSM interests you, read about it on its own terms rather than as a deficiency cure; see the joint-health discussion linked below.
Related Pages and Where to Read More
Because sulfur in the body is really the story of its amino acids, the most useful further reading is on methionine and cysteine themselves, and on the molecules cysteine builds.
- Methionine — the essential sulfur amino acid that is the body's entry point for dietary sulfur and the precursor of cysteine. Start here to understand sulfur intake.
- Cysteine — the conditionally essential amino acid made from methionine's sulfur and the direct building block of glutathione, taurine, and sulfate.
- Glutathione and N-Acetylcysteine (NAC) — the master antioxidant and a cysteine-delivering supplement; this is where most of the cysteine-and-sulfur health interest actually lands.
- Sulfur, Glutathione & Methylation and Sulfur and Joint Health — the legitimate biology of what sulfur does, including the MSM/joint discussion in proper context.
- Sulfur (overview) and the Sulfur Toxicity hub — the companion pages to this one.
Key Research Papers
- Brosnan JT, Brosnan ME (2006). The Sulfur-Containing Amino Acids: An Overview. The Journal of Nutrition;136(6):1636S-1640S. — DOI: 10.1093/jn/136.6.1636S
- Stipanuk MH (2004). Sulfur Amino Acid Metabolism: Pathways for Production and Removal of Homocysteine and Cysteine. Annual Review of Nutrition;24:539-577. — DOI: 10.1146/annurev.nutr.24.012003.132418
- Reeds PJ (2000). Dispensable and Indispensable Amino Acids for Humans. The Journal of Nutrition;130(7):1835S-1840S. — DOI: 10.1093/jn/130.7.1835S
- Stipanuk MH, Dominy JE, Lee JI, Coloso RM (2006). Mammalian Cysteine Metabolism: New Insights into Regulation of Cysteine Metabolism. The Journal of Nutrition;136(6):1652S-1659S. — DOI: 10.1093/jn/136.6.1652S
- Cresenzi CL, Lee JI, Stipanuk MH (2003). Cysteine Is the Metabolic Signal Responsible for Dietary Regulation of Hepatic Cysteine Dioxygenase and Glutamate Cysteine Ligase in Intact Rats. The Journal of Nutrition;133(9):2697-2702. — DOI: 10.1093/jn/133.9.2697
- Courtney-Martin G, Pencharz PB (2016). Sulfur Amino Acids Metabolism From Protein Synthesis to Glutathione. In The Molecular Nutrition of Amino Acids and Proteins;265-286. — DOI: 10.1016/B978-0-12-802167-5.00019-0
- Nimni ME, Han B, Cordoba F (2007). Are we getting enough sulfur in our diet? Nutrition & Metabolism;4:24. — DOI: 10.1186/1743-7075-4-24
- Pizzorno JE, Katzinger JJ (2012). Glutathione: Physiological and Clinical Relevance. Journal of Restorative Medicine;1(1):24-37. — DOI: 10.14200/jrm.2012.1.1002
- Kim LS, Axelrod LJ, Howard P, Buratovich N, Waters RF (2006). Efficacy of methylsulfonylmethane (MSM) in osteoarthritis pain of the knee: a pilot clinical trial. Osteoarthritis and Cartilage;14(3):286-294. — DOI: 10.1016/j.joca.2005.10.003
- Brien S, Prescott P, Bashir N, Lewith H, Lewith G (2008). Systematic review of the nutritional supplements dimethyl sulfoxide (DMSO) and methylsulfonylmethane (MSM) in the treatment of osteoarthritis. Osteoarthritis and Cartilage;16(11):1277-1288. — DOI: 10.1016/j.joca.2008.03.002
- Methionine restriction and longevity research (life-span and metabolic effects of dietary sulfur amino acid restriction). — PubMed
PubMed Topic Searches
- PubMed — Sulfur amino acid requirements in humans
- PubMed — Methionine, cysteine, and dietary protein metabolism
- PubMed — Cysteine, parenteral nutrition, and the preterm infant
- PubMed — Glutathione synthesis and cysteine availability
- PubMed — MSM and osteoarthritis clinical trials
Connections
- Sulfur Overview
- Sulfur Toxicity Hub
- Sulfur Benefits Hub
- Sulfur, Glutathione & Methylation
- Sulfur and Joint Health
- Sulfur and Detoxification
- Methionine
- Cysteine
- Taurine
- Amino Acids (overview)
- Glutathione
- N-Acetylcysteine (NAC)
- Comprehensive Metabolic Panel
- Selenium
- Magnesium
- Minerals (overview)
- Eggs
- Beef
- Broccoli
- Onions